- Indications
- Materials
- Manufacturing methods
- Stages of treatment
- Life time
- Care
- Prices
- Doctors
- Reviews
Provisional or temporary crowns are installed while preparing for permanent prosthetics. They protect sharpened teeth from the aggressive environment of the oral cavity, restore chewing function, the aesthetics of a smile, provide comfort during communication, and prevent gum growth until a permanent orthopedic structure is installed. The prosthesis is made from high-quality, non-toxic materials. Despite the fact that these are temporary orthopedic structures, their functional significance is very high. The cost of a temporary crown per tooth depends on the material, type of product, and manufacturing method.
- When to use:
Severely damaged tooth (temporarily) - Treatment period:
1 visit - Type of anesthesia:
Local - Healing period:
no - Procedure time:
5-15 minutes - Age restrictions:
From 18 years old
Why are provisional crowns needed?
- Prevention of changes in bite – eliminates the displacement of teeth in a row;
- protection from infections, thermal, chemical irritants to the tissue of prepared units;
- preventing gum growth around the stump;
- maintaining normal diction and correct pronunciation;
- restoration of chewing function;
- formation of an aesthetic gingival margin;
- prevention of mechanical damage to teeth and gums;
- adaptation to the volume and shape of the future permanent orthopedic system.
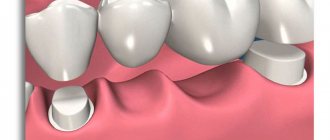
A temporary dental crown is installed on your own tooth, as well as on an implant, immediately after its implantation into the bone tissue using a one-stage protocol or 10-14 days before installing a permanent orthopedic structure using classical technology.
Temporary dental crown: when can you not do without it?
Dentists identify a number of situations that require the use of this orthopedic design. It happens:
- In the process of orthopedic treatment, when the teeth have already been ground, and permanent dentures are not yet ready for them;
- After installing the implants for the period of their engraftment, which can last from two to twenty-four months;
- In the process of individually creating permanent structures to evaluate their functionality in the future;
- In the process of gradually increasing the height of the dentition in order to prolong the therapeutic effect.
Materials
Various plastics (acrylic, polymethyl methacrylate PMMA) and composites are used for manufacturing. The materials reproduce different colors and shades, are quite durable, and can withstand moderate chewing load. For complex rehabilitation of multiple dental defects, metal-composite or metal-plastic structures on implants are used. Such prostheses consist of a lightweight metal frame lined with composite or plastic. The crown is secured with cement. It holds it firmly, but at the same time, the prosthesis can be easily removed for treatment and installed again.
Alekperov Roman Borisovich Dentist-orthopedist, doctor of the highest category
I got a temporary lab crown two months ago. It's time to do a re-prosthesis, but it hasn't broken and I'm satisfied with its appearance. How much longer can I walk with a prosthesis?
This question will be better answered by an orthopedist after examining the situation. The prosthesis has a service life that should not be exceeded.
Alekperov Roman Borisovich Dentist-orthopedist, doctor of the highest category
I got a temporary crown three months ago. Yesterday a corner broke off from it. How urgently do I need to come to the clinic for re-prosthetics?
A three-month period is the standard period for wearing a temporary prosthesis, which should not be much exceeded. If the corner of the crown is broken, the sharp edge can injure the mucous membrane and cause inflammation. If possible, you should come to our clinic as quickly as possible; if this is not possible, you should contact orthopedists at your place of residence so that they can polish the chip.
What problems do temporary restorations solve?
Temporary restorations can be used for all types of dental prosthetics, including when restoring a tooth with a single crown.
Let us list the main functions of “temporary” solutions:
- Restore the aesthetics of the smile while the permanent crown is being made (this is especially important if the missing tooth will spoil the smile)
- Protect the “living” tooth from reactions to temperature and chemical irritants, since after “crown treatment” the tooth becomes more sensitive
- If a pulpless (“dead”) tooth is being prepared “for a crown,” it should also be protected with a temporary crown to prevent re-infection of the tissues and strengthen it, since after “grinding” the tooth becomes more vulnerable to chewing loads
- If you leave a tooth “prepared for prosthetics” without a crown for some time, then while eating, food will put pressure on the gum and injure it. Inflammation of the mucous membrane may complicate the installation of a permanent crown in the future.
