How to avoid complications after implantation
- How to behave after surgery
- Postoperative nutrition
- How long does it take to heal?
- How are sutures removed?
- Postoperative complications
- Swelling after dental implantation
- Inflammation and temperature
- Numbness
- Antibiotics after implantation
- Simultaneous (immediate) implantation
During implantation, the dentist places an artificial tooth root into the gum, which then becomes the basis for a removable or fixed denture. The operation is always complex and multi-stage, and to achieve success it requires the joint work of the doctor and the patient. Even at the current level of development of medicine, it is impossible to completely guarantee the absence of complications: aching pain, hematomas, swelling, bleeding, infection, fever. It is also possible for the implant to fail.
But if you follow the recommendations, it will be easier to avoid complications, and the implant will take root faster.
So, what to do after dental implantation to quickly relieve the consequences of surgery and the best healing of the gums?
How long does pain last after dental implant placement?
Let's consider the normal postoperative course of the condition.
1-5 day
. The pain may increase during the first few days, starting from the moment the anesthetic administered before implantation wears off. It can be aching, throbbing, and worsened by tilting the head. While this does not indicate a complication, this is the body’s natural response to intervention. As well as swelling of the tissues in the area of the implant.
5-10 day
. By the 5th day the pain subsides. The swelling subsides completely. The question remains for the patient: how much does the gum hurt after installing the implant, since it is still sensitive. By the 10th day, as a rule, everything goes away.
After 2-6 months
. There are times when everything goes fine, but after a few months or even a year a person complains that the tooth implant around it hurts. Possible reasons:
- loosening
of the plug, adaptation crown on the abutment. They rub the soft gum tissue. The situation is not critical. The dentist will adjust, carry out the necessary manipulations and you don’t have to worry about the safety of the implant;
implant rejection An unfavorable outcome of the entire implantation is unsuccessful osseointegration. The body did not accept the artificial tooth root. Fortunately, the rejection rate is close to 1%;- inflammatory
gum diseases. This is often due to poor hygiene and violation of the doctor’s postoperative recommendations; - injury
to the jaw nerve, then the jaw hurts after implantation.
If your gums, jaw, or ear hurt for more than 10 days after dental implantation, do not put off visiting the doctor who performed the operation. Early diagnosis and initiation of treatment will avoid complications. Calling after two weeks or more with such symptoms may delay treatment for a longer period.
How to behave after surgery
Doctors give the following recommendations after dental implantation:
- Do not use irrigators. Any treatment of the oral cavity should be as soft and gentle as possible. Oral baths are indicated. Active rinsing with antiseptic solutions is prohibited before the sutures are removed.
- Brush your teeth with gentle movements using a soft brush (your doctor will recommend a brush). You can use dental floss and superfloss. But it is better to clean your teeth directly at the operation site only with a cotton swab dipped in a 3% hydrogen peroxide solution.
- Avoid involuntary sneezing, coughing and blowing your nose, especially if the implantation is associated with sinus lift surgery. A sharp increase in pressure in the maxillary sinus can lead to mechanical damage to the bone tissue and displacement of the implant.
- Avoid extreme temperature changes. For this reason, it is better not to visit baths and saunas.
- Air travel can also be harmful because rapid changes in altitude make it difficult to avoid a surge in pressure in the ear-nose-throat system.
Indications
Not all dental problems require the use of Ketonal. Pain with mild and moderate caries can be relieved with saline solutions or special drops. If signs of discomfort appear, it is also necessary to avoid sweet and sour foods, as they provoke increased discomfort. In such cases, taking Ketonal is considered inappropriate.
Direct readings:
- Pulpitis is an inflammation of the nerve endings of the tooth, characterized by sharp, jerking pain. Spasms radiate to the temples and ears. With pulpitis, a person will not be able to sleep normally and eat food without strong medications.
- Periodontitis is an inflammation of the tooth root and adjacent membranes. Affected units appear mobile, rising above the rest of the elements. The pathology is accompanied by uncontrollable pain, which intensifies when touching the problem area.
- Periostitis is inflammation of the periosteum. Appears as a complication of pulpitis and gumboil.
- Injury to elements of a row and previous dental surgeries. Ketonal is intended to reduce the severity of the inflammatory process and relieve discomfort.
It should be noted that the painkiller will not be able to affect the cause of the problem. It only relieves his symptoms for a short time. For this reason, consuming Ketonal does not cancel a visit to the doctor (even if the pain syndrome no longer bothers you).
Postoperative nutrition
Avoid hot foods until the anesthesia wears off. If you eat or drink something too hot, you can accidentally burn your gums because they won't feel the temperature.
In the first two days, do not drink coffee: it increases blood pressure and this can lead to bleeding. This also explains the requirement to exclude alcohol and smoking.
Within 10 days after surgery, to strengthen injured bone tissue, include calcium-containing foods in your diet: cottage cheese, kefir, yogurt.
Do not eat salty, spicy, very hot or frozen foods, as well as rough foods - crackers, nuts. The load on the teeth should be reduced as much as possible, so you should avoid foods that require careful active chewing - for example, tough meat.
The best option for a postoperative diet is pureed, semi-liquid, moderately warm food (soups, cereals, smoothies), or finely chopped.
Ketonal Duo capsules with modified release 150 mg No. 10x2
Name
Ketonal Duo caps. with modified output 150 mg per blister. in pack №10x2
Description
Capsule, blue cap, transparent body filled with white and yellow granules. The capsules contain ketoprofen in the form of modified-release granules.
