Classification of adhesives in dentistry
Interesting fact: Victoria Beckham once had to spend 40 thousand dollars to restore her attractive smile.
Adhesive systems in dentistry were created in the late 50s of the last century. They bonded well to hard surfaces, but with dentin consisting of 30-50% water, the bond strength remained low. Dental scientists have constantly improved materials, which has led to the creation of a modern adhesive consisting of an etchant component, a solvent, a primer and a bond.
There are adhesive systems aimed at interacting only with enamel, as well as additionally with dental dentin. They differ in chemical composition and method of application. The first type is practically not used in the presence of caries and open dentin.
Adhesives in dentistry are also divided according to the method of hardening into the following types:
- light-curing (hardening occurs using a special lamp);
- self-curing (there is no need to use additional equipment);
- double acting systems.
Sometimes patients confuse composites with adhesives. The first ones belong to restoration materials with high aesthetic indicators. They are used to restore teeth.
Types of adhesives
Enamel adhesive is a hydrophobic solution that, due to micromechanical adhesion, ensures adhesion of the composite surface to the surface of the enamel or primer (Synonym: bond).
Dentin adhesive is a hydrophilic solution that, due to micro- and nanoretention, ensures adhesion of the composite to the dentin surface (Synonym: primer).
Enamel-dentin adhesive is a solution capable of firmly attaching to both enamel and dentin (Synonyms: adhesive or bonding systems, adhesion activators).
Objectives of adhesive systems
Ensure tight, gapless contact of the filling material with the hard tissues of the tooth
Prevent the penetration of microorganisms and dyes along the filling-tooth border in the direction of the pulp chamber
Provide a strong connection to hard tissue, thereby eliminating the need for additional retention points and unnecessary removal of hard tissue
Generations of adhesives
Interesting fact: almost every filling, composite, and polymer has its own adhesives that are most suitable for this particular option.
Each adhesive created belongs to a separate generation. The 4th was revolutionary, as close as possible to modern systems. This is what was used most often. Everything that existed before it is not used in modern dentistry, so we will not talk about them. Let's take a closer look at the existing options:
- 4th generation adhesives. Provide high adhesion, include 3 components: bond, primer and conditioner. Disadvantages include the complexity of the work.
- 5th generation. The materials included in the composition combine the properties of an adhesive and a primer, so the work is carried out in a fewer number of stages. They have high levels of adhesion to dentin and enamel.
- 6th generation. During application, self-etching is carried out to a shallow depth, so “plugs” in the channels are not removed. A huge advantage is the absence of postoperative sensitivity.
- 7th generation adhesives. All the necessary components are contained in one bottle, which significantly reduces the time spent on work.
Modern dentistry has made great progress, so by visiting a doctor, you can get high-quality results that will last for many years.
The iOrtho clinic network provides high-quality services for correcting malocclusion with Invisalign aligners, sign up for a consultation now!
Adhesive system: a choice of generations
Despite the fact that currently there are a large number of adhesive systems, the problem of ensuring a reliable and long-term connection of the composite to the tooth surface has not yet been completely solved [6]. In this regard, various companies, in parallel with the creation of composite materials, produce new and improve existing adhesives.
I would like to draw attention to the fact that the choice of a suitable adhesive can be a decisive factor in increasing the service life of the completed restoration. Also, for reliable retention of the filling, prevention of marginal permeability and prevention of secondary caries, the quality and correct use of the adhesive system before filling the cavity with filling material is of great importance [2]. The abundance of adhesive systems existing on the dental market puts the doctor in a difficult position: so which system to choose for the job? Having summarized the literature data, as well as the results of their own observations, the authors of the article want to share the clinical and technological features of the use of different generations of adhesive systems.
Today there are 7 generations of adhesive systems.
At clinical appointments, adhesives are used starting from the 4th generation. Our foreign colleagues still mainly use 4th generation systems in their work, which ensure the highest adhesion of the composite to enamel and dentin.
They contain three components: conditioner, primer and bonding agent (adhesive).
5th generation adhesive systems include components that combine the properties of a primer and an adhesive; they are used in two stages: etching and application of a one-component adhesive. Let us recall that the action of adhesive systems of the 4th and 5th generations is based on the dissolution and complete removal of the “smear” layer [3].