The material from which temporary crowns are made allows the doctor and dental technician to best select the shape of the new tooth , check how harmonious the smile looks after restoration, and only then implement the solution into a permanent crown.
The more complex the orthopedic design, the more nuances need to be taken into account, and the cost of error increases (correcting temporary restorations is faster and easier than correcting permanent ones).
Manufacturing methods
Provisional structures are made by direct and indirect methods.
- Direct
is an express technique that allows you to make a crown from plastic or composite in a matter of minutes
in the dentist’s chair
. The doctor takes an impression of the patient’s jaw using silicone paste, prepares the stump (grinds the tooth, giving it the desired shape). Fills a silicone impression with plastic material and places it on the tooth. After the material has hardened, an impression is taken, the prosthesis is given the desired shape according to the bite, firmly fixed with dental cement, ground, and polished. - Indirect
– a temporary plastic crown for a tooth is made in a dental laboratory, based on an impression of the patient’s jaw. The technique allows you to take into account the characteristics of jaw closure and the structure of the dentition. jaw movements. The prosthesis can be made in the laboratory in two ways - by a dental technician using the classical method or using CAD/CAM technology.
The direct method is economical, fast, but does not provide good aesthetics. Making a crown using the indirect method takes 1-2 days. The dentures fit exactly and are identical to natural teeth in shape and shade. Provisional structures made of thermoplastic material PMMA are reliable, durable, and suitable for patients with allergies to plastics.
Permanence of temporary ones: provisional crowns as a stage of orthopedic rehabilitation
Provisional restorations are often considered only as temporary or “transitional space retainers” that are secured to prepared teeth until the final restorations are fabricated. But in fact, provisional structures play an important role in objectifying the aesthetic, phonetic and functional parameters of future permanent restorations. After installing temporary structures, the doctor can begin to analyze the patient’s aesthetic profile and the relationship between the position of the crowns and the lip line. In addition, provisional restorations make it possible to check the adequacy of the restoration of the patient's phonetic function, based on the new position of the cutting edges of the crowns. And most importantly, provisional structures are an ideal tool for checking occlusal relationships and correcting them. Correct occlusal adaptation of temporary crowns minimizes the risk of their fracture or decementation. Therefore, provisional structures are not only temporary restorations, but also a powerful diagnostic tool in the structure of complex rehabilitation of dental patients.
Before fixing temporary structures
The doctor must carry out several preparatory steps before fixing the temporary crowns. First, it is necessary to assess all the patient’s risks, as well as objective and subjective needs. For this purpose, it is best to make a wax reproduction of future crowns. The contour of such should be restored taking into account all functional and aesthetic considerations and the wishes of the patient. Provisional crowns are not just a copy of a wax reproduction, they are the result of its appropriate adaptation based on the diagnostic analysis performed. The temporary restorations themselves also allow us to evaluate the contour of future permanent crowns and how well this fits with the patient's aesthetic and functional needs. After fixing the temporary ones, the doctor must take into account a number of objective and subjective criteria, based on which it will be possible to assess the success of complex treatment. The advantage of temporary restorations is that they can be easily adapted and adjusted directly in the patient's mouth, systematically approaching the formation of a new aesthetic profile and functional pattern, and it is these aspects that this article will focus on (Figure 1).
Photo 1. Functional aesthetic matrix (original approach by Peter E. Dawson)
Adaptation process for temporary restorations
You should always remember that form follows function. That is why, at the first stage of evaluating temporary restorations, it is necessary to ensure the presence of stable contact in the structure of the central occlusion in the projection of the lingual surface of the anterior incisors of the upper jaw (indicated by number 1 in photo 1). This retaining contact is directly related to the centric position of the temporomandibular joint, based on which a new stable occlusal scheme can be built. This contact is determined even on the wax reproduction when it is analyzed in a semi-adjustable articulator. Possible corrections can be carried out on the lingual surface of the anterior teeth of the upper jaw in combination with correction in the projection of the anterior edge of the incisors of the lower jaw. After confirming the presence of stable contact, it is necessary to analyze the interaction of the lips with the vestibular surface of the teeth in the second and third areas subject to potential correction (indicated by numbers 2 and 3 in photo 1). The doctor's goal is to recreate a smooth, convex contour in the cervical and middle third of the crowns. Excessively pronounced contours of temporary restorations should be leveled so as not to interfere with the natural movement of the lips along their surface. The absence of excessive contours also optimizes the process of adequate cleaning of provisional structures, which is extremely important for maintaining the health of the surrounding soft tissues. The fourth area for potential correction of temporaries is located at the crown margins (labeled 4 in Photo 1), and interventions in this area are performed to achieve proper horizontal and vertical incisal edge positions. When closing the lips, the cutting edge is “adjusted” in a horizontal direction relative to the red border. This manipulation eliminates the negative influence of the cutting edge of the upper anterior restorations on the movement of the lower lip when closing the mouth for swallowing and during speech. Determining the vertical position of the incisal edge is critical to individualize the functional aesthetic matrix. This stage is performed taking into account the condition of the lips during rest and the age of the patient. A famous study by Vig and Brundo found that at rest, younger patients had greater exposure of the maxillary incisors, while older patients had greater exposure of the incisal edges of the lower incisors. When transitioning from a resting state to a smiling state, the convexity of the cutting edges should be symmetrical with the convexity of the lower lip.
