Inflammation of the maxillary sinuses is not the most dangerous disease today. The large number of effective antibiotics makes treatment of this disease relatively simple. However, if left untreated, sinusitis can cause serious complications. It is known that everything in the human body is interconnected. The source of infection and inflammation in the nasopharynx can spread to other parts of the head. The most dangerous are meningitis and cerebral edema.
Sinusitis can be acute or chronic. The acute form of sinusitis most often occurs due to infection entering the nasopharynx. The causes of this disease are viruses, bacteria or fungi. Most often, sinusitis occurs against the background of a viral infection. Inflammation of the maxillary sinuses caused by a fungal infection is difficult to treat.
In addition, inflammation of the paranasal sinuses can occur as a result of its injuries, which can lead to disruption of the anatomical structure of the bone walls of the nasal cavity and sinuses. Also, sinusitis often appears after a long allergic rhinitis.
Chronic sinusitis occurs in the absence of proper and timely treatment of the acute form of the disease. Treatment of chronic sinusitis requires much more time and effort. Therefore, it is better not to bring your body to such a state.
Main symptoms of sinusitis
The main and most well-known symptom of inflammation of the maxillary sinuses is headache. In some cases, pain can cause a lot of inconvenience; in rare cases, the pain reaches such heights that it is necessary to take painkillers. At the beginning of the disease it has a certain localization. With sinusitis, discomfort occurs in the forehead, nose and around the eyes. However, after some time the pain becomes irritating, affecting many areas of the head.
The pain of sinusitis can sometimes be very similar to the pain of a migraine. However, sinusitis also has other symptoms, which, coupled with headaches, allow the doctor to diagnose this disease quite accurately. To confirm the diagnosis, radiography of the paranasal sinuses is used.
On x-rays with sinusitis, shadows are clearly visible, in which you can guess the fluid accumulated in the maxillary sinuses of the nose. This liquid is a mixture of mucus and pus. It is the accumulation of exudate in the maxillary sinuses that is responsible for the appearance of headaches, as it puts pressure on the inflamed mucous membrane and causes discomfort.
Headache with this disease can intensify when bending the body forward, as well as from sudden movements of the head. To minimize discomfort, the patient needs rest. There are also other symptoms of inflammation of the maxillary sinuses:
- nasal discharge;
- nasal congestion;
- swelling of the soft tissues of the face, eyelids;
- increased body temperature;
- weakness, irritability.
These symptoms are characteristic not only of sinusitis, but coupled with a severe headache, they indicate precisely this disease. If you suspect an inflammatory process in the maxillary sinuses, you should immediately consult a doctor and undergo an examination to confirm the diagnosis. Untreated sinusitis can have serious consequences for the body.
Tumors of the nose and paranasal sinuses
The classification identifies the following tumors.
- Benign.
- Congenital: cerebral hernias, teratomas, angiomas (lymphangiomas and hemangiomas).
- Highly differentiated non-malignant neoplasms of the nose and paranasal sinuses: fibroma, osteoma, chondroma, angiofibroma, neurinoma, papilloma, adenoma, etc. Papilloma and adenoma belong to epithelial tumors.
- Craniosinus tumors emanating from the cranial cavity and growing into the nasal cavity and its sinuses: meningioma, angiofibroma, cavernous angioma, chondroidchordoma, chordoma, neurinoma, pituitary adenoma, cementing fibroma (cementoma), teratoma, osteoma.
- Malignant. Highly differentiated malignant and differentiated tumors (epithelial, connective tissue and originating from pigmented neuroectoderm).
There are 4 stages in the development of a malignant tumor process.
- Stage I - limited tumor.
- Stage II - tumor growth into adjacent anatomical formations in the absence of metastases (II a). Presence of mobile regional metastases (II b).
- Stage III - tumor growth beyond the upper respiratory tract system in the presence of mobile metastases (III a). Presence of fixed reshonar metastases (IIIb)
- Stage IV - tumors growing into the base of the skull (IVa). Presence of distant metastases (IV6).
The extent of tumor spread is indicated as follows.
- I degree (T1) - the tumor affects one anatomical part.
- II degree (T2) - the tumor affects two anatomical parts.
- III degree (TD) - the tumor extends beyond the organ.
- IV degree - the tumor grows into the bones.