Therefore, the use of these systems involves the technique of total conditioning of hard dental tissues. In some publications, the recommended duration for etching enamel with acid is 60 s. However, experimental studies using electron microscopy (Barkmeier WW et al., 1986; Swift EJ et al., 1995) showed that etching for 15 s leads to the same enamel porosity as with exposure for 60 s. Moreover, prolonged exposure leads to the destruction of enamel prisms.
Residual acids can prevent the adhesive from binding to the hard tissues of the tooth, so the acid must be thoroughly washed off the tooth surface. Theoretically, all doctors know that it is necessary to rinse the cavity for as long as the conditioning was carried out. However, in practice this principle is not observed. Meanwhile, only complete rinsing of the cavity with a water-air aerosol under pressure for 15 seconds. ensures complete removal of acid and insoluble precipitates formed during the etching process. In addition, simply applying acid to the enamel (so-called static etching) is not enough for high-quality etching. This type of etching ensures good etching only of the internal areas consisting of enamel prisms. In this case, the etching of aprismatic areas occurs unevenly. As a result, islands of unetched enamel remain on the surface, with which the adhesive does not interact. This leads to the formation of microspaces, the appearance of a white line, and marginal staining of the restoration. This problem is most relevant in aesthetic fillings and is critical when etching unprepared enamel, since in this situation such islands make up the majority of the bonding surface. Based on the above, preference should be given to dynamic etching, which involves constantly rubbing the etching gel into the enamel surface using a brush or applicator. With this technique, regardless of the initial structure of the enamel, a uniform micro-roughness of its surface is achieved [4].
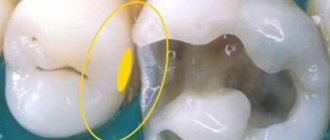
When dentin is conditioned (no more than 15-20 seconds), its surface layer is demineralized, the “smear” layer and the layer of “plugs” that cover the mouths of the dentinal tubules are removed [1, 6] (Fig. 1).
Rice. 1. Conditioning of enamel and dentin with Vokotsid gel.
At dental appointments, we use the 4th generation adhesive system “Solobond Plus” (Solobond Plus, VOCO). In our opinion, the huge advantage of this system over analogues is the formation of a strong bond between the composite and tooth tissues and the effect of immediate adhesion (the composite is glued to the bond, and not to the instrument). Another advantage of such a system is that the primer, which is an easily spreadable solution that well wets the etched surface, performs only one function, namely, penetration into the spatial structure of exposed collagen fibers and the formation of a transition layer, the structure of which is stabilized upon subsequent application relative to more viscous adhesive (Fig. 2-4).
Rice. 2. Application of primer. Rice. 3. Drying the primer with a stream of air. Rice. 4. Application of adhesive and its photopolymerization.
This significantly increases the likelihood that the adhesive will reach the deepest areas of demineralized dentin layers and, therefore, higher adhesive bond strength will be achieved (Haller B., Blunck U., 2004). The 4th generation adhesive system can be used in a variety of clinical applications situations: when performing direct restoration of any defects using composite materials; for treating hard dental tissues before fixing crowns, bridges, inlays, for the prevention of increased sensitivity of teeth. In addition, “Solobond Plus” is preferable to use when working with dual-curing materials (light + chemical) for fixing fiberglass pins.
The most famous 5th generation adhesive is Solobond M (Solobond M, VOCO). In our opinion, the unique advantage of Solobond M is its one-time application to the surface of tooth tissue and rapid drying under the influence of a stream of air without the formation of “waves”.
This means a reduction in work steps and, accordingly, saving time and material. The one-component system minimizes mixing errors and simplifies storage. In addition, Solobond M is available in practical unidoses - tiny blisters made of aluminum foil containing a drop of adhesive sufficient to cover two or three small cavities. As experience in clinical use shows, Solobond M provides reliable adhesion and marginal sealing of the filling, minimizing the risk of developing postoperative sensitivity. It can be recommended as the main adhesive system in the daily work of a dentist (Fig. 5-7).
Rice. 5. Initial clinical situation: tooth 47 before treatment. Rice. 6. Stage of application of the Solobond M adhesive system. Rice. 7. Tooth 47 after restoration.
I would like to draw attention to the recommendations that are important to follow when working with 4th and 5th generation adhesive systems. First, the adhesive must be applied using light, gentle “appliqué” movements.