Checking the phonetic function in the formation of the sounds “F” and “V” is extremely important when assessing the horizontal and vertical position of the incisal edges during dynamic changes in the position of the lips during speech. The cutting edge of the upper incisors should interact unhindered with the outermost border of the lower lip. In the author's experience, if the patient strains, making weak sounds "F" and "V", then the mistake is often that the position of the cutting edges is too high, that is, the crowns themselves are too long. This error can be corrected by grinding the restorations in their vestibular-coronal third.
Once the position of the incisal edge has been verified visually and phonetically, the fifth step in the processing of temporary restorations is to integrate the esthetically desired and functionally required contour (indicated by number 5 in Photo 1). This is achieved by creating an anterior guide within the structure of the functional movement pattern. Having established a point of stable contact in the patient, the goal of the fifth stage is to allow the jaw to move passively down the palatal surface of the incisors until edge-to-edge contact is formed. Graphically, this trajectory looks like a smooth continuous line from the point of fixation of the central position of the jaw to the point of the cutting edge. If there is a conventional point where the line ends and then begins again, then the patient probably has distal contacts that prevent the jaw from opening. Removal of such distal interferences allows not only to form a proper anterior guide, but also to ensure adequate disocclusion of the chewing teeth and normalize muscle activity. After checking and confirming the trajectory of the jaw along the anterior guide, the doctor should transfer the patient to an upright sitting position. This is done to assess whether there is a need for wider contact to maintain centric jaw position, and also allows for harmonization of the functional pattern and trajectory of movement from outside to inside. Any noted interference with the above-described movement of the anterior teeth must be neutralized in order to ensure an unimpeded mechanism for closing the mouth. The sixth stage of testing and potential correction of temporary restorations involves analyzing the area of the tooth “belt” - from the projection of a stable centric contact to the gingival margin on the lingual surface (indicated by number 6 in photo 1). The goal is to create such a smooth transition in this area that it is not functionally noticeable and does not interfere with the tongue during the pronunciation of the sounds “S”, “T” and “D”.
To improve aesthetics, provisional structures must be sufficiently detailed by modifying angles, lines, surface texture, and the shape of interdental spaces. At this stage, it is extremely important to take into account all the patient’s personal wishes. For example, a patient may prefer more convex teeth instead of sharp angles. While the functional and phonetic components of crowns are under the control of the doctor and represent objective parameters, the aesthetic components are subjective, therefore, it is extremely important to take into account the patient’s wishes regarding the contour, shape, size and shade of future crowns.
After step-by-step inspection and correction of temporary crowns, they are classified as an approved option. The final contour of the provisional restorations is transferred to the dental laboratory for the production of permanent orthopedic structures based on their layout. The process of transferring information occurs through a set of clinical photographs, impressions and facial arch registers. The maxillary model with the final provisional restorations can be sent to the laboratory fixed directly in the semi-adjustable articulator. After the laboratory receives the latest approved version of temporary crowns, a comparison of the lower jaw model is carried out with them. At the same time, the position of the lower teeth in relation to the prepared teeth of the upper jaw is clarified. The laboratory can produce a matrix to control the reduction of hard tissues on the vestibular side with a special guide pattern for the cutting edge. These two key components provide the laboratory with the ability to analyze the three-dimensional (3D) relationship of the approved temporaries to the contour of the prepared teeth, which is essentially the functional esthetic matrix. Collaborating with a laboratory that understands the concepts of working with a three-dimensional functional aesthetic matrix is paramount to achieving predictable final results of successful orthopedic treatment. In fact, the final crowns are not something new; they simply repeat all the nuances of the final version of the temporary ones, only they are made not of bis-acrylic material, but of porcelain.