Regional metastases of tumors of the nasal cavity and paranasal sinuses develop at a late stage in the submandibular lymph nodes. Highly differentiated malignant tumors metastasize to distant organs.
- The absence of metastases is designated as N0.
- Unilateral mobile metastases - N1.
- Movable double-sided - N2.
- Fixed one- or two-sided - N3.
- Distant metastases - M.
High quality. Poorly differentiated and undifferentiated tumors.
Clinical characteristics. The clinical course of all benign tumor processes in the nasal cavity in the first stages of development is identical.
The first symptoms of the disease do not have specific features. The child is worried about unilateral or bilateral persistent sharp difficulty or absence of nasal breathing, hypo- or anosmia, purulent runny nose, spontaneous nosebleeds of varying intensity (in case of vascular tumors, profuse).
Later, headache occurs, with widespread growth, displacement and bone destruction of the walls of the paranasal sinuses, curvature and displacement of the nasal septum, hard palate with facial deformation occur.
When the tumor grows into the orbit, zygomatic region and alveolar process, a number of signs are observed: diplopia, lacrimation, scleral injection, exophthalmos.
When the tumor spreads into the oropharynx, respiratory failure and dysphagia are observed.
Pain syndrome is uncharacteristic and occurs when the alveolar process of the upper jaw, pterygopalatine and retromaidibular fossae, and orbit are affected.
Subsequent clinical course varies.
The volume of a cranial hernia can increase with screaming, coughing and crying. Subsequent histological examination reveals the medulla or meninges in the hernia sac.
Teratoma usually fills the nasal cavity and nasopharynx, is detected already in the 1st year of life, causes disruption of nasal breathing, sucking, dysphagia in children, and aspiration syndrome in some newborns.
The pedicle of the tumor is usually fixed on the side wall of the nasal cavity or nasal part of the pharynx; its wide base is tightly fused to the posterior surface of the soft palate.
Treatment is surgical. During microscopy, the rudiments of all types of tissues are found in the tumor stroma.
angiomas are most often observed . They can be of various shapes and sizes. There are stellate angiomas of the newborn, regressing within several months, cavernous angiomas or resembling a cyst.
They are localized in the area of the vault of the nasal cavity, on the border of the bony and cartilaginous sections of the nasal septum, in the anterior sections of the lower and middle nasal concha.
The tumor has a round shape, soft consistency, dark purple color, sometimes with a bluish tint, uneven surface, wide base, is easily injured and bleeds.
Microscopically, vascular tumors consist of many capillary and sinusoidal vessels with a small amount of connective tissue stroma; have the structure of lymphangiomas or cavernous angiomas, simple capillary, branched, mixed type with capillary, venous and arterial vessels. They often recur.
Benign tumors have a slow expansive growth, clinical symptoms gradually increase, and there is no metastasis.
Soft pashomas have a soft consistency, loose edematous stroma surrounding a thin-walled blood vessel, and are covered with columnar epithelium.
Papillomas are pinkish in color and bleed easily. They can be localized in the area of the anterior end of the inferior turbinates of the nasal septum, sometimes grow into the surrounding tissues (mainly into the maxillary sinus), and often recur.
Adenoma is most often localized in the region of the anterior ends of the lower and middle turbinates, in the ethmoid and maxillary sinuses. It has the appearance of a dense encapsulated node on a wide base, grayish or brown in color, with a smooth surface, covered with a thickened mucous membrane. Has expansive growth. Microscopically, it is built from atypical mucous glands, lined with columnar or cuboidal epithelium, with a high content of goblet cells.
Adenomas of the medial wall of the nose grow slowly, benignly, and those of the lateral wall grow rapidly; as they grow, they destroy other structures and relatively quickly grow into the paranasal sinuses, are accompanied by spontaneous bleeding and often become malignant.
Osteoma macroscopically has the appearance of a chacha with numerous grooves and grooves, a smooth surface, and a rounded shape. The consistency is dense, immobile, painless, gives an intense shadow on the radiograph. In the initial period it is not accompanied by any symptoms. On the cut, the tumor has the appearance of compact, less often cancellous bone.
As it grows, headaches appear, signs of damage to surrounding tissues and organs (facial disfigurement, displacement of the eyeball), and often grows into the cranial cavity.
Microscopically, the typical structure of osteomas of another localization is noted.