Main active ingredient
Ketoprofen
Release form
Capsules
Dosage
150mg
pharmachologic effect
Pharmacodynamics
Ketoprofen has anti-inflammatory, analgesic, antipyretic effects. Ketoprofen, the active ingredient of the drug, inhibits the synthesis of prostaglandins and leukotrienes by blocking the enzyme cyclooxygenase (cyclooxygenase-1 (COX-1) and cyclooxygenase-2 (COX-2)), which catalyzes the synthesis of prostaglandins in the metabolism of arachidonic acid. Ketoprofen stabilizes lysosomal membranes in vitro and in vivo, in high concentrations inhibits the synthesis of leukotrienes in vitro and has anti-bradykinin activity in vivo. The mechanism of the antipyretic effect of ketoprofen is unknown. It is possible that ketoprofen inhibits the synthesis of prostaglandins in the central nervous system (most likely in the hypothalamus). In some women, ketoprofen reduces the symptoms of primary dysmenorrhea, probably by suppressing the synthesis and/or effectiveness of prostaglandins.
Pharmacokinetics
Ketoprofen is well absorbed from Ketonal DUO 150 mg capsules after oral administration. Ketonal DUO 150 mg capsules are presented in a new pharmaceutical form, which differs from conventional capsules in the special release of the active substance. The capsules contain two types of granules: standard (white) and coated (yellow). Ketoprofen is released quickly from the white granules (60% of the capsule contents) and slowly from the yellow film-coated granules (40% of the capsule contents), so the capsule has both immediate and delayed effects. The bioavailability of ketoprofen from regular-release capsules is 90%; the same applies to modified-release capsules. When taking ketoprofen with food, its total bioavailability (AUC) does not change, but the rate of absorption slows down. Bioavailability (AUC) or peak plasma concentrations are not affected by a fatty meal, but peak plasma concentrations are reached later. After oral administration of 150 mg of ketoprofen in the form of modified-release capsules, peak plasma Cmax levels of 9036.64 ng/ml are observed after 1.76 hours. 99% of ketoprofen binds to plasma proteins, mainly albumin. The volume of distribution in tissues is 0.1 l/kg. Ketoprofen penetrates into the synovial fluid, where it reaches 30% of the plasma concentration. Ketoprofen is metabolized in the liver. It binds to glucuronic acid, forming an unstable metabolite, ketoprofen glucuronide, which serves as a reserve of the primary active substance. This may be important in individuals with renal impairment as the conjugate may accumulate in the serum and be deconjugated back to the primary active substance. It was noted that the conjugate appears in the plasma of healthy adults only in small quantities, but its concentration is higher in the elderly (probably due to reduced renal clearance). Approximately 60-75% of ketoprofen is excreted in the urine, mainly as a glucuronide metabolite. Less than 10% of the prescribed dose is excreted unchanged in the feces. Plasma clearance of ketoprofen is about 0.08 l/kg/hour. Special groups of patients In patients with liver failure, probably due to hypoalbuminemia (free biologically active ketoprofen), the concentration of ketoprofen almost doubles, which requires the administration of a minimum daily dose that provides a sufficient therapeutic effect. In patients with renal failure, the clearance of ketoprofen is reduced. Therefore, in case of severe renal failure, a dose reduction is required.
Indications for use
Ketonal DUO is a non-steroidal antirheumatic drug with anti-inflammatory, analgesic and antipyretic effects. It is used for pain relief in a range of pain syndromes and for the treatment of inflammatory, degenerative and metabolic rheumatic diseases. Indications for use Pain: - pain in the lumbar region (muscle sprains/tears, lumbago, sciatica, fibrosis); - dysmenorrhea; - pain due to diseases of the musculoskeletal system. Rheumatic diseases: - rheumatoid arthritis; - ankylosing spondylitis, cervical spondylitis; - osteoarthritis; - acute articular and extra-articular rheumatism (tendinitis, bursitis, capsulitis, synovitis).
Directions for use and doses
For oral administration. Take during or after meals with at least 100 ml of water or milk. Capsules should not be cracked or chewed. Undesirable effects can be minimized by taking the drug at the lowest effective dose for the shortest possible time necessary to relieve symptoms. Recommended dose The usual dose is 1 capsule of Ketonal DUO (150 mg ketoprofen) once a day. The maximum daily dose of ketoprofen is 200 mg. Before starting treatment at a dose of 150 mg of ketoprofen per day (one capsule of Ketonal DUO), you must carefully weigh the risks and benefits. Doses above the maximum daily dose are not recommended. Elderly patients and patients with impaired renal function It is recommended to reduce the initial dose and prescribe maintenance therapy using the lowest effective dose. If the drug is well tolerated, dose adjustment can be considered on an individual basis. Patients with impaired liver function Such patients should be closely monitored and the drug should be used at the lowest effective daily dose. Children The safety and effectiveness of ketoprofen in children have not been studied.
Use during pregnancy and lactation
Inhibition of prostaglandin synthesis may have a negative effect on pregnancy and/or embryo/fetal development. In the first and second trimesters of pregnancy, the drug should not be prescribed unless absolutely necessary. If Ketonal DUO is used by a woman who is trying to become pregnant or who is in the first or second trimester of pregnancy, the dose should be as low as possible and the duration of treatment should be as short as possible. In the third trimester of pregnancy, the use of Ketonal DUO is contraindicated. There are no data on the penetration of the drug into milk. It is not recommended to prescribe Ketonal DUO to nursing mothers.