It is worth noting that although modern digital and CAD/CAM technologies continue to develop in dentistry, being a very effective tool for duplicating all aspects of temporary restorations on permanent structures, many practitioners still continue to use the analog treatment protocol, therefore it is important for them to take into account all the nuances modification and transfer of parameters of provisional structures to the laboratory. At the same time, it is necessary to remember the main thing: even with an analog protocol, robots can still achieve highly accurate rehabilitation results!
The following case example illustrates the sequential process of obtaining appropriate esthetics, phonetics and function on temporary crowns.
Clinical case
A 75-year-old man sought dental care for worn front teeth (Figure 2).
Photo 2. Situation before treatment: signs of pathological tooth wear.
After a complete diagnosis, a treatment plan was drawn up, which included making crowns for teeth 4-13, as well as teeth 20, 21, 28 and 29. In addition, it was planned to perform restorations in the projection of teeth 22-27 to restore the height of the crowns and stabilize the occlusion . Composite restorations in the anterior areas have been proposed instead of crowns in order to save the patient's financial costs. At the same time, the patient was informed about the possibility of replacing them with veneers later. After preparing the teeth and fixing the temporary crowns, special stop areas were formed on the lingual surfaces of the provisional structures of the anterior teeth of the upper jaw to stabilize the centric position. Thus, the height of the crowns of the lower front teeth was determined (photo 3-4).
Photo 3. Determination of the guiding vestibular-incisal edge of the lower incisors.
Photo 4. Stable contact points on the lingual surface of the upper anterior teeth.
The labial surface of the temporary restorations was then contoured to provide adequate support to the soft tissue of the lip so that it could move as freely as possible when smiling (Figures 5-6). Additionally, the length of the temporary structures of the anterior teeth of the upper jaw was checked so that they would not injure the lower lip when closing the oral cavity (photo 7).
Photo 5. Contour correction starting from the cervical area.
Photo 6. Correction of the contour of the middle third of the crowns.
Photo 7. Correction of the vestibular-incisal part of the crowns to create the possibility of free lip movements.
If there are any difficulties in the process of closing the lips, the doctor should first of all pay attention to the length of the provisional restorations. But before reducing the vertical parameters, you can first begin by contouring the labiolingual profile in the horizontal plane to achieve proper convexity of the vestibular surface (Figure 8). After checking the horizontal position of the temporary crowns, check their vertical position at rest. In this clinical case, given the patient's age, a slightly greater exposure of the incisors in a relaxed state is possible (Figure 9). When transitioning to a smile, the cutting edges should display a convex arc of a smile, and repeat the symmetry of the lower lip (photo 10) with a certain inclination of the plane of the teeth to the inner surface of the red border of the lips (photo 11).
Photo 8. Convex contour of temporary crowns in three projections.
Photo 9. View of the edge of temporary crowns at rest.
Photo 10. Equal convexity of the incisal edges of the upper anterior teeth in relation to the curve of the lower lip.
Photo 11. Equal convexity of the incisal edges of the upper anterior teeth in relation to the curve of the lower lip.
The horizontal and vertical position of the cutting edges was also checked using phonetic tests with the pronunciation of the sounds “F” and “V”. The patient was asked to count from 50 to 59 and observed for any phonetic obstructions in pronunciation. The presence of these indicates the need for correction of the coronal third of the crowns on the vestibular side.
The functional and aesthetic components were then analyzed: the patient was asked to clench the teeth together and then move the lower jaw to the right and left, as well as perform protrusive movements. The anterior guide should have a smooth trajectory from a stable centric relation position to the position of direct contact of the cutting edges of the anterior teeth (Figure 12). If there are any interferences in the distal areas, they are leveled out to stabilize the neuromuscular system of the entire dentofacial apparatus (photo 13-14). After this, the adequacy of the distribution of occlusal contacts is checked using articulation paper.
Photo 12. Front guide with a smooth trajectory.
