Signs Causes Types Diagnostics Treatment methods Consequences Timing Prevention Doctors Work
Mesial occlusion is a violation of the closure of the jaw, when the lower one protrudes more forward and the upper incisors overlap. This causes the patient not only psychological problems, lack of proper aesthetics, possible discussions of the defect from the outside, but also affects health in general. And the treatment of mesial occlusion in adults and children is long and difficult. There is work to be done from all sides: myofunctional gymnastics, massage of the alveolar process, the use of orthodontic structures and periodic visits to dental specialists.
What is mesial bite
Mesial (medial) bite is an anomaly of occlusion when the jaws do not close correctly. The forward position of the lower dentition towards the upper is noticeable even visually.
The mesial jaw occurs in up to 10%
of the total amount (quite often pathology is observed in the Mongoloid race). And unlike distal occlusion, mesial occlusion is diagnosed less frequently. However, all ages are susceptible to it.
Mesial displacement of the tooth is sometimes combined with other types of anomalies - open, cross bite.
The concept of progenic occlusion
With this defect, the lower jaw protrudes forward compared to the upper row of teeth. Because of this, the name “progenic” appeared. Pro genus is translated from Greek as “chin forward.” The concept of progenic occlusion includes two main meanings. Firstly, dentists use this term to describe the option of correct closure of teeth, that is, in fact, an absolutely normal bite. In other cases, the definition is used as a synonym for mesial malocclusion, which requires correction. Whether progenic bite is a pathological form or a type of physiological condition is determined by a number of additional signs:
- structure of the bones of the face and jaw;
- number of teeth and their size;
- shape of the dentition.
Both variants of progenic bite have their own characteristics, which are worth considering in more detail.
Progenic occlusion is an abnormal type of occlusion in which the lower dentition is located in front of the upper dentition, which causes aesthetic and functional disturbances.
Signs
Progeny of the jaw, as mesial occlusion is also called, is expressed by the following signs:
- the upper incisors are covered by a third by the lower antagonists;
- “strong-willed chin” protruding forward, the expression seems angry;
- ⅓ of the bottom of the face is visually more massive;
- lower lip thickened;
- the profile is concave, “month-like”;
- the change of baby teeth begins with the lower teeth and occurs quite early;
- asymmetry of the temporomandibular joint due to mesial occlusion;
- jaw clicking, sounds when yawning, chewing.
In addition to external, facial signs, intraoral symptoms can manifest themselves not only by reverse overlap of the incisors, but also by direct bite. The teeth of the lower jaw are directed towards the oral cavity; there may be three, diastemas, and crevices. Chronic periodontal diseases are often diagnosed.
Pathology of the mesial jaw is accompanied by a speech defect. The patient complains of difficulty biting food and gastrointestinal problems.
Typical symptoms
The expressed symptoms of the pathology are differentiated into two categories - external and internal signs. Typical external symptoms include:
- Significant advancement of the lower jaw;
- Distortion of natural facial symmetry;
- Change in the line of the mouth, manifested in protrusion or enlargement of the lower lip;
- Sharp delineation of nasolabial folds and sharpening of the chin.
The presence of such signs in itself is not yet a factor that allows us to unequivocally state the development of progeny. However, the presence of internal symptoms requires prompt attention to the dentist. These include:
- Speech defects and chewing dysfunction;
- Overlapping the top row with the bottom;
- Violation of jaw symmetry;
- Regular diseases of the oral cavity;
- Hypertrophic sizes of individual units.
Timely detection of pathology is the key to effective treatment carried out using one of the methods used in orthodontics.
Causes
The etiology of the causes of mesial occlusion is different. They can be congenital, acquired, genetic:
- heredity, structural features of the skull, facial skeleton in a generation;
- pathologies in intrauterine development, when a pregnant woman took strong medications or suffered a serious illness;
- short bridle;
- underdeveloped jaw (upper) or premaxillary bone;
- bad habits (thumb sucking, upper lip, for example);
- early eruption of lower primary teeth (however, any deviations in eruption can be the cause of mesial occlusion);
- osteomyelitis and other bone diseases;
- macroglossia (large tongue);
- removal of baby teeth ahead of schedule;
- previous rickets;
- supernumerary teeth.