Chondroma is localized mostly in the area of the cartilaginous part of the nasal septum, in the maxillary, ethmoid and sphenoid sinuses; can reach a large size with facial disfigurement.
It grows slowly, growing into blood vessels, and can metastasize.
Macroscopically, the tumor has a smooth surface, less often lumpy, located on a wide base, dense consistency, pale pink in color, often lobulated, similar in appearance to cartilage.
Microscopically, it does not differ from chondromas of other localizations, built from hyaline and fibrous cartilage.
Chordoma has a hemispherical or mushroom-shaped bowl, a soft gelatinous consistency, a lumpy surface, and is surrounded by a capsule.
Microscopically, the tumor has an alveolar structure, the parenchyma consists of large round and lamellar cells with pyktnotic nuclei. The protoplasm, along with glycogen and liggids, contains numerous vacuoles. The main intercellular substance is rich in acidic mucopolysaccharides.
Angiofibroma of the base of the skull arises from the dome of the nasopharynx, the pharyngeal-basic fascia, or the region of the pterygopalatine fossa. Benign in histological structure, its clinical course is similar to malignant: infiltrating destructive growth, debilitating nosebleeds, invasion into the paranasal sinuses, orbit and cranial cavity, frequent relapses after surgery. The surface of angiofibroma is smooth, the consistency is dense or densely elastic; the superficial mucous membrane is shiny, with a pronounced vascular pattern.
In young children, the course of the disease is much more aggressive than in older children.
The microscopic structure varies depending on the age of the patients and is determined by the different ratio of vascular and fibrous components:
- in the active growth phase of the tumor, the vascular component predominates; the largest vessels are located at its base, smaller and less organized ones depart from them; at the surface, spongy structures are identified in the form of slits and sinusoids lined with endothelium; the tumor stroma at this stage is edematous, rich in stellate or elongated cells with myxoid areas;
- in “old” tumors the vascular component is less pronounced, the stroma becomes less cellular and more fibrous; in a growing tumor, ulcerated fragments of the surface with local inflammatory infiltration are detected.
Removal is extremely difficult due to massive, difficult to stop bleeding.
Hemangiopericytoma. Vascular tumor with a characteristic perivascular arrangement of proliferating cells from periocytes, soft, polypoid, gray in color, with locally destructive growth. There is a marked disturbance in nasal breathing and frequent spontaneous nosebleeds.
Fibrous dysplasia has the appearance of “bloated” bone with a thin inner cortex. It affects the area of the nose, paranasal sinuses, and possibly multiple lesions of the bones of the facial skeleton and skull with progressive facial asymmetry as the tumor spreads to the zygomatic bone and orbit. It is characterized by slow growth, difficulty in nasal breathing, and headaches.
X-ray reveals intense darkening of the maxillary sinus, sometimes outlined foci of clearing with a demarcation border of sclerosis at the edges.
Neurofibroma and neurilemmoma (schwannoma) are characterized by slow, uniform growth, compression of surrounding tissues without infiltration.
Histologically, they are manifested by the presence of dilated vessels with their thrombosis and hyalinosis of the walls.
Symptoms depend on the size of the tumor. Nasal deformation, exophthalmos, and paresthesia are possible.
Myxoma occurs in the nasal cavity and in the maxillary sinuses, and has the appearance of a soft node in the thickness of the mucous membrane.
Constructed of loose, soft-fibrous tissue with a large number of young fibroblasts; there are areas of mucus rich in hyaluronic acid, poorly vascularized. Characterized by infiltrating growth, recurrent course without metastases.
The clinical course depends on the size and direction of tumor growth. When localized in the nasal cavity, in advanced cases it can grow into the orbit and cranial cavity.
Craniosinusonasal tumors can be relatively limited with predominant extracranial growth and widespread with massive damage to the anterior and middle cranial fossae, as well as with invasion into the pterygopalatine, infratemporal fossa with gross deformation of the hard palate, bone walls of the external nose and paranasal sinuses.
The degree of extracranial spread of the tumor into the nasal cavity varies - from partial damage to the superoposterior and middle sections, to complete obstruction of the nasal cavity.
The features of these formations are purulent or purulent-polyposis sinusitis, the formation of mucocele and pyocele, nasal liquorrhea, pneumocephalus, gushing nosebleeds, the frequent occurrence of infectious complications in the cranial cavity, and blood entering during bleeding from the nasal cavity and its sinuses directly into the cranial cavity.
