The maxillary (maxillary) sinus, despite its significant volume (up to 10 cubic centimeters), in a healthy person is hidden in the thickness of the bone of the upper jaw and does not betray its presence in any way. However, it is not so far from the mouth - the roots of an adult’s teeth sometimes reach it. In some cases, perforation of the bottom of the maxillary sinus is possible, meaning its direct connection with the oral cavity. This is possible due to some physiological characteristics of a particular patient:
- the close arrangement of the roots of the teeth can thin the bone border between the oral cavity and the maxillary sinus, from normal 1 centimeter to a very dangerous 1 millimeter;
- with low bone thickness, the roots of the molars can reach the cavity, separated from it only by the mucous membrane;
- a cyst, periodontitis or periodontitis can contribute to the thinning of the bony septum between the sinus and the oral cavity.
Perforation occurs against the background of the listed factors after dental intervention, even if the surgical technique was not violated.
Features of the maxillary sinus
The maxillary sinus (its other name is the maxillary sinus) is located in the thickness of the bone tissue of the upper jaw. It is separated from the oral cavity by the alveolar process of the upper jaw, which forms its bottom. The volume of such a sinus is quite large, and in adults it can reach 10 cubic centimeters.
This sinus, or sinus, is not airtight. It communicates with the nasal cavity through a narrow slit.
Typically, perforation of the maxillary sinus occurs in the area of its bottom. Some of its features contribute to this:
- Close proximity of the roots of molars and premolars. In some cases, the thickness of the bone layer between the tooth roots and the bottom of the maxillary sinus can be relatively large - up to 1 cm, but in some people the bone border between these formations is very thin - no more than 1 mm.
- Sometimes the roots of the first and second molars are located in the sinus cavity itself, separated from it by just a layer of mucous membrane.
- Rapid thinning of the bone layer in the presence of acute or chronic inflammatory diseases: periodontitis, periodontitis, cysts.
- Relatively thin bony trabeculae in the tissue of the upper jaw.
All this predisposes to the occurrence of perforation during dental procedures, even if the treatment technique was not violated and the doctor did not apply significant traumatic force.
What is this
Perforation of the maxillary sinus is a complication that a dentist can provoke during the process of removing chewing dental units located at the top.
This is due to the peculiarities of the anatomical structure, which affect the roots of the teeth and the bottom of the sinuses. Typically, the roots of the teeth of the upper jaw are separated from the bottom of the sinuses by a bone plate. In the area where the first 2 radical units are located, the plate is only 0.2-1.2 millimeters thick. In some cases, there is a pressing of the tops of such teeth into the sinuses. In addition, their protrusion further than the sinus floor may be observed.
The bone, which serves as a barrier separating the roots of the teeth from the maxillary sinus, can dissolve over time in the presence of periodontitis. This leads to the fusion of the tissue located in the lesion with the mucous membrane of this bone.
During the process of tooth extraction, a rupture of the mucous membrane occurs, and a symbiosis with the oral cavity is formed through the hole.
Causes of perforations of the maxillary sinus floor
The etiology of perforations of the maxillary sinus is always associated with any dental procedures. Perforation can occur:
- when removing teeth;
- during endodontic treatment;
- during dental implantation;
- during root resection.
When teeth are removed, damage to the bottom of the maxillary sinus can be a consequence of either rough actions by the dentist or failure to comply with treatment tactics, or as a result of the anatomical characteristics of the patient himself (for example, when the tooth roots are located directly in the sinus cavity).
When endodontic treatment is carried out, one of the complications is perforation of the tooth root, which is often combined with damage and perforation of the bottom of the maxillary sinus. This happens when the root canals are excessively expanded, when brute force is used when inserting pin elements or compacting filling cement. With this type of perforation of the maxillary sinus, filling material or root fragments almost always penetrate into its cavity.
If perforation occurs at the time of insertion of a dental implant (it can be an implant of any brand, for example, Mis, Nobel, Xive, etc.) or during root canal filling or insertion of pins into the tooth root, then it is always a therapeutic error doctor's tactics.
Damage to the bottom of the maxillary sinus is a serious complication when implanting artificial roots into bone tissue during prosthetics. This is explained by the fact that after tooth extraction, bone tissue very quickly undergoes degeneration processes. As a result, the height of the alveolar process of the jaw decreases. If the doctor does not take this point into account and incorrectly carries out preparations before implantation, and also incorrectly selects the size of the implant, then the risk of sinus perforation is very high.
Tooth root resection is a treatment method for the presence of cysts in the area of its apex. If the patient is underexamined, when the doctor does not know the exact size of the bone plate separating the bottom of the sinus from the wall of the cyst, and also if it is necessary to remove a large volume of jaw bone, then perforation of the maxillary sinus is not a rare phenomenon.
When is anastomosis closure required?
