9218
This term originates from Latin and means “closure.”
Central occlusion is a state of evenly distributed tension of the jaw muscles, while ensuring simultaneous contact of all surfaces of the elements of the dentition.
The need to determine central occlusion is to correctly manufacture a partial or removable denture.
Main features
Experts have determined the following indicators of central occlusion:
- Muscular. Synchronous, normal contraction of the muscles responsible for the functioning of the lower jaw bone.
- Articular. The surfaces of the articular heads of the lower jaw are located directly at the bases of the slopes of the articular tubercles, in the depths of the articular fossa.
- Dental:
- full surface contact;
- opposite rows are brought together so that each unit is in contact with the same and the next element;
- the direction of the upper frontal incisors and the similar direction of the lower ones lie in a single sagittal plane;
- the overlap of the elements of the upper row of fragments of the lower one in the front part is 30% of the length;
- the anterior units contact in such a way that the edges of the lower fragments abut the palatine tubercles of the upper ones;
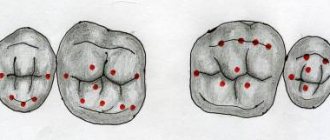
- the upper molar comes into contact with the lower one so that two-thirds of its area is combined with the first, and the rest with the second;
If we consider the transverse direction of the rows, then their buccal tubercles overlap, while the tubercles on the palate are oriented longitudinally, in the fissure between the buccal and lingual of the lower row.
Signs of correct row contact
Are common:
- the rows converge in a single vertical plane;
- incisors and molars of both rows have a pair of antagonists;
- there is contact between units of the same name;
- the lower incisors do not have antagonists in the central part;
- the upper eighths have no antagonists.
Applies to anterior units only:
- if we conditionally divide the patient’s face into two symmetrical parts, then the line of symmetry should pass between the front elements of both rows;
- the upper row of fragments overlaps the lower one in the anterior zone to a height of 30% of the total crown size;
- the cutting edges of the lower units are in contact with the tubercles of the inner part of the upper ones.
Applies only to lateral ones:
- the buccal distal cusp of the upper row is based in the space between the 6th and 7th molars of the lower row;
- the lateral elements of the upper row close with the lower ones in such a way that they fall strictly into the intertubercular grooves.
Let's find out together how dental impressions are made and what modern material is used.
Read here about the purpose of filing the front teeth.
At this address https://orto-info.ru/ortodonticheskoe-lechenie/podgotovitelnyiy-period/separatsiya-zubov.html we will talk about the consequences of teeth separation.
Signs of occlusion
The main signs of central occlusion are:
- muscular;
- articular;
- dental
In the latter case, it is necessary to determine what the surface contact will be and whether it is complete. It is necessary to determine how exactly the opposite rows are brought together, if there are any violations, what kind of overlap is for the top row. Also, when determining occlusion, the specialist looks at whether the upper molar comes into full contact with the lower molar, whether there is a coincidence or displacement.
Methods used
Central occlusion is determined at the stage of manufacturing prosthetic structures when several units are lost.
This is necessary to ensure the normal functioning of the product and eliminate the occurrence of deviations and problems in the functioning of the temporomandibular joints.
In this case, the height of the lower third of the face is of great importance. However, in the absence of a large number of units, this indicator may be violated and must be restored.
If the patient has partial adentia, several options for determining the indicator are used.
The presence of antagonists on both sides
The method is used when antagonists are present in all functional areas of the jaws.
In the presence of a large number of antagonists, the height of the lower third of the face is maintained and fixed.
The occlusion index is determined based on as many contact zones as possible of the same units of the upper and lower rows.
This option is the simplest, as it does not require the additional use of occlusal ridges or specialized orthopedic templates.
Presence of three occlusion points between antagonists
This method is used if the patient still has antagonists in the three main contact zones of the rows. At the same time, the small number of antagonists does not allow normal positioning of plaster casts of the jaw in the articulator.
In this case, the natural height of the lower third of the face is disrupted, and occlusal ridges made of wax or thermoplastic polymer are used to correctly match the casts.
The roller is placed on the bottom row, after which the patient brings his jaw together. After the roller is removed from the oral cavity, imprints of the antagonist contact zones remain on it.
These prints are subsequently used by technicians in the laboratory to position the casts and create a fully functional and correct, from an orthopedic point of view, prosthesis.