Precautionary measures
Avoid simultaneous use of the drug with NSAIDs, including selective COX-2 inhibitors. Older adults are more likely to experience adverse reactions to NSAIDs, especially gastrointestinal bleeding and perforation, which can be fatal (see Dosage and Administration). Gastrointestinal bleeding, ulceration, and perforation Gastrointestinal bleeding, ulceration, or perforation, which may be fatal, has been reported for all NSAIDs and may occur at any time during treatment, with or without preexisting symptoms or severe gastrointestinal disease. tract in the anamnesis. Ketonal DUO may be associated with a high risk of severe gastrointestinal toxicity, which is common with some other NSAIDs, especially when taken in high doses (see also Dosage and Administration and Contraindications). The risk of gastrointestinal bleeding, ulceration or perforation increases with increasing doses of NSAIDs, in patients with a history of peptic ulcer disease, especially complicated by bleeding or perforation (see "Contraindications"), as well as in the elderly. Treatment of these patients should be started with the lowest dose available. For these patients, as well as for patients concomitantly taking low-dose acetylsalicylic acid or other drugs that increase the risk of gastrointestinal complications, combination therapy with protective drugs (eg, misoprostol or proton pump blockers) should be considered (see below and “Interaction with other medicinal products and other types of interactions”). Patients with a history of gastrointestinal toxicity, especially the elderly, should report any unusual abdominal symptoms (especially gastrointestinal bleeding), especially early in treatment. Particular caution should be exercised when co-administered with drugs that may increase the risk of ulceration or bleeding, such as oral corticosteroids, anticoagulants (eg, warfarin), selective serotonin reuptake inhibitors, or antiplatelet agents such as acetylsalicylic acid (see Interactions with other medications and other types of interactions"). If patients experience gastrointestinal bleeding or ulcers during treatment with Ketonal DUO, the drug should be discontinued. NSAIDs should be prescribed with caution to patients with a history of gastrointestinal diseases (ulcerative colitis, Crohn's disease), since they may experience exacerbations of these diseases (see “Side Effects”). Cardiovascular and cerebrovascular effects. Patients with a history of hypertension and/or mild to moderate congestive heart failure require appropriate monitoring and counseling as fluid retention and edema have been reported with the use of NSAIDs. The use of some NSAIDs (especially at high doses and during long-term treatment) may be associated with an increased risk of arterial thrombosis (eg, myocardial infarction or stroke) (see Warnings and Precautions). There is insufficient data to exclude such a risk for ketoprofen. In patients with uncontrolled hypertension, congestive heart failure, established coronary artery disease, peripheral arterial disease and/or cerebrovascular disease, treatment with Ketonal DUO should be carried out only after a careful assessment of benefits and risks. The same should be done before prescribing long-term treatment for patients with risk factors for cardiovascular disease (eg, hypertension, hyperlipidemia, diabetes mellitus, smoking). Patients suffering from bronchial asthma in combination with chronic rhinitis, chronic sinusitis and/or nasal polyposis are more likely to experience allergic reactions after taking acetylsalicylic acid and/or non-steroidal anti-inflammatory drugs than other patients. Prescribing Ketonal DUO may cause an attack of bronchial asthma or bronchospasm, especially in patients with an allergy to acetylsalicylic acid or NSAIDs (see “Contraindications”). In patients with heart failure, cirrhosis and nephrotic syndrome, as well as in patients taking diuretics and in patients with chronic renal failure, especially the elderly, renal function should be carefully monitored at the start of treatment. In such patients, the administration of Ketonal DUO may cause a decrease in renal blood flow due to inhibition of prostaglandin synthesis and lead to decompensation of renal function. In patients with abnormal liver function tests or a history of liver disease, blood transaminase levels should be periodically monitored, especially during prolonged therapy. Rare cases of jaundice and hepatitis have been described in connection with the use of ketoprofen. Treatment should be discontinued if visual disturbances such as blurred vision occur. The drug is prescribed with caution to persons suffering from alcohol dependence. Severe skin reactions (some of them fatal) associated with the use of NSAIDs, such as exfoliative dermatitis, Stevens-Johnson syndrome and toxic epidermal necrolysis, have been reported extremely rarely (see “Side effects”). The greatest risk of developing these reactions is at the beginning of the course of treatment; in most cases, reactions occur in the first month of treatment. Ketonal DUO should be discontinued at the first appearance of skin rash, lesions on the mucous membranes or other signs of hypersensitivity. Ketonal DUO may mask signs and symptoms of infectious diseases, such as elevated body temperature. Before extensive surgical interventions, the drug must be discontinued. The use of Ketonal DUO may reduce fertility, so it is not recommended for women planning pregnancy. In women experiencing difficulty becoming pregnant or being evaluated for infertility, discontinuation of Ketonal DUO should be considered. Ketonal DUO capsules contain lactose and should not be taken by patients with hereditary galactose intolerance, lactase deficiency or glucose or galactose malabsorption.
Interaction with other drugs
Drug combinations not recommended Other NSAIDs (including selective cyclooxygenase-2 inhibitors) and salicylates in high doses: increased risk of ulcers and bleeding in the gastrointestinal tract. Anticoagulants (heparin and warfarin) and platelet aggregation inhibitors (eg, ticlopidine, clopidogrel): increased risk of bleeding (see Warnings and Precautions). If co-administration is necessary, close medical supervision is required. Lithium: Risk of increased plasma lithium levels, which can sometimes reach toxic levels due to decreased renal excretion of lithium. If necessary, plasma lithium concentrations should be carefully monitored and the dose of lithium adjusted during and after NSAID treatment. Methotrexate in doses exceeding 15 mg/week: increased risk of hematotoxicity of methotrexate, especially if used in high doses (>15 mg/week), which is likely due to the displacement of methotrexate from protein binding and reduced renal clearance. Combinations Requiring Caution Diuretics: Patients receiving diuretics, especially those with dehydration, are at increased risk of renal failure due to decreased renal blood flow due to inhibition of prostaglandin synthesis. Such patients should be adequately hydrated before initiating concomitant use of these drugs, and renal function should be monitored at the start of treatment (see "Special Instructions and Precautions"). Angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor antagonists. In patients with impaired renal function (eg, dehydrated patients or the elderly), concomitant use of an ACE inhibitor or angiotensin II receptor antagonist and cyclooxygenase inhibitors may cause further deterioration of renal function, including possible acute renal failure. Methotrexate in doses below 15 mg/week: in the first weeks of combination treatment, it is necessary to monitor the detailed blood picture once a week. If there is any impairment of renal function and in elderly patients, monitoring should be carried out more often. Corticosteroids: Increased risk of ulcers or bleeding in the gastrointestinal tract (see Warnings and Precautions). Pentoxifylline: increases the risk of bleeding. More frequent clinical monitoring and more frequent control of bleeding time are necessary. Tenofovir: Concomitant use of tenofovir disoproxil fumarate and an NSAID may increase the risk of renal failure. Combinations that need to be taken into account Antihypertensive drugs (beta blockers, ACE inhibitors, diuretics) Ketoprofen reduces the effect of antihypertensive drugs (inhibition of the synthesis of vasodilator prostaglandins). Probenecid: Concomitant use of probenecid may significantly reduce the plasma clearance of ketoprofen. Combinations that should also be taken into account: Cyclosporine, tacrolimus: risk of additive nephrotoxicity, especially in elderly patients. Thrombolytics: increased risk of bleeding. Selective serotonin reuptake inhibitors: increased risk of gastrointestinal bleeding (see "Special Instructions and Precautions"). Gemeprost: the effectiveness of gemeprost may be reduced. Intrauterine contraceptives: The effectiveness of intrauterine contraceptives may be reduced.