Damage to the integrity of the voids of the appendages, which are located on both sides of the nose, can occur during the removal of a tooth from the alveolus in the upper jaw.
The channel occurs due to the following reasons:
- quick removal of a dental unit using surgical forceps;
- an operation to implant an implant into the jaw bone tissue;
- urgent treatment of a complex tooth with inflammation;
- chronic periodontitis, in which the ligaments and plate of bone that hold the tooth in the socket become thinner and flake off.
When performing manipulations in the upper row of the jaw, a cavity or fistula may form. The danger is the possible spread of purulent fluid. The problem is solved by surgery.
Symptoms of perforation
If perforation of the nasal sinus occurred at the time of tooth extraction, then its symptoms will be quite specific:
- The appearance of small air bubbles in the blood released from the tooth socket, the number of which increases with a sharp forced exhalation through the nose.
- The appearance of bloody discharge from the nose on the side of the perforated maxillary sinus.
- Changes in the timbre of the patient’s voice, the appearance of “nasality”.
Sometimes the patient begins to complain about the passage of air through the hole after tooth extraction, as well as a feeling of heaviness or pressure in the projection of the maxillary sinus.
If perforation of the maxillary sinus occurs during implantation or endodontic treatment, the doctor may suspect it by:
- characteristic failure of the instrument or implanted element after applying some force to advance it;
- changing the position of the instrument in the wound;
- the appearance of small air bubbles in the blood.
If perforation of the maxillary sinus for any reason was not diagnosed and treated immediately, then its cavity becomes infected with the development of acute sinusitis or sinusitis, which is characterized by symptoms such as:
- severe acute pain in the maxillary sinus area;
- swelling of the nasal mucosa on the corresponding side with difficulty breathing through the nose;
- the appearance of purulent nasal discharge.
The appearance of general symptoms of intoxication is also characteristic: headaches, chills, high fever, weakness.
Diagnostics
Diagnosis of perforation of the floor of the maxillary sinus during tooth extraction is based on a typical clinical picture. In doubtful cases, as well as when such a complication is suspected during implantation or endodontic manipulations, it is necessary to use instrumental diagnostic methods:
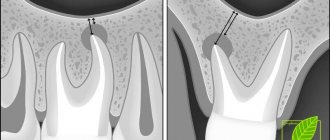
- Probing the socket of an extracted tooth or perforated canal with a thin probe . This allows us to determine that there is no bone bottom in the wound. In this case, the instrument passes freely through soft tissues and does not encounter obstacles along its path.
- X-ray of the sinus area . In this case, the pictures can reveal both darkening of the cavity due to the accumulation of blood in it, as well as fragments of dental roots, implants or filling material. Sometimes it is advisable to conduct radiography with contrast, when a contrast agent is introduced into the cavity through a perforation fistula.
- Computed tomography , which allows you to determine perforations and the presence of foreign bodies in the sinus with maximum accuracy.
- If old perforations are suspected, general clinical blood tests , the result of which may indicate the presence of an active source of infection in the body.
Treatment
Treatment of perforations of the maxillary sinus floor depends on what changes are present in the sinus cavity itself.
Treatment without surgery is possible only in cases where perforation occurred during tooth extraction and was detected immediately, and according to radiography there are no signs of infection of the sinus cavity or the presence of even minor foreign bodies in it. With this option, the doctor’s tactics are to preserve the blood clot formed in the socket as carefully as possible, as well as to prevent its infection. To do this, a small gauze swab soaked in iodine solution is inserted into the lower part of the hole. Usually it is tightly fixed in the wound cavity on its own, but sometimes sutures are required on the gum. This treatment with iodine continues for at least 6-7 days until full granulations are formed and the defect is closed. In this case, the tampon is not removed from the hole so as not to damage the blood clot.
It is also possible to temporarily close the defect with a small plastic plate, which is fixed to adjacent teeth with clasps. It separates the oral cavity and sinuses, which promotes healing of the perforation.
At the same time, a course of preventive measures is prescribed, aimed at preventing the development of inflammatory complications. It includes taking antibiotics, anti-inflammatory drugs, drops with a vasoconstrictor effect. This course is carried out on an outpatient basis or at home.
If, during perforation, foreign bodies penetrate into the sinus (implant, filling material, fragment of a tooth root), then treatment is carried out only in a hospital setting. In this case, an operation is indicated to open the cavity of the maxillary sinus, remove the foreign body and non-viable tissue, followed by plastic closure of the perforated defect.
»
How to treat
The fistula after sinus lifting and bone grafting is initially subjected to antibacterial therapy. In the case of a “fresh” fistula, broad-spectrum antibiotics are used: Lincomycin, Erythromycin, Summed.