The color and consistency of the tumor depend on its histological structure:
- angiofibroma is bright red;
- meningiomas, often nodular, in the form of pale pink, lumpy, densely elastic or soft tumors, not fused with the lateral walls of the nasal cavity, emanating from the upper anterior and upper posterior sections;
- cementomas are dirty gray in color;
- most benign tumors have a soft elastic consistency, smooth or bumpy surface;
- chordoma, cementoma and neuroma have a bone or cartilage-like density.
Tumors rich in blood vessels are characterized by severe nosebleeds and impaired sense of smell.
Malignant tumors have the following signs: rapid infiltrating growth with destruction of bone walls and ingrowth into the paranasal sinuses, uneven surface, severe bleeding upon probing, immobility due to fusion with surrounding tissues, foul-smelling discharge, metastasis.
Malignant tumors of the nasal cavity and paranasal sinuses are usually primary.
Epithelial undifferentiated tumors include cancer. The tumor is localized in the nasal cavity, especially often in the maxillary sinus. There are exo- and endophytic forms. In the exophytic form, a polypoid, tuberous tumor of gray or pale pink color is formed on a wide base. In the endophytic form, the tumor has the appearance of a lumpy, dense infiltrate, covered with a hyperemic mucous membrane.
The tumor ulcerates early with the formation of a deep ulcer with “dirty” edges and bottom, metastases are detected early in the submandibular lymph nodes. Possible profuse arrosive bleeding.
Characterized by rapid germination into surrounding organs, into the orbit, into the cranial cavity with the development of meningitis, brain abscess, and damage to the cranial nerves. When they grow into the paranasal sinuses, empyema .
Death occurs from progressive cachexia, bleeding, pneumonia, sepsis, meningitis.
Histogenetically, cancer is associated with the integumentary epithelium and glandular epithelium.
Histologically, squamous cell keratinizing and non-keratinizing cancer, adenocarcinoma, solid or papillary poorly differentiated cancer are distinguished.
In children, squamous cell carcinoma is more often observed, which usually develops from metaplastic epithelium. Connective tissue undifferentiated tumor - sarcoma of the nasal region is less common, mainly originating from the periosteum of the ethmoid labyrinth and the perichondrium of the nasal septum and external nose.
Based on their microscopic structure, osteo-, chondro-, myxo-, angiogenic, synovial sarcomas, and lymphosarcoma are distinguished. Often the tumor is so anaplastic that it is impossible to determine its histogenesis.
Macroscopically, exo- and endophytic forms are distinguished.
In the exophytic form, the tumor has the appearance of a smooth or coarsely tuberous polyp-like node on a wide base; For quite a long time, compared to cancerous tumors, it remains covered with an unchanged mucous membrane. The consistency of the tumor depends on the degree of its anaplasia. On the section, the tumor is whitish or whitish-pink in color, homogeneous.
The endophytic form is characterized by a dense, tuberous infiltrate. Only when the tumor is large does it ulcerate, and then its surface has the appearance of an ulcer with a dirty gray bottom.
Sarcoma grows faster than a cancerous tumor, although it disintegrates and metastasizes relatively late. It is usually large in size, dense, lumpy, inactive or immobile, bleeds when touched, and is less likely to grow into the cranial cavity. Recurrent tumors, on the contrary, are characterized by rapid growth. Characteristic features include early development of purulent runny nose, foul-smelling discharge and bleeding.
Subsequently, as the sarcoma grows, the following symptoms occur. Various pain sensations - from simple heaviness in the head to acute trigeminal neuralgia. Then, as it grows into the surrounding tissues, swelling of the bones, displacement of neighboring organs, metastases, general anemia, and cerebral phenomena are observed.
Sarcoma grows extremely quickly, grows into the paranasal sinuses, grossly deforming the facial bones, especially in young children, due to the separation of the nasal bones and growth through the cavities under the soft tissues of the face.
Cancer and sarcoma in children most often affect the maxillary sinuses; at first they are asymptomatic, then difficulty in nasal breathing, tooth pain, and unilateral nosebleeds appear without signs of changes in the nasal mucosa. Subsequently, the tumor grows into the bone walls, resulting in bone deformation and exophthalmos. Gum reaction, bulging or asymmetry of the hard palate are noted.