Contraindications
- Hypersensitivity to ketoprofen or any of the excipients of the drug; - a history of bronchial asthma, urticaria, bronchospasm, rhinitis or allergic-type reactions after using ketoprofen or similar active substances, such as other nonsteroidal anti-inflammatory drugs (NSAIDs) or salicylates (eg, acetylsalicylic acid); in such patients, severe (in rare cases fatal) anaphylactic reactions have been described (see “Side effects”); - severe heart failure; — treatment of pain in the perioperative period during coronary artery bypass grafting (CABG); - history of chronic dyspepsia; - peptic ulcer in the acute phase, as well as a history of gastrointestinal bleeding, ulcer or perforation; - predisposition to bleeding; - severe renal dysfunction; - severe liver dysfunction; - last trimester of pregnancy (see “Pregnancy and lactation”); - children.
Compound
Each capsule contains 150 mg of ketoprofen in the form of modified-release granules. Excipients Capsule contents: microcrystalline cellulose, lactose monohydrate, povidone, croscarmellose sodium, polysorbate 80, Eudragit RS 30D (30% dispersion of amino methacrylate copolymer (type B)), Eudragit RL 30D (30% dispersion of amino methacrylate copolymer (type A)), triethyl citrate , talc, iron oxide yellow E172, colloidal anhydrous silicon dioxide; capsule shell: gelatin, indigotine E 132, titanium dioxide E 171.
Overdose
Cases of overdose of ketoprofen in a dose of up to 2.5 g have been described. In most cases, the observed symptoms were benign in nature and were limited to lethargy, drowsiness, nausea, vomiting and epigastric pain. There is no special antidote for an overdose of ketoprofen. If a significant overdose is suspected, gastric lavage and symptomatic and supportive therapy are recommended to eliminate dehydration. You also need to monitor diuresis and correct acidosis (if it develops). If renal failure develops, hemodialysis may be effective to remove the drug circulating in the blood.
Side effect
Edema, high blood pressure and heart failure have been reported in association with treatment with non-selective NSAIDs. If severe side effects occur, treatment should be discontinued. Adverse effects are distributed by organ system class, by frequency of occurrence and descending severity: very common (≥ 1/10); frequent (≥ 1/100,
Storage conditions
Keep out of the reach of children. Store at a temperature not exceeding 25°C.
Buy Ketonal Duo capsules with modified release 150 mg No. 10x2 in the pharmacy
Price for Ketonal Duo capsules with modified release 150 mg No. 10x2
Instructions for use for Ketonal Duo capsules with modified release 150 mg No. 10x2
How long does it take to heal?
Bone tissue and gums heal after dental implantation on average from three to six months, and the period is different for the upper and lower jaws. The lower jaw will heal in three to four months, but the upper jaw will take longer: four to six months. This is due to the greater bone density of the lower jaw.
Sometimes the healing rate deviates from the average time frame, because it depends on the individual characteristics of the patient’s body: the speed of regeneration, the strength of the immune system, the pain threshold. Even such factors as gender, age, lifestyle, diet and daily routine of the patient are important.
In any case, recovery after surgery takes some time. Following medical recommendations will help protect yourself from complications during healing.
How are sutures removed?
Sutures after dental implantation are usually removed 10-14 days after surgery, unless otherwise indicated. Throughout this period, surgical sutures need careful, delicate handling. After suturing, there may be some discharge or slight pain. It is permissible to use painkillers (Nise, Ketanov or another remedy recommended by a doctor).
Modern dentistry uses strong synthetic threads that do not break even with active chewing of food, so dental sutures now rarely come apart. But suture dehiscence is still possible - however, it is most often associated with violations of medical recommendations, most often with mechanical damage to the operation area.
Removal of sutures does not require anesthesia and is completely painless.
Side effects
It is necessary to stop taking Ketonal if the following side symptoms appear:
- nausea and vomiting;
- heart rhythm disturbances;
- diarrhea;
- severe headache;
- sleep disorders;
- allergic reactions on the skin;
- difficulty breathing;
- violations of the pronunciation of words and sounds;
- increased blood pressure.
In such cases, the doctor can adjust the dose of Ketonal or replace it with similar drugs with an analgesic effect.
Postoperative complications
The most common complications after dental implantation are:
- Pain syndrome. The norm is mild soreness of the gums in the area of implantation for 1-2 days. In cases where severe pain does not go away even after taking the generally recommended painkiller, you should consult a doctor, because this is most often a symptom of a complication.
- Inflammation.
- Seams coming apart.
- Hemorrhages. After surgery, ichor often separates from the gums, the amount of which quickly decreases and disappears. It is enough to remove it with cotton swabs. But if the bleeding becomes more intense, you should consult a doctor immediately.
There are also complications such as inflammation of the sinuses, peri-implantitis (inflammation of the tissue around the implant, leading to destruction of the supporting bone tissue), mucosal hyperplasia (pathological growth of the mucous membrane in the area of the implant), damage to the implant and prosthesis.