Absence of antagonistic pairs
The most labor-intensive scenario is the complete absence of the same elements on both jaws.
In this situation, instead of the position of central occlusion, the central relationship of the jaws is determined .
The procedure includes the following steps:
- Work on the formation of a prosthetic plane , which is positioned along the chewing surfaces of the lateral units and is parallel to the beam. It is built from the lower point of the nasal septum to the upper edges of the ear canals.
- Determination of the normal height of the lower third of the face.
- Fixation of the mesiodistal relationship of the upper and lower jaws using wax or polymer bases with occlusal ridges.
Checking central occlusion with existing pairs of elements of the same name is carried out by closing the teeth and is carried out as follows:
- a thin strip of wax is placed on the already prepared and fitted contact surface of the occlusal roller and glued;
- the resulting structure is heated until the wax softens;
- heated templates are placed in the patient’s oral cavity;
- After bringing the jaws together, the teeth leave imprints on the wax strip.
It is these fingerprints that are used in the process of modeling central occlusion in the laboratory.
If, during the process of determining occlusion, the surfaces of the upper and lower rollers close, the specialist adjusts their contact surfaces.
Wedge-shaped cuts are made on the upper one, and a certain amount of material is cut off from the lower one, after which a wax strip is glued to the treated surface. After the rows are brought together again, the strip material is pressed into the cutouts.
The products are removed from the patient’s mouth and sent to the laboratory for subsequent production of a prosthesis.
News
Determination of the centric relation of the jaws
The clinical stage of determining the centric relation during prosthetics of edentulous jaws consists of the following substages: 1) Preparation of the occlusal ridges. When preparing occlusal ridges, the following operations are performed: a) clarifying the boundaries of the wax templates; b) formation of the vestibular surface and thickness of the upper ridge; c) determining the height of the upper occlusal ridge; d) formation of a prosthetic plane; e) fitting the lower roller to the upper one. 2) Clarifying the boundaries of the occlusal ridge is to eliminate obstacles to its fixation on the prosthetic bed and prevent deformations of the upper lip. To do this, you should check all the boundaries of the wax template, freeing from it the frenulum of the lips, cheeks and tongue, the lateral folds of the mucous membrane, the pterygomaxillary folds, and sometimes shorten the base along line “A”. 3) The formation of the vestibular surface and the thickness of the upper occlusal ridge in the anterior section is dictated by the following circumstances. Atrophy of the alveolar part after tooth loss does not manifest itself in the same way everywhere. Thus, in the lower jaw, the bone decreases primarily from the apex and lingual surface of the alveolar ridge. On the upper jaw, on the contrary, the bone decreases from the top of the ridge and its vestibular surface. At the same time, the alveolar arch narrows, the conditions for setting teeth worsen, and in the anterior part a retraction of the upper lip occurs, giving the face an senile appearance. Therefore, the occlusal ridge in the anterior part of the upper jaw must be made taking into account the changes in the alveolar process that have occurred. In order for the patient’s appearance to be restored, sometimes it is not enough to position the occlusal ridge along the alveolar arch, but it is necessary to increase its vestibular surface in the anterior section. 4) When determining the height of the upper occlusal ridge, be guided by the following. When the mouth is closed, the cutting edges of the central upper incisors coincide with the line where the lips close, and when speaking, their edges protrude from under the upper lip by 1.0-2.0 mm. A person looks older than his age if the cutting edges of the upper incisors are not visible when smiling. Guided by these considerations, the height of the upper occlusal ridge is determined. After inserting the template into the oral cavity, ask the patient to close his lips. In this position, a line of lip closure is applied to the roller and its height is established along it. If the edge of the roller is located below the closure line, it should be shortened, if higher, it should be extended with a strip of wax. In this case, its edge should protrude 1.0-2.0 mm from under the upper lip.