Photo 13. Leveling of all distal interferences for free disocclusion on the right side.
Photo 14. Leveling of all distal interferences for free disocclusion on the left side.
The last contour that needs to be checked is the area from the tooth flange to the stop corresponding to the centric relation. This contour should be smooth and pronounced. The adequacy of its formation is checked through phonetic tests for the sounds “S”, “T” and “D”. After fixing the provisional structures, the patient used them for 1 week. After 7 days, all final corrections were made and occlusion parameters were recorded using a facebow. Impressions from the upper and lower jaws, bite registers and a new set of clinical photographs were also obtained. First, the models are compared with the facebow along with temporary structures (photo 15), after which the latter are removed and the models are compared without them (photo 16). After this, a matrix for vestibular reduction is formed along with a template to control the area of the cutting edges. The latter allows the ceramist to visualize the patient's functional aesthetic matrix in three-dimensional space (photo 18). It is essential that the ceramist work within this functional aesthetic matrix in order to reproduce all the formed aesthetic, phonetic and functional determinants tested in the preliminary preparation process. This approach is the key to creating final restorations with a predicted contour (Figures 19-20).
Photo 15. Comparison of models with temporary restorations.
Photo 16. Comparison of models with each other.
Photo 17. Making a matrix to control vestibular reduction and a template to control incisal edges.
Photo 18. Formation of a matrix for transmitting data about all the features of restorations to the ceramist.
Photo 19. View of the final crowns in the articulator.
Photo 20. View of the final restorations in the oral cavity.
Conclusion
Testing and evaluation of temporary restorations is essential to achieving predictable esthetic rehabilitation results. Using comprehensive diagnostic and verification tools, the clinician can provide the ceramist with basic information about the patient's lip dynamics and other functional determinants. Although provisional restorations are considered interim restorations, their importance should not be underestimated as they are not merely “temporary” but also influence the long-term functional and esthetic success of the final crowns.
Posted by Zachary S. Sisler, DDS
Temporary prosthetics of anterior teeth
Prosthetics with a temporary crown of incisors or fangs involves preserving the aesthetics of the smile. Prostheses are made in a laboratory (indirect) method. Select a shade of material similar to the color of the natural enamel of neighboring units. Installing a temporary crown on the front tooth allows you to make the intermediate stage of prosthetics more comfortable.
Plastic imitates enamel well and can withstand moderate chewing load. The procedure for installing provisional structures on the anterior or chewing units is no different. The only difference is that plastic structures on molars and premolars wear out and crack very quickly. If you plan to wear a provisional system for longer than 3-4 weeks, it is recommended to order lightweight metal-plastic or metal-composite prostheses.
Main materials of manufacture
The most affordable material is standard plastic. It is inexpensive and imitates a real tooth well. The only drawback is that it is not very durable, so you need to be careful before installing a permanent structure.
The second option is to use a more expensive, but also reliable acrylic structure. It is much stronger, looks beautiful and can be used longer. This is especially convenient if the production of a permanent crown will take much longer than you originally expected.
Stages of installing temporary crowns
- Tooth preparation
– the doctor gives the stump the desired shape (depulps, fills canals, strengthens with a stump inlay, grinds) - Taking impressions
– using an impression tray and plastic material, an impression is taken from the patient’s jaw - Making a crown
- the prosthesis is made directly (in the dentist's chair) or indirectly (in the laboratory) - Installation
- fixation of the temporary crown is performed with dental cement.
How is the installation carried out?
In order for the structure to be as stable, high-quality and durable as possible, the dentist must comply with the previously prescribed installation frequency.
The entire process of creating and installing a crown is planned in advance.
Therefore, at the preparatory stage, the dentist sees the patient, checks the current condition of the oral cavity and determines the need for treatment of varying degrees of complexity. The cost is calculated and the fastening method is selected.
After this, a decision is made on the placement of the temporary structure and the process begins.
Among the main stages:
- Anesthesia. To ensure that the patient feels as comfortable as possible, we use optimal anesthesia methods. They help relieve sensitivity locally.
- Preparation. This stage is also called tooth grinding. It is performed to provide the thickness needed for subsequent installation on top of an orthodontic structure with the desired structure, dimensions and other features.
- Creation of a temporary structure. As noted above, it can be carried out by direct and indirect methods. In the first case, everything happens on the day of treatment, in the second - after one or two days.