How to Reduce or Prevent Pain During Recovery, Do's and Don'ts
In the postoperative period, the main thing is to strictly follow all the doctor’s recommendations. Basic:
- in the first hours after implantation, do not eat or drink;
- the first days (about a week) eat liquid foods: soups, purees, baby food;
- exclude hot, cold, spicy, alcohol;
- After surgery, apply cold compresses to relieve swelling;
- take prescribed medications strictly according to the schedule. Do not cancel them yourself if you feel better;
- make mouth baths using antiseptics: chlorhexidine, chamomile;
- sleep on a high pillow and on the opposite operating side;
- forget about physical activity for a while;
- Going to bathhouses and saunas is prohibited.
Usually, every dental clinic has a reminder about what is possible after implantation, what is prohibited, how to relieve pain after dental implantation, and a schedule for visiting the doctor.
The doctor will definitely prescribe painkillers - Nurofen, Nimesil, Analgin, Nise, etc. They need to be taken as long as the pain lasts after installing the dental implant, up to 7-10 days. If it persists longer, it is better to contact your dentist.
Swelling after dental implantation
In the first three days after implantation, swelling may occur in the gum tissue. This is the body's natural reaction to surgery. Most often, a tumor is an indicator that blood is actively flowing to the operation site.
But if you want to avoid the discomfort caused by swelling, you can reduce the risk of its occurrence. To do this, in the first two days, apply cold to the operation site: for 5-10 minutes with breaks of 20 minutes. Do not apply ice directly to the skin; it is best to wrap it in a towel. In rare cases, the tumor will require the use of antihistamines, antibiotics (to prevent infection) or treatment with antiseptic solutions.
It will also help to avoid swelling by eliminating sudden stress loads on the body: physical overload, hypothermia, overheating.
Inflammation and temperature after dental implantation
Your body may also react to surgery with a low-grade fever, that is, an increase in general body temperature to 37°C. Even if the temperature stays within these limits for several days, this will remain the norm. You should be wary only when there is a persistent increase in temperature to 37.8-38°C. In this case, it almost certainly means inflammation, which requires immediate intervention (for example, in case of peri-implantitis, this should be sanitation of abscesses, bone regeneration, as well as professional oral hygiene).
In this case, you should not delay visiting a doctor: the inflammation can not only worsen on its own, but also lead to implant rejection.
Instructions for use KETONAL® (KETONAL) suppositories
Undesirable effects can be minimized by prescribing the drug at the minimum dose for the shortest period of time necessary to control symptoms.
Elderly patients have an increased incidence of side effects of NSAIDs, especially gastrointestinal bleeding and perforation, which can be fatal.
At the beginning of treatment, renal function should be monitored in patients with impaired cardiac function, heart failure, impaired liver function, cirrhosis and nephrosis, as well as in patients receiving diuretics, patients with chronic renal failure, especially in old age. The use of ketoprofen in these patients may result in decreased renal blood flow caused by prostaglandin inhibition and impaired renal function.
NSAIDs have been found to have nephrotoxicity in various forms, which can lead to interstitial nephritis, nephrotic syndrome and renal failure.
In patients with impaired liver function, as well as in patients who have had liver disease, transaminase levels should be periodically monitored, especially during long-term therapy. Rare cases of jaundice and hepatitis have been described in patients taking ketoprofen.
Cardiovascular and cerebrovascular effects:
- Appropriate monitoring and consultation are required for patients with a history of hypertension and/or mild to moderate congestive heart failure, manifested by fluid retention or edema, associated with NSAID treatment.
Clinical experience and epidemiological data suggest that the use of some NSAIDs (especially at high doses and during long-term treatment) may be associated with an increased risk of arterial thrombosis (eg, myocardial infarction or stroke). There is insufficient data to exclude such a risk for ketoprofen.
In patients with uncontrolled hypertension, congestive heart failure, established coronary artery disease, peripheral arterial disease and/or cerebrovascular disease, treatment with ketoprofen should be undertaken only after careful assessment of the appropriateness of its use. Such an analysis should be done before starting long-term treatment in patients with risk factors for cardiovascular disease (for example, hypertension, hyperlipidemia, diabetes mellitus, smoking).
Patients suffering from bronchial asthma, in combination with chronic rhinitis, chronic sinusitis and/or nasal polyposis, are more likely to experience allergic reactions after taking acetylsalicylic acid and/or NSAIDs than in the general population. The use of the drug may cause attacks of bronchial asthma or bronchospasm, especially in patients with an allergy to acetylsalicylic acid or NSAIDs
Gastrointestinal bleeding, ulceration or perforation with risk of death has been reported for all NSAIDs at any stage of treatment, with or without warning symptoms or a history of previous severe gastrointestinal illness.
Some epidemiological data suggest that ketoprofen may be associated with a higher risk of severe gastrointestinal toxicity compared with some other NSAIDs, especially at high doses.
In patients with a history of peptic ulcer disease, especially those complicated by bleeding or perforation, and in elderly patients, the risk of gastrointestinal bleeding, ulceration or perforation increases with increasing doses of NSAIDs. In such patients, treatment should be started with the minimum effective dose.
For these patients, as well as for patients who require concomitant use of low-dose acetylsalicylic acid or other drugs that increase the risk of gastrointestinal complications, concomitant administration of drugs that protect the gastrointestinal mucosa (for example, misoprostol or proton pump blockers) may be required.
NSAIDs should be prescribed with caution to patients with a history of gastrointestinal diseases (ulcerative colitis, Crohn's disease), because their aggravation is possible.
Patients who have experienced gastrointestinal toxicity, especially elderly patients during the initial stages of treatment, should report any unusual abdominal symptoms. The risk of gastrointestinal bleeding should be kept in mind.
