Reason for breakage
The canals in our teeth have a very complex structure; they are curved, very thin and branched in different directions. To clean the canal to the very end, the doctor uses special devices, which are also very thin and flexible. Unfortunately, it is impossible to completely protect yourself from item damage. Even the most experienced professional cannot be 100% insured against such an incident.
The process of removing a foreign object is quite difficult, so not every master can cope with the task. The final decision on the need to remove a part should be made only after an adequate assessment of all the pros and cons.
There are many nuances, for example, if part of the instrument is lost in a living tooth and at the final stage of treatment, no complications should arise in the future. The patient will not encounter an allergic reaction, inflammatory processes or increased sensitivity to various irritants in the future.
The main ways that fragments of dental instruments get into dental canals
A broken instrument in a tooth canal can appear due to the direct influence of several reasons, and is directly related to the treatment procedure. Most often, this situation occurs when a dead nerve or blood vessels are removed - a fragment of an instrument remains in the tooth, which, at the dentist’s discretion, can be removed or left, depending on the patient’s indications. Also, the reason that an instrument remains in the tooth canal may be:
- When a dentist passes curved and narrow canals, dental instruments may not withstand the stress caused by their bends.
- When using only hand tools, tip fractures occur due to a metallurgical defect or due to metal fatigue.
Possible complications
It is worth noting that a piece of the instrument itself does not pose any threat to the patient’s health. This is explained by the fact that such items are made from hypoallergenic materials. However, the part may prevent complete cleaning of the dental canal, which will negatively affect the outcome of the entire treatment. As a result, inflammation may develop, severe pain will occur, and in rare cases, tooth extraction may be necessary.
Parts remaining in the canal can negatively affect recovery after treatment. In rare cases, the patient may develop an allergy; sometimes it is accompanied by a strong tooth, swelling and redness of the soft tissues and mucous membrane located next to the diseased tooth.
The final prognosis of endodontic treatment will depend on many factors, for example, on the stage at which the working instrument broke, as well as on the degree of preparation and sufficient treatment of the canal with medications at this stage.
Closing tooth perforations.
Perforation is a hole in a tooth, and an artificial one. It occurs if the doctor worked too zealously and carelessly with the tooth. This most often happens when preparing canals for the installation of various types of pins.
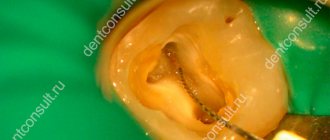
In our case, the lower chewing tooth was restored after treatment with a filling on a pin... and more than one. Apparently, the principle “you can’t spoil porridge with butter” worked. But that was a mess, but for the tooth, the “multiple pins” actually turned out to be murder: one of the pins was installed past the root canal and pierced right through the bottom. Perhaps the tooth was mobile and the doctor wanted to strengthen it a little in this way, but then it was worth choosing a longer pin...
Here in the photo, after removing the old filling, 2 pins are found screwed into the tooth (on the left), and after their removal we see the bottom of the tooth cavity in the holes (on the right).
As it turned out, one of these holes was, as the sailors would say, “below the waterline.” In dental terms, this is root perforation . The tooth channel is in one direction (the channels are shown by green arrows), the hole for the pin is completely in the other direction (the perforation is shown by a red arrow).
A puddle of blood seems to hint that a crime has taken place here. The killer doctor tried to drill a tooth to death and he almost succeeded. Most often, teeth with perforations are sent by dentists for removal. But with good visualization, which is provided by an operating microscope, it is quite possible to carefully treat the wounds inflicted on the tooth and mend the poor thing. Which is what was done.
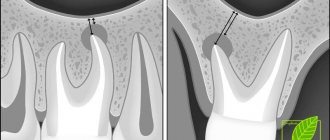
On an x-ray, the same picture looked like this: red lines show 3 root canals, a black dotted line shows the perforation zone, covered with a special material, and a red dotted line shows the inflammatory process in the bone tissue around the perforation zone.
After closing the root perforation , the main problem of this tooth, which led it straight into the hands of the surgeon, the root canals were re-treated and the root was thus preserved for subsequent prosthetics.
The process of removing debris from the canal
Even if the fragment does not affect the outcome of treatment in any way, a conscientious doctor will definitely inform his patient about the problem. This is necessary so that if the slightest discomfort is detected, a person immediately goes to the clinic, and does not treat the tooth with folk remedies at home. If the instrument breaks at the initial stage of the intervention before the infection is eliminated, the dentist must try to remove the part from the canal.
