Treatment of cysts with calcium preparations in dentistry
Given the constant and continuous development, modern dentistry successfully combats most diseases of the teeth, gums and the oral cavity itself. One of these problems is a dental cyst.
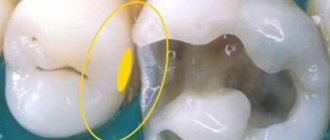
Tooth cyst
is a disease expressed in the formation of an inflammatory capsule with dense walls, inside of which there is often a mass consisting of bacteria and dead cells. This neoplasm appears in the gums around the root of the tooth, and in the absence of timely and targeted treatment, it can cause undesirable consequences. Over time, the size of the cyst increases, gradually destroying the surrounding bone tissue.
The occurrence of a dental cyst is usually associated with an infection; less often, the cause of the disease can be an injury that can be obtained in a completely trivial way - for example, cracking nuts with your teeth.
To determine the presence of a dental cyst, an X-ray examination of the affected area of the jaw is performed. Most often, the patient does not even suspect the presence and development of a cyst, since it passes painlessly
without causing any discomfort. Only during exacerbation does profuse tissue inflammation occur, accompanied by purulent formations and “flux.”
For successful treatment of the disease, its timely diagnosis is very important. Modern dentistry uses two methods to treat inflammation: surgical and therapeutic.
For therapeutic treatment of cysts, the inflamed tooth is drilled and the root canal is disinfected using a special solution. However, the result of these manipulations is not always successful, therefore, six months after the treatment, a re-examination with X-rays will be required to exclude re-inflammation.
Treatment of cysts with a more modern therapeutic method used in dentistry is the use of depophoresis
.
During the treatment, calcium is used, or rather copper-calcium hydroxide, which is injected into the canal of the diseased tooth. At the same time, the tooth is exposed to a weak electric current - for better penetration of the suspension into the cyst and its removal. After three sessions of depophoresis, the tooth is filled. Also, in the treatment of dental cysts, preparations based on calcium and iodine are used ( Metapex
,
Calasept,
etc.).
When using the surgical method in dentistry, the cyst is removed along with the damaged part of the tooth root (cystectomy), or the entire root and part of the tooth above it are removed (hemisection), subsequently placing a crown on it. The site of the resulting defect in the bone tissue is filled with bone material.
Complications in endodontics
Author: Zuhair Alkhatib
Translation: Roman Ragozin
Calcium hydroxide
Calcium hydroxide [Ca(OH)2] has been used in dentistry for many years. In root canal treatment, its use as a temporary attachment has a positive effect on the healing of periapical inflammation. Due to this property, calcium hydroxide has become a widely used preparation for temporary intracanal placement. Calcium hydroxide is an effective antibacterial agent, mainly due to the high acidity of the environment (pH) and its destructive effect on bacterial cells and protein structures. It has been established that when calcium hydroxide is applied in cases of extensive periapical lesions, conditions favorable for healing are created and osteogenesis is stimulated. Calcium hydroxide is a shapeless, fine, granular powder with strong base properties and a density of 2.1. Slightly soluble in water and insoluble in alcohol. Due to the lack of radiopacity of calcium hydroxide, it is difficult to determine its presence on radiographs. This is the main reason for adding various radiopaque materials (barium sulfate [BaSO4], bismuth, and other compounds containing iodine and bromine) to the paste, thereby allowing the detection of lateral and accessory canals, resorptive defects, fractures and other structures. At the same time, in cases of uncovered root apex, it is recommended to use calcium hydroxide without radiopaque impurities, since the degree of leaching of calcium hydroxide is assessed by its relative radiodensity in the canal in subsequent visits.