Caution is required when using Ketonal in patients receiving concomitant therapy with drugs that may increase the risk of ulcerative lesions or bleeding, for example, ingestion of corticosteroids, anticoagulants such as warfarin, selective serotonin reuptake inhibitors or antiplatelet agents such as acetylsalicylic acid.
If gastrointestinal bleeding or ulceration develops in patients receiving ketoprofen, treatment should be discontinued.
There may be an increased risk of serous meningitis in patients with systemic lupus erythematosus and mixed connective tissue lesions.
Severe skin reactions (some of them fatal) such as exfoliative dermatitis, Stevens-Johnson syndrome and toxic epidermal necrolysis have been observed extremely rarely in association with the use of NSAIDs. Patients are at greatest risk of developing these reactions at the beginning of treatment; in most cases, the occurrence of a reaction is noted within the first month of treatment. Ketonal® should be discontinued at the first appearance of a skin rash, changes in the mucous membranes or other signs of hypersensitivity.
As with the use of other NSAIDs in the presence of infectious diseases, it must be taken into account that the anti-inflammatory, analgesic and antipyretic effects of ketoprofen may mask the symptoms of infection, such as fever.
If visual disturbances, such as blurred vision, appear during treatment, the drug should be discontinued.
Impact on the ability to drive vehicles and operate machinery
Patients should be warned about the possible occurrence of drowsiness, dizziness, or convulsions while taking the drug. If there is a risk of developing such reactions, patients should refrain from driving vehicles and operating machinery.
Results of preclinical safety studies
Acute toxicity. After oral administration, the LD50 of ketoprofen was 360 mg/kg in mice, 160 mg/kg in rats, and 1300 mg/kg in guinea pigs. The LD50 of ketoprofen is several times higher than that of indomethacin.
Chronic toxicity. Ketoprofen was administered orally to rats for 4 weeks at doses of 2, 6 or 18 mg/kg. 10% of animals receiving ketoprofen at a dose of 18 mg/kg died on days 6-30, some had ulceration of the intestinal mucosa. In dogs receiving the same dose, only intestinal ulcerations were described, while no animals died. Among the animals receiving indomethacin at a dose of 6 mg/kg body weight, half died; all animals receiving 18 mg/kg body weight died.
In a 6-month study, rats were administered orally ketoprofen at doses of 3, 6 or 9 mg/kg. After 8 weeks, 53% of male rats treated with 6 mg/kg and 67% of male and 20% of female rats treated with 9 mg/kg died. In animals receiving 9 mg/kg, plasma concentrations of all proteins decreased and spleen weight increased. Histopathological studies of tissues from surviving animals did not reveal significant pathological changes.
Carcinogenicity, mutagenicity and effects on fertility. Long-term toxicity studies in mice administered orally ketoprofen up to 32 mg/kg/day did not reveal carcinogenic effects of this drug. The Ames test did not show any mutagenic properties. Ketoprofen did not affect the fertility of male rats that received up to 9 mg/kg/day orally. In female rats receiving 6 or 9 mg/kg/day, the number of implantations was reduced. In male rats and dogs, suppression of spermatogenesis was found. Dogs and male monkeys treated with high doses of ketoprofen experienced a decrease in testicular weight.
Teratogenicity. Neither teratogenic effects nor effects on the fetus were shown in mice receiving ketoprofen up to 12 mg/kg/day and in rats receiving up to 9 mg/kg/day. Doses of ketoprofen that were toxic in terms of fetal damage in rabbits were not teratogenic.
Numbness after dental implantation
For most patients, anesthesia wears off within four to five hours after implant placement. Then oral sensitivity should return. If numbness persists after this period, then you have cause for concern because it may indicate nerve damage. This is only possible when the operation was performed on the lower jaw, because there are no large nerves in the upper jaw.
Other symptoms of mandibular nerve injury are lack of facial skin sensitivity, excessive salivation, and difficulty speaking and eating. Timely diagnosis will help to establish the nature and extent of the damage and manage the treatment with medications rather than surgical methods.
Ketonal in the practice of a rheumatologist
Z
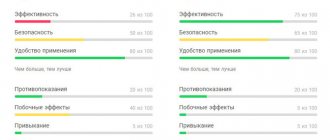
Joint diseases are one of the most common reasons for a patient to visit a doctor (Fig. 1).
The pain syndrome accompanying damage to joints and periarticular tissues in most cases is chronic, significantly worsening the patient’s quality of life. Although there are many reasons for the appearance of pain in various structures of the musculoskeletal system: pain can be associated with damage to blood vessels or nerves, with increased intramedullary pressure, with spasm of the periarticular muscles, but most often the pain syndrome is associated with the development of chronic inflammation in the synovium
. Patients suffering from rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthropathy are often forced to take painkillers for many years, which should also have an anti-inflammatory effect. The increasing incidence of deforming osteoarthritis in the population also increases the number of patients in need of pain-relieving agents. Therefore, certain requirements are imposed on drugs that reduce inflammation and pain: the drugs must be effective and well tolerated both in the short term and over long periods of use.
Rice.
1. The incidence of various diseases in the population (US National Health Interview Survey, 1999) Nonsteroidal anti-inflammatory drugs
(NSAIDs) have three main actions - analgesic, anti-inflammatory and antipyretic.
They are widely used in medical practice, primarily for the relief of acute and chronic pain of various origins. Most drugs in this group are, by their main mechanism of action, non-selective inhibitors of the enzyme cyclooxygenase (COX), which is involved in the breakdown of phospholipids in cell membranes when cells are damaged [1], which determines their therapeutic effect (suppression of COX-2), but is also associated with the development of adverse reactions (suppression of COX-1). These provisions formed the basis for the development of a new class of NSAIDs - COX-2 selective drugs
(meloxicam, nimesulide, celecoxib), the effectiveness of which in chronic inflammatory diseases of the musculoskeletal system is well known to clinicians, and the tolerability in relation to the mucous membrane of the gastrointestinal tract (GIT) is comparable using placebo [2,3]. When using non-selective COX inhibitors, it was believed that a more pronounced analgesic or anti-inflammatory effect is necessarily associated with a higher frequency of side effects. However, in recent years, new facts have emerged about the COX-independent mechanisms of the effectiveness and toxicity of NSAIDs [4]. There have been reports that non-selective NSAIDs have a central mechanism of analgesic action, which in most cases is more pronounced than that of selective COX-2 inhibitors [5,6].