This will require a special dental microscope; without it, it will be simply impossible to detect such a small detail in a thin canal. At the first stage of the procedure, the doctor must create direct access to the foreign particle; for this he can use a dental bur.
Next, ultrasonic instruments with different tips come into play; it is with their help that the fragment can be removed from the dentin with minimal consequences. After this, the canal is thoroughly cleaned and sealed again, and medications are placed inside if necessary. A temporary filling is first placed on the tooth to ensure that there is no inflammation. After some time, you can put a permanent filling.
previous post
The dangers of teeth whitening at home
next entry
Instrument breakage and removal: two clinical cases
Every endodontist is faced with the problem of an instrument breaking off in the root canal. The task of removing a broken instrument from a root canal can be quite a challenge. The clinical outcome of treatment for instrument fracture depends on a number of factors, including the position of the instrument in the canal, the type of material, the size of the instrument, and the anatomical structure of the canal. The inability to extract part of the file does not necessarily mean that the treatment has failed. You can try to bypass the broken part, resort to surgery, or even just leave everything as it is and conduct dynamic monitoring. However, in any situation we must at least try to remove the broken tool from the canal.
Clinical case 1 A 27-year-old female patient was referred to our clinic. The score on the American Society of Anesthesiologists (ASA) scale was 1. The patient was bothered by pain in the area of tooth 46. When examined in the area of the apical part of the canal of tooth 46, a broken instrument was discovered, a diagnosis of “chronic periodontitis” was made, after which it was decided that it was necessary to remove the instrument before how the re-endodontic treatment of the canal will be carried out. Before starting treatment, a new diagnostic radiograph was taken, which revealed two file fragments: one in each of the medial canals (Fig. 1). The tooth was isolated using a rubber dam, the coronal filling was removed, after which direct access to the canal was provided: the latter is a prerequisite for the possibility of detecting instrument debris. To widen the mouth of the medial canals, Gates-Glidden burs (DENTSPLY Maillefer) were used. After the file fragment was located in the mesiobuccal canal, I modified the Gates-Glidden No. 3 bur by removing the instrument tip (Figure 2). Due to this, it is possible to create a more aggressive tool that allows you to form a platform over the fragment. At this stage of the work, the break of the tool in the channel was clearly visible (Fig. 3). ProUltra (DENTSPLY Maillefer) zirconium nitride ultrasonic tips were then used to release the file fragment.
Rice. 1. Diagnostic radiograph demonstrates two instrumentation fragments in the medial root.
Rice. 2. Modified GatesGlidden bur used to form a platform over the wreck.
Rice. 3. One of the file fragments.
1.5 hours after the start of the procedure, positive dynamics were noted, but the file fragment still could not be removed from the canal. We decided to leave him in the canal for a while and scheduled a follow-up visit. Calcium hydroxide paste (UltraCal XS, Ultradent) was injected into the coronal portion of the medial canals, after which the tooth was sealed with glass ionomer cement (Fuji IX GP Fast, GC) and covered with a cotton swab. During the second visit, the tooth was again isolated and exposed. The calcium hydroxide paste was removed using 10% citric acid and passive ultrasonication using an IRRISAFE handpiece (Satelec). Ultrasonic instruments were again used to locate the tool part. After 5 minutes, the broken instrument located in the medial buccal canal was removed. After another 5 minutes, we extracted a fragment of the file from the medial lingual canal. While removing the fragment from the mesiobuccal canal took a very long time, retrieving the file fragment from the mesiolingual canal was surprisingly easy. This example only confirms the variety of complexity levels of this procedure mentioned above. After extracting the fragments using an electronic apex locator (Root ZX Mini, Morita), the working length of the medial canals was determined. A conical clearance was provided; The medial canals were first shaped using a ProTaper S1 file (DENTSPLY Maillefer). Extensive medicinal treatment of the canals was performed using a 3% sodium hypochlorite solution. Gutta-percha was then removed from the distal canal using a ProFile file (DENTSPLY Maillefer) size 25.06 (rotation speed 500 min-1, X-smart Easy DENTSPLY Maillefer endodontic motor), without the need for chemicals to soften it. The canal walls were processed using a Micro-Debrider (DENTSPLY Maillefer) to remove any remaining gutta-percha. Final channeling was done using a 40.06 ProFile file. The apical third of the canals were shaped using K-Flexo files (DENTSPLY Maillefer). Removal of the smear layer of dentin was achieved by treating the canals with 10% citric acid. Final treatment of the canals was performed using a sterile solution. Then the conical gutta-percha pins were fitted (Fig. 4). Topseal material (DENTSPLY Maillefer) was used as a sealer. Obturation was performed using the continuous wave method using the Elements Obturation Unit (SybronEndo). After obturation, a temporary filling made of glass ionomer cement (Fuji IX GP Fast) was placed (Fig. 5). Final radiographs were taken (Figs. 6, 7). They demonstrate uniformly sealed medial canals; therefore, extracting file fragments from the canals had a positive effect. The patient with a favorable prognosis was referred to her dentist for final crown restoration.