In recent years, the percentage of detection of mesial occlusion has been increasing; scientists see the problem as a genetic predisposition.
Incorrect position during sleep (head lowered on the chest), habit of holding a fist, hands under the chin (sitting) can affect malocclusion.
Causes and etiology
There are several reasons for the appearance of this form of bite, but sometimes it can also be associated with genetic heredity. Factors that provoke the development of the pathological form of the disease include:
- absence of frontal teeth in the upper jaw area;
- damage to the body by chemicals or heavy metals during intrauterine development of the fetus;
- diseases during pregnancy leading to the development of disorders in the child’s dental system;
- atypical placement of tooth germs;
- congenital non-fusion of the palate with the alveolar processes, short frenulum of the tongue;
- mouth breathing with hypertrophy of the tonsils, chronic ENT diseases;
- injuries to the child when moving along the birth canal;
- macroglossia or large tongue, the pressure of which increases the parameters of the lower jaw;
- early loss of primary teeth;
- remaining bumps on primary canines;
- early childhood diseases (rickets);
- Incorrect placement of the baby's head in sleep.
When provoking factors appear, the physiological relationship between the masticatory and facial muscles is disrupted, which causes a strong impact on the lower jaw.
When there is a progenic disorder of the anterior teeth, the factors that cause the upper anterior teeth to develop incorrectly come first. This group includes:
- disrupted sequence of replacement of temporary teeth with molars;
- edentulous lateral incisors;
- supercomponent teeth that erupted in the frontal part from below;
- early appearance of the lower teeth with loss of the upper ones.
Classification
In dentistry, the classification of mesial occlusion is quite expanded and expanded over the last century. Even back in 2004, Persin L.S. proposed his own system of 9 classes, based on the experience of previous years.
- lower macrognathia (hyperdevelopment of the jaw);
- lower prognathia (the jaw protrudes significantly forward);
- upper micrognathia (underdevelopment of the jaw);
- upper retrognathia (displacement of the jaw deeper into the skull);
- superior micrognathia and inferior macrognathia;
- superior retrognathia and inferior prognathia;
- upper micrognathia and lower prognathia;
- superior retrognathia and inferior macrognathia;
- habitual protrusion of the lower jaw forward.
Mesial occlusion is distinguished by prognathia, which can be:
- true;
- false.
True
- pronounced facial asymmetry, severe speech impediment. It appears at an early age. This is macrognathia of the lower jaw and/or its prognathia. Correction of mesial occlusion must begin at the age of 5-7 years, for now in the form of therapy.
False
- the lower jaw is of normal size, and the upper jaw is underdeveloped and/or recessed into the skull. This type of jaw progeny cannot always be noticed at first glance. But x-rays and computed tomography give a clear understanding of the pathology.
Classification of the degree of curvature:
- First degree
- visually imperceptible anomalies, the size of the gap between the teeth is up to 2 mm, the lower incisors protrude slightly. - Second degree
- a “strong-willed chin” appears, the gap increases to 10 mm, the fangs of the lower jaw constantly touch the mucous membrane of the upper lip. - Third degree
- the lower jaw moves forward and it is clearly noticeable that it is larger than the upper jaw, the gap is more than 10 mm between the teeth, the incisors do not touch each other. Other abnormalities may be present—dental crowding is one of them.
The third degree of curvature is dangerous because almost always such mesial displacement of the teeth turns into an open bite. And it may not be possible to correct a mesial bite with braces.
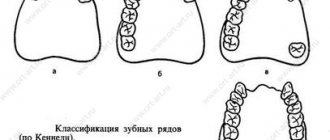
Another type of displacement separation by shape:
- dentoalveolar
- the lower jaw can fall into place on its own, move back with normal closure of the lateral teeth; - gnathic
- in this case, spontaneous shift is impossible; - mixed
.
We have not described all types; there are many classifications in the medical literature, as well as clinical cases.
Diagnostics
Diagnosis begins with a visual examination by a doctor, and this should be an orthodontist. To determine the degree of mesial occlusion, the following studies and actions will be needed:
- assessment of facial anomalies, asymmetry;
- measuring the proportions of the jaw using measuring instruments;
- X-ray, teleradiography, orthopantomography;
- CT scan;
- on the articulators, clarify the inclination of the incisors to the temporal region;
- use bite pads;
- taking impressions of the jaw.