5) Formation of the prosthetic plane. After determining the height of the upper occlusal ridge, they proceed to the formation of a prosthetic (occlusal) plane, which corresponds in the anterior part to the pupillary line, and in the lateral part to the nasal line. For this, two rulers are used. To determine the prosthetic plane in the anterior region, one ruler is installed on the occlusal surface of the roller, the other on the pupillary line. The parallelism of these rulers indicates the correct formation of the occlusal (prosthetic) plane in this section. Then a prosthetic plane is formed in the lateral sections, running parallel to the Camper horizontal, which on the face corresponds to the nasal line connecting the base of the nasal wing with the middle of the tragus of the ear. To check the correctness of its direction, as in the first case, use two rulers. One is installed on the occlusal surface of the roller, the other along the nasal line. The parallelism of the rulers indicates the correctness of the prosthetic plane. If there is no parallelism, then it should be created by adding or removing wax, depending on the need. The prosthetic plane serves as a guide for the dental technician for the correct installation of the staging glass, which will later be used to construct the upper dentition. After the formation of the prosthetic plane, the upper roller becomes untouchable. 6) Fitting the lower roller to the upper one. In this case, they achieve tight closure of the ridges in the anteroposterior and transversal directions and the location of their buccal surfaces in the same plane. Corrections that may be necessary in this case are made only (!) on the lower roller. With well-fitted rollers, the occlusal surfaces fit tightly to each other throughout their entire length. When closing the mouth, they simultaneously come into contact both in the anterior and lateral sections. Non-simultaneous closure is eliminated by building up or removing wax in the corresponding sections of the lower roller. The buccal surfaces of the roller should lie in the same plane.
All noticed deficiencies are eliminated, and corrections are made only on the lower, and not on the upper, roller. The latter is not corrected, since its prosthetic plane and orientation lines subsequently serve as landmarks for setting teeth. After fitting the occlusal ridges, they proceed to determining the interalveolar height. 7) Determining the height of the bite or the lower part of the face affects the appearance of the patient. The best aesthetic and functional effect of prosthetics is achieved by optimally setting the height of the lower part of the face. To determine the height of the lower part of the face, there are three methods: anatomical, anthropometric and anatomical-physiological. The anatomical method is based on restoring the correct configuration of the patient's face. The anthropometric method is based on the principle of proportionality of parts of the human body and, in particular, individual parts of the face. The height of the lower section is established, according to this method, using Heringer’s “golden” section compass, as well as the Wadsworth-White and Gysi method. The golden section compass consists of two compasses. They are connected in such a way that the legs of the large compass are separated in the extreme and middle ratios. Only on one leg the larger segment is located closer to the hinge, and on the second - further from it. Whatever distance is measured with this compass, the middle leg always divides it in extreme and average ratios. There are several points on the face that divide it in extreme and average respects. A Heringer compass helps to find these points. If you ask a patient who has front teeth to open his mouth wide and place the outer leg of a compass on the tip of the nose, and the middle one on the chin tubercle, then the distance thus obtained will be divided by it in the extreme and middle ratios. A large value will correspond to the distance between the indicated points, but with closed teeth or occlusal ridges. Using this technique, it is easy to determine the interalveolar height.
The Wadsworth-White method of determining the height of the bite is based on the equality of the distances from the middle of the pupils to the line of closure of the lips and from the base of the nasal septum to the bottom of the chin. According to the Gisi method, the height of the lower part of the face is determined by the severity of the nasolabial folds. Anthropometric methods for determining the height of the lower part are acceptable for the classic profile of the face and allow you to get the correct answer only in 10-15% of cases, and generally give an overestimation of the size of the lower part of the face. Therefore, these methods can be recommended for practical use with certain restrictions or as additional methods. The best results when establishing bite height are obtained using the anatomical and physiological method. The anatomical and physiological method is based on the use of the relative physiological rest height of the lower jaw in combination with anatomical data or functional speaking tests. From the anatomy course we know that with the correct shape of the face, the lips close freely, without tension, the nasolabial and chin folds are slightly pronounced, the corners of the mouth are slightly lowered. The basis of this method is the relative physiological rest position of the lower jaw and the fact that the occlusal height is 2-3 mm less than the height of the lower part of the face in a calm state. Physiological rest is a free position of the lower jaw, in which the distance between the teeth is 2-3 mm and the masticatory muscles are relaxed. So, to determine the height of the bite, two points are marked on the patient’s face with a pencil: one above the oral slit, the other below. Most often, one point is placed on the tip of the nose, the other on the chin, and the distance of the lower part of the face is measured in a state of physiological rest. The distance between the points is recorded on paper or a wax plate. 2-3 mm are subtracted from this distance so that when the jaws are closed, the distance between the marked points is less than the height in a state of physiological rest and, thus, the desired bite height is obtained.