- Installation. After the crown is completely ready, it is placed in the prepared place. Dental cement is used as a material for fixation and fastening. Over time, it begins to dissolve on its own. The substance is designed to break down on contact with saliva. Moreover, the composition is completely safe for the body - the substances are not deposited in the internal organs and are quickly eliminated naturally.
The doctor schedules a visit, during which the temporary structure is replaced with a permanent one. All that remains is to come to the appointment and exchange the acrylic or plastic version for a new one.
Care
- Brush your teeth thoroughly twice a day, without putting excessive pressure on the denture;
- limit the chewing load in the area of prosthetics;
- eliminate hard, sticky foods;
- limit foods and drinks that can stain the prosthesis material (coffee, tea, red wine, etc.);
- do not wear the device for longer than the period recommended by the dentist;
- If the prosthesis is displaced or damaged, immediately contact the dentist.
Article Expert
Alekperov Roman Borisovich Dentist-orthopedist, doctor of the highest category
Work experience: more than 32 years
What else do you need to know about “temporary solutions”?
Perhaps many people believe that doctors, when drawing up treatment plans, are guided by their own experience and treat “as they see fit.” This is not entirely true.
The treatment methods used by doctors are based on clinical recommendations and protocols that are developed by international and Russian professional medical associations.
Regarding “temporary” crowns, the Russian Dental Association recommends the use of temporary dentures as a cosmetic and functional guideline for the manufacture of permanent denture structures.
Therefore, if a doctor suggests using a temporary one before installing a permanent crown, this is not a desire to delay treatment and earn more money, but to follow personal clinical experience and the recommendations of authoritative colleagues. And all this in order to guarantee the patient a successful treatment result as much as possible.
Question No. 10: how is the restoration removed?
Today, many patients know that permanent restorations are not easy to remove. In most cases, it has to be sawed and removed using a special tool. The procedure, although painless, is unpleasant.
Read the article on the topic: “5 ways to remove an artificial crown from a tooth.”
However, with a provisional structure everything is much simpler, because it is fixed with temporary cement. To remove it, the doctor uses an ultrasonic tip that breaks up the cement. Next, the specialist uses forceps to remove the cap from the mouth.
The photo shows pliers for removing temporary crowns
As for temporary crowns on implants, removing them is even easier, because they are fixed with screws: the doctor simply removes the masking layer of the composite from the outer part of the crown and unscrews the screw.
Notice
: Undefined variable: post_id in
/home/c/ch75405/public_html/wp-content/themes/UltraSmile/single-item.php
on line
45 Notice
: Undefined variable: full in
/home/c/ch75405/public_html/wp-content /themes/UltraSmile/single-item.php
on line
46
Rate this article:
( 2 ratings, average: 5.00 out of 5)
crown
- Petrosyan A.A., Dobrovolskaya P.E. Production of provisional crowns for prosthetics on implants with subsequent formation of the occlusal surface // International Journal of Applied and Fundamental Research. – 2016.
Expert “Some patients neglect doctors’ recommendations about the need for timely replacement of such temporary crowns and continue to wear them until the effect of the temporary cement is disrupted. However, this can lead to inflammation starting under the structure. As a result, the tooth will be destroyed and will have to be removed.” Orthopedist Chorny Stanislav Vladimirovich
Consulting specialist
Dzagurova Elina Ruslanovna
Doctor rating: 9.5 out of 10 (2) Specialization: Dentist-therapist Experience: 11 years
The main functions of such prostheses:
- protection of the pulp from the negative influence of pathogenic microorganisms;
- preventing displacement of treated and adjacent teeth;
- formation of the gingival margin and prevention of gum growth when treating teeth with a special ledge;
- reconstruction of occlusion during therapy for increased wear of chewing elements;
- continuation of the full functionality of teeth;
- acceleration of adaptation to the modernized chewing element, which will take the place of the affected one after installation;
- maintaining the aesthetic appearance of the oral cavity.
Many people are concerned about the question: how long can temporary crowns be worn? The answer is simple - the entire period allocated for the manufacture of permanent dentures.
This may even take a couple of months. When these orthodontic structures are worn for a long time, they wear out, which will lead to the displacement of adjacent teeth.
Inflammation of the gingival margin also occurs due to bacterial contamination of the plastic. Sometimes the crown breaks, followed by gum growth and pain.