At the same time, it is strongly recommended not to “rub” it forcefully into the surface of the enamel and dentin, since this may cause damage to the “etching pattern” and collagen fibers in the dentinal tubules. Secondly, after applying the adhesive, it is necessary to wait a certain period of time (about 10-15 seconds) before removing excess solvent so that the adhesive penetrates to the same depth as the etching gel. Otherwise, postoperative sensitivity will occur. After this, using a stream of compressed air, it is necessary to carefully remove excess solvent until there are no “waves”. If the solvent is not completely removed, incomplete polymerization will occur, also leading to the development of postoperative sensitivity. Thirdly, after conditioning and washing the hard tissues of the tooth, the doctor most often dries the dentin either with a stream of air or with cotton balls, which he rolls himself. However, in this case, bacterial contamination of the surface of the cotton ball occurs, since the doctor does not change gloves beforehand. Therefore, we recommend carrying out the stage of drying the dentin using Pele Tim foam sponges, which have different sizes and absorb a certain amount of moisture, while leaving the dentin surface moist enough to create a full-fledged hybrid layer (Fig. 8).
Rice. 8. Drying the dentin using a Pele Tim foam sponge.
Recently, self-etching adhesive systems of the 6th and 7th generations have become more frequently used at dental appointments. The advantage of these systems is that the dentin is etched shallowly and “plugs” in the canals are not removed. It is obvious that their use in most cases is not accompanied by postoperative sensitivity. Despite the fact that the hybrid layer is thin, the strength of the adhesive-dentin connection is very high [5–7]. Of the 6th generation adhesive systems, we use Futurabond NR (VOCO). Long-term clinical trial data has demonstrated Futurabond HP's extremely high bond strength levels, which are comparable to those obtained using the total etch technique. The superstable emulsion of nanoparticles contained in Futurabond HP, obtained using the patented Sol-gel technology, allows the material to be applied in only one layer and photopolymerizes for 10 seconds, which ensures high adhesion strength and ease of use. It saves time, which is especially valuable in gerontological and pediatric practice. Futurabond NR releases fluorides, which prevent the development of “secondary” caries. Self-etching adhesives are ideal for restoring cervical defects in hard dental tissues. The fact is that over time, hypermineralization (dentinal sclerosis) occurs in the area of the bottom of the defect, leading to the closure of the lumen of the dentinal tubules with mineral crystals, making it difficult for adhesive systems to access. The use of self-etching systems makes it possible to transform the smear layer and, in combination with preliminary etching of the bevel boundaries with orthophosphoric acid, simultaneously decalcify the surface layer in the area of the defect (Fig. 9).
Rice. 9. Tooth 21 after restoration using Futurabond HP and Amaris Gingiva.
Of particular interest in recent years is Futurabond DC, a self-etching dual-cure adhesive. We recommend using this system in those clinical situations where the light from the photopolymerizer is not enough to fully illuminate the adhesive, for example, in hard-to-reach areas: when fixing fiberglass pins, veneers, inlays, etc. If Futurabond DC is not completely illuminated by the lamp, it will within 3 minutes it polymerizes independently chemically (Fig. 10).
Rice. 10. Application of Futurabond DC before fixing the fiberglass pin.
Recently, new 7th generation adhesives have appeared on the dental market - Futurabond M+ and Futurabond U. The advantage of Futurabond M+ is that this universal adhesive can be used for both direct and indirect restorations. It has reliable adhesion to a variety of materials without additional primer, including metal, zirconium and aluminum oxide, and silicate ceramics. "Futurabond U" is a universal dual-curing adhesive that is compatible with all photopolymer, self-curing composites, and dual-curing materials. But its main advantage is its tolerance to moisture and the absence of the need for storage in the refrigerator. In addition, studies by Toru Nikaido et al. (2007, 2009) confirmed that the functional monomers of self-etching systems, which have a chemical connection with hydroxyapatite of hard dental tissues, form a zone directly under the polymer hybrid layer that is resistant to acid-base effects, due to which, along with the release of fluoride, desensitizing and cariesstatic effects. When using total etching systems, the formation of an acid-base resistant zone is not observed. We draw your attention to the method of applying adhesive systems of the 6th and 7th generations: they should be thoroughly rubbed into the hard tissues of the tooth so that the residual acid is neutralized by hydroxyapatite crystals.