Rice. 4. Fitting the gutta-percha cone.
Rice. 5. Pulp chamber after obturation with gutta-percha
Rice. 6. Final radiograph (parallel).
Rice. 7. Final radiograph (angular).
Case 2 A 19-year-old patient with no comorbidities was referred to our clinic with an ASA score of 1. The attending physician broke a small instrument—most likely a size 10 or 15 K-file, according to his accompanying letter—while treating root problems. canals of tooth 15. Endodontic treatment was required due to trauma suffered by the patient, as a result of which a crack formed and traumatic pulpitis developed. A new diagnostic radiograph was taken which showed a file fragment approximately 5 mm from the apex (Figure 8). The tooth was isolated using a rubber dam, then access to the canal orifices was provided through a temporary filling placed by the patient's dentist.
Rice. 8. Diagnostic x-ray shows a fragment of the instrument approximately 5 mm from the apex.
After this, the remaining calcium hydroxide was removed using a 10% citric acid solution and passive ultrasonic irrigation. The fragment of the file immediately became clearly visible due to the large width of the canal in the coronal and middle third (Fig. 9). This allowed us to use a very conservative and gentle approach. Taking into account the position of the canal and its shape, it was assumed that the canal branched in the apical part. Probing using small K-files made it possible to determine the position of the palatal canal.
Rice. 9. Tool fragment.
The instrument broke off in the buccal canal. To remove it, we used a ProUltra No8 titanium tip (DENTSPLY Maillefer) while simultaneously heavily medicating it with a 5% sodium hypochlorite solution. The file fragment was removed, and after determining the working length, we began to form the canals using rotating nickel-titanium instruments (Twisted Files, SybronEndo) (Fig. 10, 11). The final size of both channels matched the Twisted File tool size 25.08. Due to the branching in the apical area, a small master file was chosen to form the apical constriction, which was processed with extreme care, which avoided further damage to the instrument (Fig. 12).
Rice. 10. Recovered tool fragment
Rice. 11. Determination of working length.
Rice. 12. Branching of the canal in the apical part.
The final shaping of the apical third of the canal was done using size 25 K-flexo files. The smear layer of dentin was removed by treating with 10% citric acid. Final treatment of the canals was performed using a sterile solution. Then the conical gutta-percha pins were fitted (Fig. 13). After sealer treatment, both canals were obturated using the continuous wave method using the Elements Obturation Unit. After obturation (Fig. 14, 15), a temporary filling made of glass ionomer cement was placed, which was covered with a cotton swab; the swab is pre-moistened with a mixture of alcohol and chlorhexidine and then, after being placed in the access cavity, dried with air. Final radiographs were taken (Figs. 16, 17). A patient with a favorable prognosis is referred to his dentist for final restoration of the tooth crown.
Rice. 13. Fitting the gutta-percha cone.
Rice. 14. Obturation of the apex with gutta-percha.
Rice. 15. Pulp chamber after complete obturation with gutta-percha.
Rice. 16. Final radiograph (parallel).
Rice. 17. Final radiograph (angular).
Conclusion I would like to emphasize once again that removing a broken instrument from a root canal can be a very difficult task, the solution of which will require a lot of time. Dr. Marga Ree once said on the ROOTS magazine forum that the ESSENCE of endodontics is Passion, Perseverance and Patience. This formula is completely correct when it comes to extracting a file fragment from a channel.