The control for correct determination of the height of the lower part of the face is the interalveolar height, which on average in the area of the front teeth is 2.5-3.0 cm, and in the area of the lateral teeth - 1.5-2.0 cm. Fixation of the central relationship of the jaws. The following method of fixing the central relationship of the jaws is most often used. On the upper ridge in the area of the first premolars and molars, two non-parallel cuts are made with a spatula, and a well-heated strip of wax is applied to the lower occlusal ridge. The doctor asks the patient to close his jaws, after making sure that the closure occurs in central occlusion. Heated wax enters the notches of the upper occlusal roller, creating locks, and the heated strip of wax is squeezed out from under the rollers, as a result of which the height of the lower part of the face does not increase. In order to prevent overbite, before applying a strip of wax to the lower roller, you must first cut off the wax from it to the thickness of the new wax strip. Then the wax bases with occlusal ridges are removed from the oral cavity, cooled, excess wax is cut off and the correct fixation of the central relationship of the jaws is checked several times. At this stage, phonetic tests can be carried out for control: when pronouncing vowels, the distance between the upper and lower occlusal ridges should be 2 mm, and when speaking - up to 5 mm. 9) Drawing guide lines for setting the front teeth. Based on these lines, the technician selects the size of the teeth. On the upper roller it is necessary to apply the median line, the line of the fangs and the smile. The midline is drawn vertically - as a continuation of the midline of the face, dividing the groove of the upper lip into equal parts. This line cannot be drawn along the frenulum of the upper lip, which is quite often shifted to the side. The midline runs between the central incisors. The line of fangs, passing along the tubercles of the latter, descends from the outer wing of the nose.
Fixation of the central relationship of the jaws. The following method of fixing the central relationship of the jaws is most often used. On the upper ridge in the area of the first premolars and molars, two non-parallel cuts are made with a spatula, and a well-heated strip of wax is applied to the lower occlusal ridge. The doctor asks the patient to close his jaws, after making sure that the closure occurs in central occlusion. Heated wax enters the notches of the upper occlusal roller, creating locks, and the heated strip of wax is squeezed out from under the rollers, as a result of which the height of the lower part of the face does not increase. In order to prevent overbite, before applying a strip of wax to the lower roller, you must first cut off the wax from it to the thickness of the new wax strip. Then the wax bases with occlusal ridges are removed from the oral cavity, cooled, excess wax is cut off and the correct fixation of the central relationship of the jaws is checked several times. At this stage, phonetic tests can be carried out for control: when pronouncing vowels, the distance between the upper and lower occlusal ridges should be 2 mm, and when speaking - up to 5 mm. 9) Drawing guide lines for setting the front teeth. Based on these lines, the technician selects the size of the teeth. On the upper roller it is necessary to apply the median line, the line of the fangs and the smile. The midline is drawn vertically - as a continuation of the midline of the face, dividing the groove of the upper lip into equal parts. This line cannot be drawn along the frenulum of the upper lip, which is quite often shifted to the side. The midline runs between the central incisors. The line of fangs, passing along the tubercles of the latter, descends from the outer wing of the nose.
The smile line is horizontal, drawn at the level of the red border of the upper lip when smiling. Artificial teeth are placed in such a way that their necks are above the marked line: when you smile, they will not be visible, like the artificial gum. If the patient has dentures, they are used to determine the bite in a state of physiological rest and the thickness of the vestibular surface for correct orientation. If there is significant atrophy of the alveolar processes of both the upper and lower jaws with poor fixation of wax bases with occlusal ridges, it is advisable to determine the central ratio of the jaws on rigid bases (made of plastic), which are better fixed, do not deform or shift on the jaws. On these bases, artificial teeth are subsequently placed. After these stages of work, wax bases with occlusal ridges are removed from the oral cavity, applied to the model and fixed in the central occlusion. In this position, the models with wax bases and occlusal ridges are transferred to the dental laboratory for further work.
The next stage is checking the teeth alignment
Calculations for orthopedic purposes
In the process of creating prosthetic structures for malocclusion, an orthopedic specialist takes measurements of the heights of the lower third of the patient’s face using an anatomical and physiological method.
To do this, the height of the bite is measured in a state of complete reduction of the jaws, with central occlusion and in a state of physiological rest.
Payment procedure:
- At the lowest point of the nose , at the level of the nasal septum, the first mark is placed strictly in the center. In some cases, the specialist places a mark on the tip of the patient's nose.
- in the center of the chin , in its lower zone.