The production of such crowns is much faster than their permanent counterparts.
Regardless of what material modern crowns are made from, they are fixed with temporary cement. Such material gradually dissolves under the influence of saliva.
Sometimes it becomes necessary to attach temporary dentures after implantation. This is because it is important for the gums to return to the desired shape after this type of intervention, and non-permanent crowns can help with this.
Before installing a permanent prosthesis, the implant must take root. The average period of its integration in the upper jaw is about six months, and in the lower jaw – 4 months.
The lower jaw is better supplied with blood, and it is larger and stronger, since it bears more chewing load.
While it takes root, the patient wears a temporary crown, which imitates a regular tooth, protecting the gums from inflammation.
Dentures are placed on an implant when the dental nerve is removed and it is not possible to restore the chewing element.
Why are such prostheses needed - functions and purpose?
What are temporary crowns needed for, and why are they placed? The manufacture of any permanent dentures requires a certain amount of time – usually three or more days. At the same time, the supporting teeth have already passed the processing stage and do not look quite aesthetically pleasing - after all, they are quite sharply ground. Therefore, if the question arises - why are temporary crowns placed before permanent ones, you need to understand that they serve the following purposes:
- protection of the ground tooth and surrounding gums from mechanical damage: during chewing food or brushing with a toothbrush. Inflammation of the gums or dental “nerve” should not be allowed. It is also necessary to maintain the shape of the support, because the permanent “cap” is made using casts from the support – and if it breaks, you will have to start prosthetics “from scratch”
- protection from external irritants: acids, temperature changes,
- restoration of dental aesthetics,
- restoration of the functionality of the tooth: of course, in this case its “functionality” will be incomplete, because strong chewing pressure can damage the root or implant,
- acceleration of adaptation to a permanent prosthesis,
- normalization and correction of the position of the gums, if such a crown is placed on a newly installed implant.
Only until 15.01 South Korean implant Osstem - from 18,500 rubles.
Hurry up to sign up for a free consultation and lock in promotional prices.
Call now or request a call
Opening hours: 24 hours a day - seven days a week
Question No. 8: how to care for temporary restorations?
Care must be carried out carefully, but very carefully. To begin with, you should buy a brush with soft bristles and a toothpaste without abrasive particles (it should not be bleaching!). If you use “harsh” hygiene products, there is a risk of prematurely damaging the artificial material and ruining its appearance.
For complete oral care, it is recommended to purchase an irrigator, because you have a temporary prosthesis installed. At the junction with the gum, plaque must be removed more carefully, since this is where it accumulates the most. The irrigator also helps to care for the gums, the health of which is very important for the safety of the teeth and the restorations themselves. With the help of a directed jet, the mucous membranes can be gently massaged, increasing their blood flow.
Using an irrigator will help with oral hygiene
If an irrigator and a brush with soft bristles are ideal assistants in the fight against contamination of artificial material, then you should be very careful when using floss. Some doctors advise avoiding flossing altogether, as the teeth and gums under the structures become less sensitive, and if the cleaning technique is incorrect, there is a risk of injuring the mucous membrane. In addition, careless use of thread can cause breakage or peeling of the prosthesis.
If you still use floss, remember that after use it is better to carefully pull it out of the interdental space by only one end.
If you have provisional restorations, it is better to stop smoking and consuming products with dyes, as they change the shade of artificial materials. Also, you should not lean on hard and sticky food, because this can destroy your artificial teeth ahead of time, or lead to their deformation.
Why do we need temporary crowns on teeth - what they are and how long they are worn
Article navigation
- What are temporary crowns?
- Functions and purpose
- Types of temporary crowns
- How long does the service life last?
- Advantages and disadvantages
- Manufacturing methods and installation
- Is it safe to use temporary prosthetics?
- How to remove a prosthesis
- Rules for wearing, care and adaptation
- Cost of products
Question for a specialist
Gold crowns are familiar to every person - they are a classic of prosthetics that are already becoming a thing of the past. Now there are more modern materials - metal ceramics, ceramics, zirconium dioxide and ceramic composite. And all of them are used for permanent dentures that are worn for years. But there are also temporary dental crowns that need to be worn for a shorter period of time. In today's material we will talk about all the features of temporary crowns - their types, why they are needed, how they are made and placed, how long they are worn, as well as the cost.