Source: dental-tribune.com
Similar articles:
Ibrahim El Naggar
Huge perforation
Cancellation
The physician must be able to assess the current situation from diagnosis, treatment to prognosis, and be able to cope with various clinical surprises.
Ibrahim El Naggar Read Viresh Chopra
Endodontic treatment of the second lower molar
Cancellation
The article presents a case of irreversible pulpitis with symptomatic apical periodontitis of the mandibular second molar.
Viresh Chopra Read Daniel Flynn
Repeated endodontic root canal treatment: pros and cons
Withdrawal
Repeat root canal treatment is a predictable endodontic procedure. In the past, when telling patients about the prospects of retreatment, doctors often pointed to the possibility of failure.
Daniel Flynn Read L. Stephen Buchanan
Obturation using the continuous wave method for greater precision of the procedure
Cancel
I invented the Continuous Wave Obturation Technique (CWOT) in 1986 and continued through the winter of 1988-1989. I used it in combination with the Touch'n Heat device (SybronEndo).
L. Stephen Buchanan Read Mohamad Zaafrany
MB2: The Most Famous Missed Channel
Cancellation
Missed canal is one of the main causes of endodontic failure. During root canal treatment, MB2 is most often not found among the maxillary molars.
Mohamad Zaafrany Read
Calogero Bugea
Continuous wave condensation of gutta-percha
Cancellation
In 1987, Dr. Stephen Buchanan developed the continuous wave condensation technique for obturation of gutta-percha to simplify the Schilder technique of vertical condensation of heated gutta-percha.
Calogero Bugea Read S.S. Grigoriev
Evaluation of the quality of root canal filling with gutta-percha using optical microscopy and cone-beam computed tomography
Cancellation
Despite significant advances in clinical dentistry in the prevention and treatment of caries, complicated caries is a very common pathology of hard dental tissues.
S.S. Grigoriev Read CAE STANDARDS OF PRACTICE
Classification of clinical cases according to the level of complexity and risks
Cancel CAE STANDARDS OF PRACTICE Read Calogero Bugea
Bioceramics and adhesion: root canal preparation for fiberglass using the single cone technique
Cancellation
One of the controversial topics in endodontics and restorative dentistry is the relationship between the properties of endodontic sealers and the concept of adhesion.
Calogero Bugea Read Garima Poddar
Endodontic treatment of the lower first molar with a denticulate obliterating the bottom of the pulp chamber. Clinical case
Cancellation
This article describes a clinical case of endodontic treatment of a lower first molar with a denticulate obliterating the bottom of the pulp chamber.
Garima Poddar Read Mohamed Milad Ganawo
Clinical case of treatment of internal root resorption of the upper central incisor
Cancellation
This article describes a clinical case of internal resorption that began in the pulp and resulted in loss of dentin and possibly cementum from the root of tooth 2.1.
Mohamed Milad Ganawo Read Ahmed Shawky
Regenerative endodontics: a sustainable solution
Withdrawal
This case report describes successful regenerative endodontic treatment with a 42-month follow-up.
Ahmed Shawky Read
- ‹
- 1
Methods for removing a foreign body from a root canal
Specialists use two ways to remove a foreign object from the mouth of the dental canal:
- Simple. Used when pin elements are detected. The doctor uses an ultrasound machine to destroy the filling, then empty the cavity and remove the foreign body. Usually the procedure is quick and does not cause any difficulties.
- Difficult. The method is used if the doctor detects the presence of remains of a dental instrument in the root canal. At the same time, small parts of foreign bodies can only be detected using a microscope. The procedure is performed as follows: the doctor prepares the mouth of the tooth, loosens the detected foreign object using ultrasound and removes it with a special tool.
To carry out a high-quality procedure, the dentist must be highly qualified and have sufficient experience. Such doctors work in our clinic. They have the best modern equipment and skills in applying effective treatment methods. Our therapy is painless, quick and without complications.
Types of foreign bodies
Usually, foreign objects get into dental pockets during complex treatment. It can be:
- Broken endodontic instruments.
- Anchor or fiberglass pins.
- Parts of stump inlays.
Foreign bodies are any objects that should not be in the root canal after treatment is completed. If any body remains in the mouth of the tooth, it will interfere with the quality of the filling and will cause the formation of cracks and the development of inflammation. In this case, there is a risk of tooth loss. Therefore, foreign objects must be removed in a timely manner.