Stages of bite formation in children
The process of developing a child’s bite can be divided into several important stages.
Each of them is characterized by changes in the structure of the jaw and has factors that influence the formation of pathology. Stages of bite development in children:
- Elementary.
From birth to six months of the child. The first teeth begin to erupt towards the end of the period. The cause of pathology at this stage is a genetic predisposition or improper latching of the nipple during breastfeeding. - The process of formation of the bite of primary teeth.
Lasts until the age of three; as a rule, by the end of the period, all 20 baby teeth are in their position. At this age, the presence of gaps between the teeth is acceptable, but twisting, too close a fit, and growth in an uncharacteristic plane are considered as deviations from the norm. In addition to the above reasons, the most common factor in the development of pathology is bad habits: thumb sucking, pacifiers, toys or eating disorders. The child's diet should include a sufficient amount of solid food. - Preparation for the development of permanent dentition.
The stage continues until the appearance of the first permanent teeth. With proper oral care, no external changes are observed during this period. Bad habits can cause malocclusion. It is necessary to ensure that the child does not chew hard objects: pencils, thick books, furniture, since baby teeth are very soft and easily deformed. - Changing the temporary bite to a permanent one.
The most critical stage. It is during this period that serious pathologies begin to manifest themselves as unpleasant changes: torsion, improper growth of teeth, discrepancy between the size of the jaw and the volume of bone units, etc. On average, this period lasts up to 12 years. Factors in the development of anomalies are physiological characteristics or untimely replacement of teeth. - Formation of a permanent bite.
The teeth complete their growth and occupy a certain position in the jaw.
You can start correcting your bite from the early stages. There are several hardware and manual methods for this. Treatment with braces begins after a permanent bite has formed.
When should an x-ray be taken?
For children, this study is most often performed in cases of trauma, including birth trauma. Often this is the only method that helps identify life-threatening pathologies. The following doctors can refer you for this procedure: oncologist, neurologist, traumatologist, surgeon, ophthalmologist, endocrinologist. Symptoms and indications for examination are:
- headache;
- tremor (shaking) of hands;
- nosebleeds;
- darkening of the eyes;
- dizziness;
- decreased vision or hearing;
- fainting;
- facial asymmetry;
- suspicion of a malignant tumor;
- recent injury;
- some endocrine diseases;
- congenital pathologies.
Pictures are also taken during treatment to monitor the effectiveness of the therapy.
Signs of malocclusion
For timely detection of maxillofacial defects, it is necessary to regularly examine the baby’s oral cavity. Here are a few signs by which you can identify a malocclusion in a child:
- obvious displacement of the lower jaw outward or inward;
- crooked, uneven teeth;
- vestibular or lingual growth of teeth - in front or behind the main row;
- diastema - spaces between the incisors;
- strong overlap of the lower teeth with the upper ones;
- non-closure of the upper and lower incisors with a formed bite;
- half-open mouth, replacement of nasal breathing;
- speech defects.
Signs of malocclusion
In addition to the visible signs, if you look closely, you can notice abrasion of the enamel on the front or back teeth, and gum injuries. The child complains of tension in the jaw muscles, difficulty chewing or swallowing food, and headache. These signs will help you understand that your child has a malocclusion and seek advice from an orthodontist.
Mouth breathing
If you find that your child predominantly breathes through his mouth or snores at night, I advise you to immediately contact an ENT doctor first and foremost. Orthodontic measures for oral breathing in children can begin at 3-4 years of age. Mouth breathing in children leads to a violation of the position of the tongue: the tongue moves down the oral cavity and ceases to occupy the desired position. So it does not have a stimulating effect on the upper jaw - and it does not develop to the required extent. As a result, there is not enough space for permanent teeth, and they begin to grow unevenly. In addition, a narrow upper jaw can cause a habitual lateral displacement of the lower jaw. A crossbite and facial asymmetry will form. When dealing with mouth breathing, it is important to work in conjunction with an ENT doctor and often with a speech therapist. In some cases (for example, if the cause of mouth breathing is allergic rhinitis), we also involve an allergist. The task of the ENT doctor is to normalize the patency of the airways so that the child can physically breathe through the nose. Next, the orthodontist and speech therapist are included in the work. A speech therapist works with the muscles of the lips and tongue to train them and teach them to work normally. The orthodontist eliminates the effects of mouth breathing and can also prescribe myogymnastics - training for the muscles of the lips, cheeks, and tongue.