At present, it remains indisputable that self-etching adhesives are able to remove a layer of biofilm from the tooth surface less effectively than phosphoric acid in the total etching technique. Therefore, when choosing an adhesive system, one should take into account the location of the defect, the C-factor, age, etc. Thus, when making veneers and restoring class IV defects, it is necessary to give preference to proven adhesives of the 4th and 5th generations. The most common reason for failure to achieve a strong bond between the composite and tooth tissue is that the doctor deviates from the instructions for using a particular adhesive. But it is in the manual that the exact algorithm for clinical use, restrictions, precautions and interaction with other materials are listed. In addition, it is important to use a timer when working. The required pause of 30 seconds while the adhesive is absorbed and reacts with the dentin surface can easily become a pause of 10 seconds if the time is counted mentally (Edinakevich N., 2009). Therefore, for a high-quality result, not only the choice of an adhesive system is of much greater importance, but also careful adherence to all recommendations on the technology of its use.
Literature
- Blunk Uwe. Adhesive systems: review and comparison
// Dent Art. - 2003. - No. 2. - P. 5-11. - Ioffe E., Nesmeyanov A. Adhesive technology in modern dentistry
// New in dentistry. - 1994. - No. 4. - P. 26-27. - Nikolaev A.I., Tsepov L.M. Practical therapeutic dentistry
. - M.: MEDpress-inform, 2007. - 923 p. - Nikolaev D. A. Cannula applicators
// STIDent - 2012. - No. 1, - P. 20-21. - Mahn E. Adhesive technique - as simple as writing // DENTALLIFE. - 2008. - No. 5. - P. 4-4.
- Pashley David H. Development of dentine bonding: from “no etching” through “general etching” to “self-etching” //
- New in dentistry. - 2004. - No. 1. - P. 2-8.
- Waning A., Smidt A., Van Pelt H. Directions in adhesive dentistry, clinical perspectives
// Maestro of Dentistry. - 2003. - No. 2. - P. 73-75.
A closer look at the adhesion process
The two main steps to ensure adhesion, stability and ease of use are etching and polymerization methods.
Etching
In order to create adhesion on enamel and dentin, an “etching” stage is necessary. This is usually done using a solution of phosphoric acid.
There are 3 different etching techniques:
The obvious difference in the three methods presented is the use of phosphoric acid. The technique using orthophosphoric acid provides better surface demineralization of the enamel, but does not increase the patient's postoperative sensitivity. There is no obvious difference in response to cold between total etching and self-etching techniques.
“Enamel etching with phosphoric acid is very pronounced, effective and understandable,” says Dr. Burgess. “If you move to formulations with a pH of 2.3 to 3.2 (usual values for universal adhesives), these materials do not fully open the enamel interprismatic space, which can lead to microleakage and destruction of the restoration in the future.”
Universal adhesives can work in any etching technique and provide good quality adhesion, while total and selective etching techniques show the best adhesion to enamel.
The advantage of universal adhesives is that we can use them in total etch, selective and self-etch techniques,” says Dr. Burgess...
Polymerization
Dental cements are used to create indirect restorations. There are basically three options for curing cements. The curing process is also called polymerization.
There are three types of curing materials:
| Chemical Curing Materials | Light curing materials | Dual Lead Materials |
| Produced using a curing lamp. “Dentists use this polymerization option when there is limited access of the lamp to the illuminated surface or the thickness of the material layer does not provide confidence that the lamp light will be able to provide polymerization to the full depth,” explains Dr. Burgess. | Mandatory use of polymerization light. The composites mainly contain camphorquinone as a photoinitiator during polymerization. Dr. Burgess points out that the best adhesion and color stability is achieved by light curing the materials. | They can be polymerized both with the help of light and chemically. |
Dentists definitely need to know about the curing method of a particular material, because... Light-curing and chemical-curing materials cannot be used at the same time. Dual-cure materials can be used in any application.
“There are differences in the use of each material and some of them cannot be used together,” says Dr. Burgess. “If you use a light-curing adhesive and put a chemical-curing cement on top, that combination will not work.
However, dual action activators have been developed. They are mixed with adhesive. Adding an activator does not mean that the adhesive becomes a dual-cure compound, it means that the adhesive becomes compatible with dual-cure cements.”