When palpating the TMJ (temporomandibular joint), the patient may feel pain and discomfort. To determine further treatment: how to correct mesial occlusion without surgery or whether it cannot be avoided, complete information about the current condition is necessary. And all innovative diagnostic methods are used.
Features, methods, stages of treatment
The choice of correction method is influenced by the patient’s age and the degree of pathology.
Correction of mesial bite in children
The best period to correct any malocclusion is childhood. It all starts with a massage of the alveolar processes, then:
Myogymnastics
- for the little ones, up to 5-6 years old. Special oral exercises will allow the jaws to grow harmoniously. For older children, myotherapy is prescribed in addition to the main treatment.
Trainers
for patients 5-8 years old they help correct the bite. For 4-8 months they are worn at night. It is a silicone two-jaw mouth guard. Acts on the jaw muscles.
Plate
. From 8 years old, an orthodontic plate is offered. Plastic base with metal arches correcting mesial occlusion. There are many types and modifications: Frenkel activator, Bruckle apparatus, Andresen-Goipl Activator, etc. The choice of whether it will be a classic plate, with springs or another depends on the degree of pathology.
Orthodontic cap
. The child will have to stay in it for 6-8 hours. It looks like a corsage with elastic bandages that puts tension on the back of the head and chin.
Bracket systems
. Mesial bite can be corrected with braces from the age of 12. The structure is not removable. The impact of a metal arch with brackets on the teeth and jaw is constant. They wear it for about a year.
Braces with and without ligatures to correct bite
Treatment of mesial occlusion in an adult
For adults, treatment begins with braces or inexpensive orthodontic plates. But they will have to be worn twice as long as children. Since it is not always possible to correct a mesial bite without surgery, implantation and prosthetics are sometimes necessary.
In case of severe pathology, it is necessary to resort to surgical intervention. There are 2 types:
- gentle
_
For effective correction it is necessary to remove the teeth
. - traumatic
_
This is an operation
directly on the jaw. Its excision and forced fixation of the correct position using a structure made of titanium plates and screws. Stitches and plaster splints are applied and must be worn for 2 weeks. To consolidate the result, either braces or retainers are used.
Orthodontic treatment of pathology
There are several ways to correct a progenic bite. The choice in favor of one or another technique is given depending on the shape and severity of the defect, and also depends on the age of the patient and the general condition of the oral cavity. Treatment of pathology has three main directions:
- Limiting excessive development of the lower jaw. This correction is performed in children and adolescents no older than 15 years.
- Inward displacement of the lower dentition. This manipulation is relevant for adult patients.
- Correction of teeth position.
The listed measures are the main treatment, but additional and preventive measures are also important for effective correction. These include:
- treatment of inflammatory processes;
- getting rid of bad habits;
- normalization of chewing function;
- breathing correction.
Sources:
https://protezi-zubov.ru/prikus/progenicheskij-prikus.html https://dentazone.ru/ortodontiya/zubochelyustnye-patologii/progenicheskij.html https://zubneboley.ru/ortodontiya/progenicheskij-prikus-nuzhno- li-correction/
Consequences
If you do not correct the mesial bite, you can expect unpleasant consequences:
- recurrent migraines;
- jaw clicking when yawning and talking;
- pain appears when opening the mouth wide;
- facial muscle spasms;
- digestive problems;
- speech defects become stronger;
- aesthetics and appearance are lost, the face changes not for the better.
From the teeth:
- increased abrasion of enamel (even on baby teeth);
- interdental caries;
- bruxism;
- open bite.
The neglected condition of teeth and bone tissue due to mesial occlusion directly affects the impossibility or difficulty of implantation. This pathology cannot be ignored and correction should begin as early as possible.
Forecast and timing
90% of cases of mesial occlusion can be corrected by correction. It is better to start with baby teeth or mixed bite. Children's bones grow, and the probability of putting everything in its place in 1-2 years is extremely high. Correcting mesial bite with braces guarantees a positive result. This can be seen in the before and after photos.
Adult patients may need to consult several doctors: dentist, orthodontist, orthopedist. Treatment will not be quick - 1.5-4 years. And only following the doctor’s recommendations will help not only achieve results, but also consolidate them.