- Between the applied marks, the height is measured in the state of central occlusion of the jaws. To do this, bases with bite ridges are placed in the patient’s oral cavity.
- Repeated measurements are taken between marks , but in a state of physiological rest of the lower jaw. To do this, the specialist must distract the patient so that he really relaxes. In some cases, the patient is offered a glass of water. After a few sips, the muscles of the lower jaw really relax.
- The results are recorded. However, the standardized indicator of normal bite height, which is 2-3 mm, is subtracted from the height at rest. And if after this the indicators are equal, we can talk about normal bite height.
If, when measuring height, the calculation results yield a negative result, the lower third of the patient’s face is underestimated . Accordingly, if the result deviates in a positive direction, the bite is overestimated .
What is the significance of teleradiography in orthodontics, and what is revealed with its help.
In this publication we will talk about diagnostic methods in orthodontics.
Here https://orto-info.ru/ortodonticheskoe-lechenie/podgotovitelnyiy-period/miogimnastika.html you are offered myogymnastics exercises used in orthodontics.
Techniques for correct positioning of the lower jaw
Correct positioning of the patient's jaw in the position of central occlusion involves the use of two methods of placement: functional and instrumental.
The main condition for correct placement is muscle relaxation of the jaw muscles.
Functional
The procedure for carrying out this method is as follows:
- the patient moves his head back slightly until the neck muscles tense, which prevents protrusion of the jaw;
- touches the tongue to the back of the palate, as close to the throat as possible;
- at this time, the specialist places his index fingers on the patient’s teeth, lightly pressing on them and at the same time slightly moving the corners of the mouth in different directions;
- the patient imitates swallowing food, which in almost 100% of cases leads to muscle relaxation and prevents jaw protrusion;
- When bringing the jaws together, the specialist touches the surfaces of the teeth and holds the corners of the mouth until it is completely closed.
In some cases, the procedure is repeated several times until complete muscle relaxation and correct reduction of both rows are achieved.
Instrumental
It is performed using specialized devices that copy jaw movements. It is used only in extremely serious situations, when bite deviations are significant and it is necessary to correct the position of the jaw using the physical efforts of a specialist.
Most often, when carrying out this method, the Larin apparatus and special orthopedic rulers are used, which make it possible to record jaw movements in several planes.
Errors allowed
Creating a prosthetic structure in conditions of malocclusion is a most complex orthopedic procedure, the quality of which depends 100% on the qualifications of the specialist and a responsible approach to work.
Violations in determining the position of central occlusion can lead to the following problems:
The bite is too high
- The folds of the face are smoothed, the relief of the nasolabial zone is poorly defined;
- the patient's face looks surprised;
- the patient feels tension when closing the mouth, while closing the lips;
- the patient feels that during communication the teeth are knocking against each other.
Low bite
- The folds of the face are strongly pronounced, especially in the chin area;
- the lower third of the face visually becomes smaller;
- the patient becomes like an elderly person;
- the corners of the mouth are lowered;
- lips sink;
- uncontrolled salivation.
Permanent anterior occlusion
- There is a noticeable gap between the front incisors;
- the lateral elements do not contact normally, tubercle reduction does not occur.
Permanent lateral occlusion
- Overbite;
- clearance on the offset side;
- shifting the bottom row to the side.
Reasons for such problems
- Incorrect preparation of wax templates.
- Insufficient softening of the material for taking impressions and impressions.
- Violation of the integrity of wax forms due to their premature removal from the oral cavity.
- Excessive jaw pressure on the ridges during impression taking.
- Errors and violations on the part of the specialist.
- Errors in the work of the technician.
The video provides additional information on the topic of the article.
Causes and types
Reasons that have a negative impact on the intermaxillary distance:
- greater abrasion of teeth, due to which the strength of hard tooth tissue is lost;
- functional overload of individual teeth, which can be caused by improper bridge prosthetics;
- disorders of the nervous system that are accompanied by grinding of teeth;
- with a fight in the gastrointestinal tract;
- disturbance of phosphorus-potassium metabolic processes.
There are high and low pathological bites. The reason for the overestimation may be an incorrectly made denture, when the implant turns out to be slightly higher than the rest of the teeth.
Low bite, as a rule, is diagnosed when the hard tissues of the tooth are severely abraded, and in rare cases, when the prosthesis is installed incorrectly.