Types of malocclusion
The curvature of the teeth does not always mean a pathology of the bite, which is understood as the closing of the jaws, ensuring the full, unhindered functioning of the masticatory apparatus.
Among the types of malocclusion in children are:
- Prognathia – distal occlusion.
This is a common reason for visiting an orthodontist in early childhood. The muscles of the lower jaw are not yet sufficiently developed, so outwardly it seems that the upper row of teeth protrudes strongly forward compared to the lower one. With the introduction of hard foods into the diet: hard fruits and vegetables, the problem may disappear without medical intervention. - Progenia – mesial occlusion.
At an early age, this pathology is usually caused by genetic characteristics or improper latching of the nipple during feeding. The sooner the pathology is identified and treatment is prescribed, the fewer negative consequences the child will receive. - Deep bite.
Parents often confuse it with the distal one, however, with a deep bite, the lower jaw does not go back, but seems to sink inside. The upper front incisors overlap the lower ones by more than half. Obvious signs of pathology are speech defects and soft tissue injuries. - Crossbite.
It appears at the stage of replacement of milk teeth with molars. In this case, on the one hand, the upper jaw overlaps the lower jaw, on the other, the lower teeth come to the fore. - Open bite.
With this malocclusion pathology, there is a noticeable lack of closure between the teeth of the upper and lower rows. Most often, this disorder affects the incisors, but it also occurs on the posterior premolars and molars.
Types of Malocclusions
Malocclusions in children are diagnosed during annual examinations. It is important not to waste time and immediately begin preventive or therapeutic treatment.
Asymmetry in the face, smile, bite
If you notice any signs of asymmetry in a child, this is a reason to immediately consult a doctor. At any age of the child - as soon as noticed. Of course, all people are naturally asymmetrical. But natural asymmetry is not visible to the eye and does not attract attention. What you need to pay attention to in terms of asymmetry: • displacement of the chin to the side • the smile is not symmetrical • the central lines of the upper and lower jaws do not coincide (with each other and with the central line of the face). The orthodontist will be able to conduct an examination and prescribe the necessary treatment or examination to identify the causes of asymmetry.
Photos of children with pathological bite
In the presented images you can see the child’s malocclusion. The photo shows various pathologies that are often found in patients with baby or molar teeth. Detailed photographs of children with malocclusion captured in the photo during an orthodontic consultation will help parents in self-diagnosis of the pathology. However, the doctor chooses the effective therapy regimen.
Photo of a girl with an incorrect open bite
Photo of a child with an incorrect deep bite
Photo of a boy with an incorrect deep distal bite
The boy has an open bite
The girl has a deep distal bite
How to correct a child's bite
No matter how severe the pathology, the earlier treatment is started, the easier it is to achieve an effective result. To correct violations, there are three ways to correct bite in children:
- traditional – installation of braces;
- alternative (without braces) – mouth guards, plates, physiotherapy;
- cardinal – surgical intervention.
Until the final stage of permanent bite formation, only alternative methods are used, but is it possible to correct a child’s malocclusion with their help?
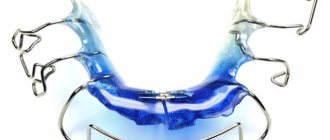
Removable orthodontic plates
Orthodontic plates
are structures consisting of a polymer jaw-expanding base and metal arches that serve to fix the plate and align the front row of teeth.
Removable orthodontic plate
These devices are made individually, based on casts of the jaw of a small patient. To adjust the load, the devices are equipped with screws and expanders. At an appointment with a doctor, the child’s parents will learn how to perform this procedure on their own, which will save time on visits to the orthodontist.
Plates for correcting malocclusion in children are designed to be worn constantly, but the removable structures are removed during meals or hygiene procedures.
Trainers for teeth
Trainers
To correct malocclusion in children, they are mouth guards made of dense silicone.
Trainer for correcting the bite
The trainer performs several functions:
- Self-corrects minor pathologies.
- Prevents further development of malocclusion and prevents complications.
- Helps get rid of bad habits that have caused crooked teeth.
Mouth guards for correcting malocclusion in children fix both jaws simultaneously in the correct position. But when using them, it is impossible to lead a normal lifestyle: talking, eating. Therefore, mouthguards are worn while the child is sleeping and for several hours during the day.