The drug ketoprofen (Ketonal)
is a derivative of propionic acid, as well as the well-known and long-known ibuprofen and flurbiprofen.
Propionic acid derivatives are the most well tolerated among other non-selective NSAIDs. Its pronounced analgesic effect is well known, exceeding that of derivatives of phenylacetic acid (diclofenac) and indoleacetic acid (indomethacin). In this regard, “a priori” it was believed that ketoprofen should also be poorly tolerated. This may be why Ketonal is more widely used by specialists dealing with the problems of acute pain syndrome - surgeons, traumatologists, dentists, gynecologists and oncologists - than by specialists - rheumatologists. In the works of P.S. Veksheva et al. [7] optimal pain relief during minor traumatic surgical interventions in 94.3% of cases was achieved with Ketonal monotherapy at a dose of 100 mg 2–3 times a day. During highly traumatic surgical interventions, the use of Ketonal made it possible to reduce the dose of narcotic analgesics [8]. A comparative study of the effectiveness of various NSAIDs in postoperative pain relief showed the advantages of Ketonal (300 mg/day IM) over diclofenac (150–200 mg/day IM) and ketorolac (90 mg/day IM) with better tolerability of Ketonal: frequency adverse effects were 4%, 31% and 14%, respectively [9,10]. Also, high efficiency and better tolerability of Ketonal compared to indomethacin and diclofenac were noted in the treatment of pain in patients with malignant tumors [11]. When using Ketonal for pain relief in gynecological practice after endoscopic interventions, it was shown that the most effective form of the drug is forte tablets compared to suppository and capsulated forms
[12].
In most cases, a rheumatologist deals with chronic joint diseases (arthritis, arthrosis), when patients are forced to continuously use NSAIDs for many months and years. The required duration of taking NSAIDs and the known fact that the frequency of adverse reactions from the gastrointestinal tract (ulcers of the gastric and duodenal mucosa, bleeding) while taking NSAIDs is higher in patients with damage to the musculoskeletal system than in those suffering from other types of chronic pain [13 ], force the doctor to look for the safest drugs. However, selective COX-2 inhibitors in some forms of inflammation have an anti-inflammatory effect only in very high doses, when the synthesis of COX-1 is also suppressed.
Ketonal belongs to the group of propionic acid derivatives, which includes the safest NSAIDs, has a short half-life (T1/2 = 1–2 hours), rapid absorption and elimination [14]. Due to its high fat solubility, Ketonal quickly penetrates the blood-brain barrier and is able to influence the transmission of pain signals at the level of the dorsal horns of the spinal cord, which determines its central mechanism of analgesic action. These pharmacodynamic characteristics of ketoprofen served as the basis for the wider use of Ketonal in rheumatological practice. We conducted clinical and clinical endoscopic studies to study the effectiveness and tolerability of Ketonal in patients with severely active rheumatoid arthritis, ankylosing spondylitis with long-term use, as well as in patients with arthrosis. A number of special clinical studies have already shown that the pharmacokinetics of Ketonal in young and elderly people does not have pronounced differences [15,16]. In addition, ketoprofen does not have a significant effect on the synthesis of proteoglycans by chondrocytes in in vitro and in vivo studies [17], that is, it does not have a negative effect on articular cartilage.
According to our data, when prescribing various forms of Ketonal, the frequency of development of a positive effect was 87% when using the tablet form, 79% when using intramuscular injections and 100% when using Ketonal in the form of 5% cream. Interesting data from JS Walker et al. [18], who showed that in RA patients who “responded” to ketoprofen, before prescribing the drug, there was a significant increase in the concentration of tumor necrosis factor-a and a tendency to an increase in the level of other proinflammatory cytokines compared to patients who “did not respond” to ketoprofen. These data confirm that the pronounced anti-inflammatory and analgesic effects of ketoprofen are associated not only with COX-mediated inhibition of prostaglandin synthesis. The drug provides a rapid and reliable reduction in pain and parameters reflecting the level of inflammation in the joints.
In a clinical endoscopic study of the effectiveness and tolerability of Ketonal in various dosage forms in patients with active rheumatoid arthritis who received Ketonal in the form of suppositories (50 mg each), forte tablets (100 mg each) or retard tablets (150 mg each) for 3 -x months we received confirmation of the high analgesic and anti-inflammatory activity of Ketonal with its good tolerability [19]. The comparative frequency of erosive and ulcerative lesions of the gastrointestinal mucosa when using various NSAIDs is demonstrated in Figure 2. It can be seen that the frequency of damage to the gastrointestinal mucosa with the use of Ketonal is comparable to that with the use of selective COX-2 inhibitors.
Rice. 2. Frequency of damage to the gastrointestinal mucosa due to the use of NSAIDs
Thus,
Ketonal showed high effectiveness in the treatment of joint pain and inflammation in patients with chronic joint diseases in combination with good tolerability.
The drug can be successfully used for long-term treatment of such patients, including elderly patients.
References:
1. Vane JR Inhibition of prostaglandin synthesis as a mechanism of action for the aspiei-like drugs. Nature, 1971; 231; 235–239.
2. Nasonov E.L. Non-steroidal anti-inflammatory drugs (prospects for use in medicine). M., "Anko", 2000, 143 pp.
3. Crofford LJ, Lipsky PE, Brooks P. et.al., Basic biology and clinical application of specific cyclooxygenase–2 inhibitors. Arthr.Rheum., 2000; 43;4–13.