Etiological factors
During root canal treatment, temporary material may inadvertently be removed beyond the root apex, which may result in complications such as hypoesthesia and paresthesia of the inferior alveolar nerve. As a rule, such complications are observed when the material is removed under high pressure, or when there is a neurotoxic effect on the neurovascular bundle. The released agent causes changes in the surrounding bone and also affects the inferior alveolar nerve. Extrusion is also observed with a wide apical foramen in immature permanent teeth. Complications can arise when a syringe with calcium hydroxide is immersed to a depth sufficient to create pressure above arterial pressure, causing the paste to penetrate the bloodstream. It should be noted that calcium hydroxide particles are small enough to penetrate the capillaries, which can cause mechanical obstruction, or induce crystallization in the bloodstream, blocking circulation. Conclusion
Depophoresis
Depophoresis is the newest method of treating teeth with difficult to pass root canals. Increases the reliability of canal filling and the effectiveness of treatment of periodontitis, cystogranulomas, teeth with fragments of instruments.
This method, which belongs to the group of “high technologies” in dentistry, is widely used in our clinics for endodontic treatment of root canals.
The main goal of endodontic treatment is to ensure the permanent sterility of the remaining tooth in the jaw. This cannot be achieved using traditional approaches in endodontics, since disinfectants are not able to reach the entire complex system of root microcanals through natural diffusion from the main root canal. There are also teeth for which access to the root canals is very difficult due to anatomical features (for example, the bend of the root canal at an angle of more than 60 degrees). Therefore, classical endodontic treatment does not guarantee complete success due to the unpredictability of microbiological processes in the complex root canal system. The consequences of classical endodontic treatment strongly depend on the degree of infection of the root dentin and the immunological status of the patient.
In recent years, a fundamentally different method of endodontic treatment of a complex root canal system has been proposed - copper-calcium hydroxide depophoresis . During treatment under the influence of an electric field, from the area of high content (depot) of the copper-calcium hydroxide suspension (in the main root canal), forced diffusion of hydroxide ions (having a strong bactericidal effect) and hydroxycuprate ions occurs into the entire canal system, including side microchannels, microholes . This leads to complex chemical and biochemical reactions and processes involving biological tissues and microorganisms. After 2-3 sessions of depophoresis (5-7 minutes for each canal), the canal is filled with a special material - atatamyte.
As a result, the tooth root becomes sterile, completely protected from the penetration of microorganisms and can serve as a support for further restoration and prosthetics. The method is also used in the treatment of chronic periodontitis. According to numerous data, the depophoresis method leads to positive results in 92% of cases and is therefore often the only alternative to tooth extraction.
A shining Hollywood smile from leading specialists in aesthetic dentistry. Make an appointment!
Reasons and purposes of application
The scope of application of the substance in dentistry is quite narrow. The direct purpose of calcium hydroxide in endodontics is the treatment and filling of root canals. The basis for use is the diagnosis of pathological processes in the area of the pulp and hard tissues of the tooth.
When the material remains in the channel cavity for more than two weeks, cementation of the powder occurs, which leads to complete sealing of the channel. In certain cases, this effect is used purposefully by dentists if other treatment methods are unacceptable.
It should be clarified that preparations with calcium hydroxide can be used in the surgical treatment of damage to the jaw structure, as well as in bone grafting.
Calcium hydroxide is also used in the dental field for intra-root therapeutic effects. Calcium-based materials are used if the following diseases are diagnosed:
Treatment with calcium hydroxyl cements is relevant for periodontitis
- pulpitis;
- inflammatory processes in bone tissue;
- neoplasms (granuloma, cyst);
- periodontitis;
- periodontitis;
- deep caries.
Calcium hydroxide can also be used after surgery to remove tumors or nerves. Used to fill canals before installing permanent fillings or implants.
Unlike many other medications used in dentistry, calcium hydroxide does not have side effects and can be contraindicated only if you are intolerant to the chemical itself.
Basic properties and biological effects of preparations based on calcium hydroxide
Authors:
Tatyana Belyaeva, Alexey Bolyachin, Department of Therapeutic Dentistry and Endodontics, Moscow State Medical Dental University (Moscow, Russian Federation).
For many years, calcium hydroxide has been actively used in endodontics to solve a wide range of treatment problems. Some clinicians attribute almost unique properties to calcium hydroxide, while others, on the contrary, consider its use unfounded. The purpose of this article was to summarize the data available in the literature regarding the chemical properties of calcium hydroxide and the biological effects of drugs based on it.