The process of correcting a bite with trainers is long and requires patience from the child and parents.
It has been noticed that in children who regularly use trainers before installing braces, the effect of therapy occurs faster.
Myotherapy
Myogymnastics
in orthodontics, it is a set of exercises to relax or develop individual facial muscles.
Myotherapy in orthodontics
The method serves as both a primary and an auxiliary method of occlusion correction. For each type of pathology there is its own set of exercises. The first lessons are carried out under the supervision of an orthodontist; as soon as the child learns to do gymnastics correctly, he continues to work at home independently or with his parents.
Conditions for performing exercises to correct bite in children:
- Systematicity and regularity.
- Sufficient application of force without jerking or pressure. The muscles feel resistance, but are not overloaded.
- Cyclicality. Exercises are performed in several approaches to achieve good results.
- Gradual increase in load and intensity.
Myotherapy is especially effective in correcting occlusion in combination with physiotherapy: electrophoresis, vibration massage, ultrasound, vacuum therapy, massage.
Alternative methods can correct mild pathologies of malocclusion in early childhood or slow down the development of complications and wait until the formation of the jaw is completed to begin basic treatment.
Braces
Braces
– the main way to correct uneven teeth and malocclusion in children from 12–16 years old and adults of any age.
Braces for correcting bite
They are a system of clasps fixed on the outer or inner surface of the teeth and a steel arch stretched between them.
Under the pressure of the arch, the teeth are aligned and placed in the correct position. With the help of braces, it is possible to correct almost all malocclusion pathologies. Treatment takes from 6 to 18 months and ends with the acquisition of a beautiful, even smile.
Treatment of malocclusion in children of different ages
Anomalies in jaw development and tooth growth cannot be ignored. Early childhood is not a reason to refuse correction. The orthodontist will help you choose the most effective treatment method. The use of alternative therapy methods can completely restore jaw function or prevent the occurrence of health-threatening complications.
Let's look at how malocclusion is treated in children of different ages.
Children under one year old
At this age, parents' actions should be aimed at preventing the development of jaw pathologies. Effective measures include:
- maintaining the correct position of the head during feeding, it does not tilt back, the chin is not pressed against the baby’s chest, make sure that the nipple is grasped correctly;
- the use of orthodontic pacifiers that imitate the female nipple and promote the correct position of the jaws when sucking;
- preventing the development of bad habits;
- introduction of solid food into the diet with the appearance of the first teeth;
- adequate consumption by mother and child of foods containing fluoride and calcium or vitamin supplements designed specifically for nursing women;
- preventive examination at the dentist.
Most often, malocclusion in a child of the first year of life develops due to the use of a low-quality pacifier, so the choice of this accessory is very important.
Children from 1 to 2 years old
There are often questions from worried parents on the Internet: “My child is one year old, it seems that he has the wrong bite, what should I do?” First of all, if you suspect the development of pathology, you need to show the baby to a specialist. He will determine whether the feature is an age-related norm or a complication.
Malocclusion in a 1-year-old child occurs as a result of dysfunction of sucking (and then chewing). At such an early age, hardware correction methods are not yet available, so physiotherapy and the use of orthodontic pacifiers, which return the jaw to its normal position, are most often prescribed.
To correct malocclusion in a child 2 years of age and older, Hintz plates are used, which are similar in shape to a pacifier, but instead of a pacifier, a flap is placed in the mouth and clamped between the teeth. The longer the device is used, the faster the bite is corrected and bad habits are eliminated.
Children from 3 to 5 years old
Malocclusion in a 3-year-old child is corrected with special caps for correcting the position of the jaw, which are worn at night. You can also continue therapy using Hintz plates.
Another accessible method at this age is myogymnastics. A three-year-old child can easily cope with the exercises.
From 4 years of age it is allowed to use LM activators under the supervision of an orthodontist. And malocclusion in a 5-year-old child is corrected with the help of trainers and orthodontic plates.
The first thing to do when malocclusion is detected is to show the child to a qualified orthodontist.
Children from 6 to 14 years old
Malocclusion in a 6-year-old child should cause the greatest concern for parents, since when baby teeth are replaced, this pathology will certainly affect the growth of permanent bone units.