If the pathological course persists for a long time, then a test is performed to determine the sensitivity of bacteria to antibiotics, after which the necessary drug is selected. The use of rinses and baths should be strictly limited due to the risk of penetration of the contents of the fistula canal from the oral cavity into the maxillary sinus. It is possible to use ointments with an antibacterial effect. In the presence of purulent discharge, punctures of the maxillary sinuses and fistula are performed in order to create outflow paths for pus.
After eliminating the pathogenic microflora, surgical intervention is performed to close the oroantral tract. The operation can be performed under local or general anesthesia - it all depends on the scope of the intervention and the patient’s wishes. It is possible to make a special mouthguard in advance to protect the operated area from microflora. The operation takes place in several stages:
- An additional hole is formed for insertion of the endoscopic probe. Using a probe, the maxillary sinus is inspected and the fistula tract on its side is closed.
- Dead tissue is excised and the fistula tract is closed using one's own tissue or artificial substitutes.
- The external opening of the fistula is closed with a mucoperiosteal flap on a vascular pedicle.
The postoperative period requires special attention to prevent re-infection. If the outcome is favorable, a repeat sinus lift and bone grafting may be performed after 1 to 2 months. After closing the fistula tract, the bone defect is not eliminated, which is felt by the patient as a “sinking” of tissue when pressing on the site of the existing fistula. The lack of bone tissue creates discomfort when eating.
Old perforations
If the perforation of the maxillary sinus was not promptly identified and eliminated, then after 2-4 weeks the stage of acute manifestations will subside, and a fistula will form in the area of the defect, connecting the sinus cavity with the surface of the gum.
This process is simultaneously accompanied by symptoms of chronic sinusitis:
- constant dull pain in the sinus area radiating to the orbit and temple;
- nasal congestion on the affected side;
- purulent discharge from the nasal cavity, as well as from the fistula;
- Sometimes patients have swelling of the cheek on the side of the damaged sinus.
Most patients also complain of a sensation of air moving through the fistula when talking or sneezing, difficulty pronouncing certain sounds, and liquid food entering the nasal cavity from the mouth.
Treatment of such chronic perforations with fistulas presents some difficulties, since the presence of a chronic focus of inflammation in the maxillary sinus significantly reduces the effectiveness of therapy and quite often leads to relapse and re-formation of the fistula canal.
Such patients are indicated for surgical intervention, which includes opening the maxillary sinus with removal of all non-viable tissues and foreign bodies from its cavity, excision of the fistula and plastic closure of the defect. Antibiotics after removal of the fistula are prescribed for a course lasting 10-14 days with the simultaneous use of anti-inflammatory and antihistamine drugs, and the use of physiotherapeutic methods of treatment.
Classification and complications of perforations of the maxillary cavities
Depending on the diameter of the hole, it is customary to distinguish:
- Small perforations - from five millimeters;
- Medium perforations - from six to seven millimeters;
- Large perforations - more than eight millimeters.
Depending on the period of development, the process proceeds:
- In acute form - it is detected either during the procedure or immediately after it;
- In its chronic form, it is detected only a few days after dental treatment.
Localization determines the presence of the following types of perforations:
- Palato-sinus - located on the palatal side;
- Alveolar sinus - located on the alveolar process;
- Vestibulosinus - located in the vestibule of the oral cavity.
Perforations that were not diagnosed on time always provoke infection and the development of inflammatory processes in the form of perforated sinusitis. The patient suffers from a feeling of nasal congestion and intense purulent discharge mixed with blood. Due to the entry of liquid food from the mouth into the sinus, infectious and inflammatory processes of the periosteum of the alveolar process and purulent lesions of the jaw bone develop.
Consequences of perforation
Perforation of the maxillary sinus is a fairly serious pathology that often has to be treated in a hospital. Attempts to independently treat it with folk remedies at home without medical assistance can lead to the development of serious and dangerous consequences:
- The development of a pronounced inflammatory reaction in the sinus cavity with the spread of infection to the surrounding bone tissue and the formation of foci of osteomyelitis of the upper jaw.
- Spread of inflammation to other sinuses of the skull (frontal, sphenoid and ethmoid).
- Loss of healthy teeth located in the area of untreated perforation.
- Formation of purulent foci (abscesses, phlegmons).
Due to the close location of the maxillary sinus and the brain, after perforation, infection may spread to the meninges with the development of meningitis or meningoencephalitis, which threatens the patient’s life.
Preventive actions
Prevention of perforations of the floor of the maxillary sinus consists of:
- in a full examination of the patient before complex dental procedures;
- in the correct assessment of the anatomical and topographical characteristics of each person;
- in strict adherence to the technology of therapeutic manipulations.
Timely detection of signs of perforation and its adequate treatment is the key to a favorable outcome for the patient. Incorrect therapeutic tactics or self-medication can aggravate the course of such a complication and cause the development of severe negative consequences.