The first mention of calcium hydroxide in specialized dental literature dates back to 1838 and belongs to Nygren, who used this drug to treat “dental fistula” (fistula dentalis). Somewhat later, Codman first used calcium hydroxide for direct pulp capping (Codman, 1851), but calcium hydroxide became truly widespread after Hermann introduced the first patented hydroxide-based preparation to the dental market in 1920 calcium - calxyl (Caixil) (calcium hydroxide suspended in Ringer's solution) (Herman, 1920). From that moment on, its active clinical and laboratory research began both in Europe and America.
Until recently, calcium hydroxide was considered the most effective drug capable of stimulating the deposition of replacement dentin and the repair of pulp and periodontal tissue. These properties determine such a wide range of indications for the use of calcium hydroxide in endodontics. Although it should be noted that not so long ago a new drug appeared on the world market - mineral trioxide aggregate (MTA). Possessing unique biological properties, MTA has become an alternative to the use of calcium hydroxide in a number of clinical situations. Yet in modern endodontics, calcium hydroxide continues to receive significant attention.
Currently, the main indications for the use of calcium hydroxide in endodontics are, according to Heithersay, 1975; Fava & Saunders, 1999: • indirect and direct pulp capping; • pulpotomy; • temporary filling of root canals; • perforation of the root and furcation area; • apexification; • apexogenesis; • internal root resorption with and without perforation of the lateral root wall; • external inflammatory resorption; • external cervical resorption associated with intracanal bleaching; • post-traumatic complications (tooth dislocation, replantation); • horizontal root fracture.
Yet, most often in everyday endodontic practice, calcium hydroxide is used for temporary filling of root canals between visits in teeth with infected necrotic pulp and symptoms of apical periodontitis.
The objectives of temporary filling in this case are: 1) destruction of bacteria remaining in the lumen of the canal and adjacent dentin after mechanical treatment and irrigation; 2) preventing bacterial growth between visits; 3) creation of a chemical and mechanical barrier that prevents reinfection of the root canal and the penetration of nutrients from outside for bacteria remaining in the canal.
Chemical properties of calcium hydroxide. Calcium hydroxide is a white powder, odorless, insoluble in ethyl alcohol, but has very low solubility in water, which decreases with increasing temperature. The finished drug is a suspension, and when introduced into the canal, only 0.17% of the drug dissolves. Its low solubility (only 1.2 g/l) provides good clinical characteristics, since when in contact with vital tissues, calcium hydroxide requires a long time to dissolve in the tissue fluid. According to the chemical classification, calcium hydroxide belongs to the strong bases. Its pH is 12.5-12.8. The main biological effects of calcium hydroxide are due to its dissociation in an aqueous environment into Ca2+ and OH ions.
Biological effects of calcium hydroxide. 1. The mechanism of the antimicrobial action of calcium hydroxide. Hydroxidiones released from calcium hydroxide during its dissociation, at a sufficiently high concentration and direct contact with bacterial cells, lead to the destruction of the bacterial cell membrane, denaturation of structural proteins and enzymes, and damage to bacterial DNA (Siqueira et al., 1999). The destructive action of calcium hydroxide is based on hydrolysis reactions. 0H ions initiate peroxidation of phospholipids in the bacterial cell membrane. They accept hydrogen atoms from unsaturated fatty acids that make up the lipid membrane of bacteria. As a result, free lipid radicals are formed, which, when reacting with oxygen, lead to the formation of lipid peroxide radicals. These secondary free radicals in turn react with further unsaturated acids of membrane lipids, triggering a cascade of autocatalytic chain reactions that ultimately lead to widespread damage to the bacterial cell membrane (Rubin & Farber, 1990). As a result, such vital functions of the bacterial wall as selective transport of molecules and ions through the membrane, growth, cell division, etc. are disrupted. (Burnet & Schuster, 1982). The transport of nutrients across the membrane at elevated pH levels can also be disrupted as a result of a change in the electrical charge of the molecules and, as a result, a decrease in their ability to pass through the layer of membrane phospholipids.