In the early stages of development, tumors do not have pathognomonic symptoms.
Children are treated for sinusitis with extensive use of physical therapy, which promotes rapid tumor progression. When attempting alenotomy, nasal polypotomy, puncture of the maxillary sinus and suction of nasal secretions, massive bleeding with progressive anemia often occurs.
For the purpose of early diagnosis in case of unilateral progressive difficulty in nasal breathing and spontaneous nosebleeds, a thorough comprehensive examination is necessary.
Features of radiography for sinusitis
The main way to confirm sinusitis today is still radiography. The procedure takes very little time and is available in most clinics in Russia.
On an x-ray of the paranasal sinuses with sinusitis, darkening in the area of the maxillary sinuses is clearly visible, indicating that there is an inflammatory process and there is excess fluid. Depending on the severity of the disease, the darkening can be local (small), subtotal and total.
Small darkening indicates that the disease began not long ago, the painful manifestations are not very pronounced, and drug treatment will be most effective.
Subtotal blackout
Subtotal darkening of the maxillary sinuses may indicate a severe inflammatory process. This suggests that the disease is in an advanced state. In such cases, in addition to antibacterial therapy, procedures may be prescribed to remove fluid from the inflamed sinus cavity.
Sometimes the inflammation spreads to other paranasal sinuses. Sinusitis can turn into frontal sinusitis or sinusitis. In such cases, the pathological process affects, respectively, the frontal sinuses or the ethmoid labyrinth.
Total blackout
Detection of total darkening on an x-ray is an alarming sign. However, modern medicine copes with such advanced cases. The most important thing is that treatment is started immediately.
If the sinuses are filled with pus and inflammatory processes are in full swing, then doctors prescribe fairly high doses of antibiotics to prevent the development of serious complications. Additionally, a puncture of the maxillary sinuses can be performed to remove accumulated exudate.
Symptoms during the formation of mycetoma
In the early stages, a patient with mycetoma feels absolutely nothing, because there are no symptoms of the disease yet.
And as the fungal growth increases in size, it will become more difficult for the patient to breathe due to nasal congestion on one side, while the nose will be clean, without discharge. But sometimes the discharge can be in the form of crumbly masses of a gray-dirty color. In addition to the symptoms listed earlier, the patient may experience dizziness, headaches, when the mycetoma grows strongly, it occupies the entire volume of the maxillary sinus, creating excess pressure, including in the orbital area. And, of course, with a large growth of mycetoma of the maxillary sinus, sinusitis is possible. The patient may have pain in the upper teeth in the lateral part from the side of the mycetoma. And, as I said earlier - difficulty breathing, the patient switches to mouth breathing as a result of acquired chronic sinusitis.
How extensive can a mycetoma be?
Molds can grow until the maxillary sinus is completely filled. And when the mold ball occupies the entire maxillary sinus (it usually takes 5-7 years to grow), the diameter of the ball reaches an average of 3-5 centimeters.
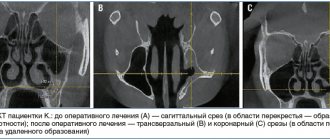
For example, here is a photo of a mycetoma of the maxillary sinus, when the growth of fungi has almost completely “captured” it. The cause of the formation of mycetoma in this case was a part of the root filling of the tooth that was removed into the maxillary sinus:
We describe in detail how the root filling got into the maxillary sinus in this clinical case.
Possible complications of advanced sinusitis
Sinusitis in itself is not a dangerous disease. However, inflammation in tissues so close to the brain can have serious consequences, especially if not treated adequately and promptly.
Meningitis and meningoencephalitis
Meningitis is a dangerous disease characterized by an inflammatory process in the membranes of the brain. This disease can lead to disability and even death.
Meningoencephalitis is an even more serious disease. Inflammation in meningoencephalitis covers both the membranes and the substance of the brain.
The symptoms of these diseases are similar:
- headache;
- nausea;
- vomit;
- chills;
- elevated body temperature.
These diseases are very insidious. If there are prerequisites for their occurrence, they can develop in an acute form within just a few hours.
Both diseases are extremely dangerous and have a poor prognosis. High probability of death.
Chronic sinusitis
If acute sinusitis is treated incorrectly or not treated at all, the disease may become chronic. Chronic sinusitis is difficult to treat, and it is impossible to guarantee a positive treatment outcome.