4. Fitzgarald GA, Partono C. The coxibs, selective inhibitors of cyclooxigenase-2. N.Engl.J.Med., 2001; 345;433–442.
5. Bannwarth B., Demotes–Mainard F., Schaeverbeke T. et.al. Central analgesic effects of aspirin–like drugs. Fund.Clin.Pharm., 1995; 9;1–7.
6. McCormack K., Urguhat E. Correlation between non-steroidal anti-inflammatory drug efficacy in a clinical pain model and the dissociation of their anti-inflammatory and analgesic properties in animal model. Clin. Drug Invest., 1995; 9; 88–97.
7. Vetshev P.S., Chilingaridi K.E., Ippolitov L.I. and others. Surgical stress in various types of cholecystectomy. Surgery, 2002, No. 3, pp. 4–10.
8. Vetshev P.S., Vetsheva M.S. Principles of analgesia in the early postoperative period. Surgery, 2002, No. 12, 49–52.
9. Kirienko P.A., Gelfand B.R., Levanovich D.A. etc. Comparative assessment of the effectiveness of non-steroidal anti-inflammatory drugs used for postoperative pain relief. Consillium medicum, Surgery No. 2, 2002.
10. Gelfand B.R., Kirienko P.A., Levanovich D.A., Borzenko A.G. Comparative assessment of the effectiveness of non-steroidal anti-inflammatory drugs used for postoperative pain relief. Bulletin of Intensive Care, 2002, No. 4, Postoperative period, pp. 83–88.
11. Novikov G.A., Vaisman M.A., Prokhorov B.M. et al. Ketonal in the treatment of pain in patients with common forms of malignant neoplasms. Palliative Medicine and Rehabilitation, No. 3, 2002, 48–51.
12. Ailamazyan E.K., Niauri D.A., Ziyatdinova G.M. Clinical and economic rationale for the use of ketonal for pain relief after endoscopic interventions in gynecology. Russian Bulletin of Obstetrician and Gynecologist, No. 6, 2002, 51–53.
13. Janssen M., Dijkmans B., van der Sluijs FA “Upper gastrointestinal complaints and complications in chronic rheumatic patients in comparison with other chronic diseases” Br.J.Rheum., 1992., Vol.31: 747–752.
14. Williams RL, Upton RA The clinical pharmacology of ketoprofen. J.Clin.Pharm., 1988; 28: 13–22.
15. Schattenkirchen M. Long-term safety of ketoprofen in an elderly population of arthritis patients. Scand.J.Rheum., 1991; 91(Suppl.): 27–36.
16. Le Loet X. Safety of ketoprofen in the elderly: a prospective study on 20,000 patients/ Scand.J.Rheum., 1989; 83:21–27.
17. Huber–Brunning O., Willbrinck B., Vanroy J., Vanderveen MJ Potential influences of ketoprofan on human healthy and osteoarthritic cartilage in vitro. Scand. J Rheum 1989;18:29–32.
18. Walker JS, Sheater–Rehd RB Carmody JJ et.al. Nonsteroidal anti–inflammatory drugs in rheumatoid arthritis and osteoarthritis. Support for the concept of “responder” and “nonresponder”. Arthr.Rheum., 1987; 11: 1944–1954.
19. Chichasova N.V., Imametdinova G.R., Karateev A.E. and others. Efficacy and safety of ketoprofen (ketonal) for rheumatoid arthritis (clinical and endoscopic study). Scientific and practical rheumatology, 2001; 1:47–52.
Antibiotics after dental implantation
For preventative purposes, the doctor prescribes a course of antibiotics after surgery. In most cases, this is inevitable, since surgical trauma, even with the modern level of development of medicine, carries a high risk of infection. Therefore, it is better not to ignore antibacterial drugs prescribed by a doctor if you do not want to additionally place unnecessary burden on your immune system to fight infection.
Most often, the course of antibacterial therapy does not exceed 7 days, and broad-spectrum drugs are prescribed - amoxicillin, amoxiclav, cephalosporins. They are characterized by low toxicity and have long proven themselves to be well tolerated by the human body.
Contraindications
Ketonal has a strong therapeutic effect. There are a number of contraindications to its use:
- digestive system dysfunction;
- serious pathologies of the liver and kidneys;
- problems with blood clotting;
- natural feeding;
- anemia;
- exacerbation of chronic gastrointestinal diseases;
- stomatitis in acute form;
- heart failure;
- diabetes.
Taking Ketonal is also not recommended for people dependent on alcohol. Taking medication and alcohol together can have serious consequences for the body.
Before consuming Ketonal and other medications together, you should consult your doctor. Some groups of medications are incompatible with NSAIDs.
Simultaneous (immediate) implantation
This prosthetic method is a one-stage implantation. In this case, the dentist removes the patient’s damaged tooth and immediately installs an artificial root.
Implantation immediately after tooth extraction is only possible if the bone tissue has sufficient volume to accommodate the implant - for example, if the tooth was damaged or lost in an accident. But tooth loss much more often occurs due to diseases when bone tissue is lost. Therefore, this method is not always available.
Dental implantation is an achievement of modern dentistry that allows you to restore lost teeth and use them for the rest of your life. And if you carefully follow your doctor’s recommendations, your smile will always bring joy to your loved ones!
What if the implant gets sick long after surgery?
Peri-implantitis is insidious; it can occur unnoticed. After some time, there will be a sharp or bursting pain, radiating even to the nose, ear, head, face. This indicates inflammation of the tissue around the artificial root. Complaint: the tooth implant hurts; it is incorrect in this case. After all, the implant itself cannot hurt; it is a non-living structure, but the soft tissue around it can. The main thing is not to wait as long as you are willing to endure, but to go to the clinic urgently.
Peri-imlantitis on x-ray
The body is not always ready to accept a foreign object and osseointegrate with it. Rejection is extremely rare - less than 1.5% of cases. But you must always monitor your well-being.