In addition, OH ions can penetrate into the bacterial cell and react with its basic structures. Thus, hydroxylion causes splitting of the chains of the DNA molecule, which leads to the cessation of bacterial DNA replication and inhibits cell activity. In addition, free radicals can directly cause lethal mutations in bacterial DNA.
Another important mechanism of the antibacterial action of calcium hydroxide is the denaturation of bacterial proteins and enzymes. The metabolism of a bacterial cell is mainly determined by the activity of its enzyme systems, which, in turn, require a certain pH level to function. Most enzymes exhibit their maximum activity at neutral pH values. Alkalinization of the medium leads to the destruction of ionic bonds that support the tertiary structure of the protein molecule, which leads to the “unraveling” of the enzyme molecule and, as a consequence, its loss of biological activity. Structural proteins can also be exposed to hydroxyl ions.
In addition, in addition to the direct chemical inactivation of microorganisms, calcium hydroxide in the root canal also serves as a mechanical barrier that prevents the penetration of new microorganisms and substrates for the vital activity of surviving bacteria into the canal from the oral cavity , and also limits their living space and ability to grow and reproduce (Dalen and Moller (Dahlen & Mopel, 1992; Siqueira et al. 1998).
The mechanisms described above determine the high nonspecific antimicrobial activity of calcium hydroxide. Theoretically, when in direct contact with a bacterial cell, calcium hydroxide is capable of killing both gram-positive and gram-negative facultative and obligate bacteria, as confirmed by in vitro laboratory studies by Siqueira & de Uzeda, 1998. Unfortunately, providing direct contact with calcium hydroxide It is not always possible to deal with a bacterial cell inside the root canal.
In addition, infection of the dentinal tubules is common as a secondary infection in cases associated with repeated endodontic treatment of teeth (Oguntebi, 1994; Love & Jenkinson, 2002). Moreover, the main microorganisms that populate the dentinal tubules are gram-positive facultative strains, in particular Enterococcus faecalis (Haapasalo & Orstavik), 987; Molander et al., 1998; Sundqvist et al., 1998; Noda et al., 2000; Nikuline et al., 2000, 2001); Hancock (Trope et al., 2001); Candida Albicans (Sen et al., 1995; Valtimo. Temporary filling of canals with calcium hydroxide paste. Calcium hydroxide acts as a mechanical barrier, preventing the penetration and proliferation of bacteria inside the root canal between visits (Waltimo et al., 1997, 2000); Pikuline et al., 2001), known for their resistance to the main antiseptics used in endodontics (Orstavik and Haapasalo, 1990; Siqueira et al., 1997).
When using calcium hydroxide as a temporary filling of canals, it should be taken into account that the maximum pH level is reached quite quickly in the lumen of the main canal, while in the layer of adjacent dentin this process is slower and reaches lower values. With distance from the canal lumen, the maximum pH level drops to an average of 9-9.5 (Nerwich et al., 1993). At the same time, it is known that for most microorganisms the optimal pH level for life lies in the range from 5 to 9. But some bacteria (for example, Enterococci) can survive at higher pH values. Thus, M. Evans and co-authors showed that E. faecalis is able to survive even at pH values equal to 11, and when the pH level increases from 11.1 to 11.5, its survival rate decreases 40 times - from 0 .4% to 0.01% respectively (2002). Nakajo et al. (2006) also obtained similar results.
Despite the fact that the OH ion has a very small size, which allows it to penetrate into the dentinal tubules to their entire depth down to the root cementum layer (Foster et al., 1993), the low rate of disinfection of dentinal tubules with hydroxide calcium is due to several reasons. The first factor is the insufficient concentration of hydroxyl ions in the adjacent dentin due to the poor solubility and diffusivity of calcium hydroxide. And the shorter the time of its exposure inside the channel, the lower this concentration. In addition, the activity of calcium hydroxide is inhibited by the action of the root dentin itself, as well as by albumin contained in tissue fluid, which can leak into the root canal through the apical foramen from periodontal tissues (Haapasalo et al., 2000, 2007; Portenier et al. , 2001). Root dentin has a certain buffering capacity due to the presence in it, namely in the hydration layer, of hydrogen ion donors - phosphate and bicarbonate buffer systems, the work of which is aimed at maintaining a constant pH (Wang & Hume, 1988; Nerwich ) et al., 1993). In addition, the organic portion of dentin also appears to have little buffering capacity (Camps & Pashley 2000; Portenier et al. 2001). Another reason that reduces the effectiveness of calcium hydroxide is the presence of organic debris inside the root canal that was not removed during chemomechanical treatment, as well as the smear layer resulting from canal preparation and closing the entrance to the dentinal tubules. In addition, the bacterial biofilm, always present in the infected root canal, significantly reduces the effectiveness of calcium hydroxide (Chavez de Paz, 2007).