Periodically, with a decrease in immunity, chronic sinusitis will worsen, causing a lot of inconvenience. In addition, a chronic inflammatory process in the maxillary sinuses is fraught with much more serious problems, including:
- chronic rhinitis;
- inflammation of bone tissue;
- inflammation of brain tissue.
You should take care of your health. Then the occurrence of a disease such as chronic sinusitis is unlikely.
Treatment of advanced sinusitis
After developing radiographs, one can judge the severity of the inflammatory process occurring in the maxillary sinuses. In case of total blackout, the doctor may prescribe a shock course of antibiotics and antihistamines to suppress inflammatory processes and reduce the severity of some symptoms.
In the most severe cases, surgical intervention may be indicated - puncture of the sinuses. This procedure has been known for a long time and is widely used in many countries around the world. Using a special syringe, excess fluid and pus are pumped out of the maxillary sinus. Then the sinus is filled with a special solution containing antiseptic drugs. This is done to reduce inflammation of the mucous membrane. Then the solution is pumped out of the sinuses. That's it, the procedure is completed.
This type of surgery is not dangerous, but it can speed up recovery and reduce the appearance of major symptoms, such as headaches.
For more effective treatment of sinusitis, the pus obtained after puncture can be sent for culture to identify the pathogen and determine which antibacterial drugs it is most sensitive to. Along with antibiotics, antihistamines are often prescribed to help reduce swelling, nasal congestion and other manifestations of the disease.
Some traditional medicines can be used to treat sinusitis. Such remedies should not replace the primary treatment prescribed by a doctor. They can only complement it. Moreover, before using any means, you should consult your doctor.
Using exclusively traditional medicine to treat sinusitis can lead to disastrous results. Untreated sinusitis will become chronic and will periodically trouble the patient throughout his life.
Causes and course of the disease
Latent (hidden) or sluggish sinusitis of a chronic nature is difficult to diagnose and treat.
Such sinusitis manifests itself as intracranial complications and is caused by atypical bacterial flora, which can only be identified by special bacteriological studies. Due to its hidden course, latent sinusitis is difficult to detect. Sluggish inflammation in the paranasal sinuses does not have symptoms (rhinological) from the nasal cavity and does not involve the lateral (outer) wall of the nasal cavity in the process, and therefore does not cause disturbances in the basic functions in the nasal cavity.
Latent sphenoiditis (inflammation of the mucous membrane of the sphenoid sinus) and latent ethmoiditis (inflammation of the mucous membrane of the ethmoidal labyrinth cells) appear simultaneously with complications associated with signs of optochiasmal arachnoiditis (disease of the membranes surrounding the optic nerves located in the cranial cavity behind the eyeballs), abducens nerve paresis , optic neuritis. The main complaint of ENT patients is a very persistent causeless headache, most often localized in the occipital region.
With such complaints, patients often seek help not from an ENT doctor, but from a neurologist or ophthalmologist, who prescribe therapy limited to the disease they have identified, within their specialty. Only if the treatment is ineffective and the disease progresses, the patient is referred for consultation to an otolaryngologist.
Latent sphenoiditis and ethmoiditis are not detected during computed tomography (CT) and magnetic resonance imaging (MRI). Only minor local signs are detected in the form of thickening of the mucous membrane of one or another sinus, but the airiness of the entire sinus is preserved.
The harm of self-medication
The most obvious harm of self-medication is the lack of positive results. People often take medications until they feel better. However, this approach is wrong. Antibacterial drugs should be taken only as prescribed by a doctor. Strictly in the volumes and within the time frame that he announced at the reception. Otherwise, the symptoms will go away, but the source of infection will remain. Inflammation in the maxillary sinus will become chronic.
Or, if the drugs were chosen incorrectly, there may be no improvement at all. The disease will become advanced, the pain due to overcrowded sinuses will become unbearable, and inflammation will have a chance to spread to the organs and tissues closest to the sinuses, causing all sorts of complications.
Another risk of self-medication is the medications that must be taken for sinusitis. If the dosage is incorrect, taken too often, or if there are problems with internal organs, antibacterial drugs can do more harm than good. Cases of drug-induced liver damage from uncontrolled use of antibiotics are not so rare. What can we say about gastrointestinal tract disorders, dysbacteriosis, and so on.