Therefore, careful adherence to the dentist's recommendations is necessary. At this age, all alternative methods are available; the doctor will select the most effective one.
Lack of distances between teeth at the age of 5-5.5 years.
At the age of 5-5.5 years, the jaws should already be very actively preparing for the replacement of milk teeth with permanent ones. The jaws must grow - after all, permanent teeth are wider than baby teeth, they will need more space. Gaps should appear between primary teeth - both on the upper and lower jaws. If you notice that your child's baby teeth are tightly spaced and there is no space between them, this indicates that there will not be enough space for the permanent teeth to erupt and they will begin to grow unevenly.
These signs will help you identify problems in your child’s bite development in the early stages. in this case, the orthodontic correction will be shorter and simpler. And in some cases, a problem noticed in time can prevent orthodontic treatment in the future.
Causes of malocclusion
Many factors influence jaw development. Among the main reasons for the formation of malocclusion in children are:
- heredity;
- incorrect position during breastfeeding, incorrect grip of the nipple or bottle nipple;
- bad habits;
- physiological features, for example, a narrow jaw;
- late transition to solid food;
- ENT diseases;
- metabolic disorders, lack of microelements;
- incorrect posture;
- intrauterine developmental pathologies;
- early loss of baby teeth or delayed loss of teeth;
- accompanying illnesses.
The habit of thumb sucking can cause malocclusion.
Before starting treatment, you need to make sure that the factor that caused the pathology no longer has an effect.
Correcting a child’s malocclusion without eliminating the cause is ineffective.
Consequences
What complications can arise if a child’s malocclusion is not corrected? Possible consequences:
- tooth abrasion, premature wear, increased risk of caries;
- difficulty chewing causes gastrointestinal problems;
- mucosal injuries, gum inflammation, periodontal disease;
- increased load on the temporomandibular joint, pain, inflammation;
- breathing problems, ENT diseases;
- pinched nerves in the cervical spine;
- aesthetic facial defects, asymmetry;
- psychological problems;
- violation of diction.
Thus, malocclusion in children is dangerous for the development of diseases. It directly affects the emotional state of the individual, self-esteem, and self-confidence. If the bite is not corrected in time, physiological, psychological and aesthetic problems may develop.
Prevention
Prevention of the development of malocclusion in children begins at an early age. By following simple recommendations, you can avoid problems and maintain your baby’s beautiful smile.
Dentists' advice:
- Correct attachment to the breast or bottle. Usually a new mother will be helped with this by a pediatric nurse or a breastfeeding specialist.
- Prevent the development of bad habits, gradually abandon the pacifier when the first teeth appear.
- Supplement your diet with solid food in a timely manner.
- Keep your mouth clean.
- Perform gymnastics to develop facial muscles.
The effectiveness of preventive measures can be monitored by a local dentist, whose consultation is recommended for children at least once a year.
The health of a child’s teeth affects not only the appearance, but also the functioning of the entire body. Incorrect bite is the cause of serious illnesses. Therefore, it is important to identify pathologies in time and correct them using methods available for a given age.
How is the procedure carried out?
Children undergo the examination lying or sitting. There should be no metal objects on the head. Sometimes you need to stand while taking a photo; this is discussed separately. Below the head, the child’s body is covered with personal protective equipment. Pictures are taken in frontal or lateral projection. It is important not to move during the examination. Therefore, soft restraints are used for the smallest children, and sedation is sometimes used. Such measures allow the procedure to be carried out quickly and almost without harm. Sometimes a child calms down thanks to the presence of one of the parents in the office.
Contraindications
Radiography has no significant contraindications unless alternative diagnostic techniques are found with similar information content but less radiation exposure. It is worth discussing the restrictions with the doctor if the child has recently had an x-ray.
Is the procedure harmful?
Ionizing radiation is harmful, especially for a growing organism. Therefore, it is better to do the procedure for a fee and in a clinic with modern equipment. The device used in the SM-Clinic provides a minimum radiation dose: from 0.03 to 0.1 mSv (for children, the permissible radiation exposure is 1 mSv per year). It is also important that the digital technologies used now make it possible to take a picture very quickly, that is, to influence the body with radio radiation for the shortest possible time - up to 1 second. The procedure is practically harmless if it is carried out all the time in the same medical center with the radiation doses received by the child throughout the year recorded in the outpatient card.