In addition to the above factors, some bacteria have their own adaptive mechanisms, which also make calcium hydroxide ineffective in combating them. For example, Enterococcus faecalis, as noted above, is able to colonize dentinal tubules due to pronounced adhesion to non-mineralized dentin collagen (Love, 2001). The ability of E. faecalis to survive at high pH values is determined by the structure of its outer membrane, which contains a proton pump that forces cations from the outside through the membrane into the cell against an electrochemical gradient, thereby maintaining the intracellular pH balance necessary for the life of the bacterial cell (Ivens et al. , 2002). In addition, in previously filled canals with a progressive focus of infection, E. faecalis is most often in the phase of its life cycle, called the “starvation phase,” when its resistance to disinfectant agents is greatest (Portenier et al., 2005).
The low effectiveness of calcium hydroxide in terms of sterilization of dentinal tubules has been demonstrated in a number of studies. For example, Haapasalo and Orstavik proposed a now classic model for the study of disinfectants in vitro under natural conditions (1987). In the same work, they demonstrated the ineffectiveness of a 10-day exposure to calcium hydroxide paste against infection of dentinal tubules using the example of Enterococcus faecalis. Similar results were obtained by other researchers (Safavi et al., 1990; Siqueira and de Useda, 1996). The low fungicidal activity of calcium hydroxide against fungi, in particular the genus Candida, was demonstrated in the works of an authoritative scientific group from Scandinavia.
Application for temporary filling
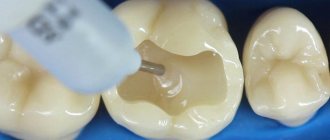
The main area of application of preparations based on hydroxide and pure calcium hydroxide powder is the tooth filling procedure. Materials with a chemical are used in the form of temporary and permanent fillings.
Since drugs change the microflora in the area of their application, and can also harden, their use must be carried out according to a certain scheme.
During the procedure for installing a temporary filling, a specialist must perform the following actions:
- measure the length of the processed channel;
- mix calcium powder with saline solution (use a ready-made preparation);
- dip the desired channel filler into the material;
- insert the instrument into the canal, 1 mm short of its end;
- start the rotation of the channel filler to process the desired areas.
Only after the process has been repeated three to four times can the dentist seal the tooth with a small layer of cement.
To increase the effectiveness of treatment, you should adhere to the following rules:
- the root canal should be opened as much as possible;
- after dilution, the finished material should have a creamy consistency;
- the channels must first be cleaned and treated;
- the residence time of the material in the tooth cavity is not less than 2, but not more than 4 weeks.
How to properly mix cement based on calcium hydroxide:
Mechanism of action
As a result of applying dissolved powder to the root canals, a reaction begins to occur between the substance, tissue cells and the microflora of the inside of the tooth. The hydroxide diffuses through the dentin channels and penetrates deep into the pulp.
The mechanism of action of calcium hydroxide is designed to provide an antimicrobial, anesthetic and therapeutic effect. Due to the long-term presence of the drug in the tooth cavity, the treated area is completely disinfected and loses sensitivity, which allows further treatment and the installation of fillings or therapeutic pads without any risks.
In addition to the main antiseptic effect, some preparations based on calcium hydroxide are capable of destroying certain types of organic tissue, which makes it possible to “kill” the nerve fibers in the canals (devitalize the pulp), thus achieving the effect of “insensitivity” of the tooth.