Causes
There are two theories for the origin of osteomas: from the remnants of embryonic cartilage or from the periosteum of mature bone. In some cases, the occurrence of osteomas is associated with an inflammatory process or injury Source: Toropova I.A. Features of the clinical course of osteoma of the nose and paranasal sinuses / I.A. Toropova // Bulletin of RUDN University. — Medicine Series. - 2005. - No. 1(29). — P. 95-97. .
It is believed that the development of osteomas is also facilitated by:
- injuries;
- hypothermia;
- inflammation and previous infections;
- some diseases (rheumatism, gout, syphilis);
- genetic predisposition.
What is osteoma of the jaw?
This neoplasm is not considered an odontogenic disease - that is, it is not a complication of dental disease. This formation is formed from mature jawbone tissue and can develop on both jaws. The likelihood of osteoma does not depend on the gender of the patient. At the same time, age-related patterns in the development of the disease are noted - in most cases, osteoma is found in adults.
Based on the nature of development, the following forms of tumor are distinguished:
- Central osteoma growing deep in the bone tissue.
- Peripheral osteoma developing on the edge of the jaw bone - such tumor formations are called exostoses.
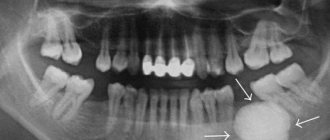
Osteoma is characterized by slow growth and in itself is not a source of pain. Therefore, especially with central localization of the tumor, the patient often does not have any complaints related to the tumor. With this development, osteoma is often discovered by chance - for example, from the results of an X-ray examination, the basis for which was suspicion of periodontitis. The complexity of treating the disease and the number of specialists involved in different fields depends on the specific case.
Osteoma of the mandible
Mature bone tissue serves as the basis for the formation of osteoma. Moreover, the tumor-forming tissue can have both a compact and spongy structure. A spongy neoplasm is characterized by disordered bone beams, the space between which is filled with connective tissue.
osteoma of the mandible grows, it can put pressure on the mandibular nerve, resulting in neurological problems. As the tumor grows on the condylar process, a decrease in the mobility of the lower jaw may occur. In some patients, the jaw may even become completely immobile. Osteoma of the upper jaw can grow into the maxillary sinuses, nasal passages and even the eye sockets. This leads to difficulty in nasal breathing on the side where the tumor is located, as well as to impaired eye movement. If the osteoma is located near the hard palate and alveolar process, then problems may arise when installing dentures. If the tumor is large, it can disrupt the symmetry of the face.
Osteoma of the maxilla
Types of osteoma of the jaw
Tumor formations in the jawbone may differ in the structure of the bone tissue that forms them, as well as the nature of their development. In this regard, the following types of this neoplasm are distinguished:
- Tubular osteoma, which is a tumor of a regular spherical shape, formed by tissue whose structure is indistinguishable from the surrounding healthy tissue of the jaw (that is, in fact, being its continuation).
- Compact osteoma, characterized by a large width of the base or pedicle.
- Intraosseous osteoma, characterized by clear boundaries and therefore clearly visible against the background of the adjacent bone.
Symptoms
The symptoms of a tumor depend on where it is located. But a number of clinical signs stand out:
- located on flat, tubular bones, vertebrae, in the walls of the paranasal sinuses, on the surface of the skull;
- immobility;
- density;
- with a smooth surface;
- with clear boundaries;
- does not hurt when pressed.
Osteoma may not make itself felt for a long time and not interfere, but if it grows too large, it begins to put pressure on neighboring tissues and bones, which causes the corresponding symptoms:
- pain;
- if the tumor is in the nasal paranasal sinuses, drooping of the eyelid (ptosis), blurred vision, etc.
- memory problems, epilepsy (if located on the inner surface of the skull);
- lameness (if localized on the bones of the legs);
- nosebleeds, difficulty breathing (if the tumor is located in the maxillary sinus area).
Table of symptoms, depending on the location of the tumor
| Tumor location | Description of symptoms |
| Posterior wall of the frontal sinus | Persistent headaches, increased intracranial pressure |
| Inferior wall of the frontal sinus | Protrusion of the eyeball visible to the naked eye |
| Nasal cavity | Difficulty breathing through the nose, lack of smell, double vision, drooping eyelid, protrusion of the eyeball, blurred vision |
| Paranasal sinuses | Deterioration of vision, pain |
| Frontal bone | Headaches, memory loss, increased intracranial pressure, seizures |
| Occipital bone | Frequent headaches, epileptic seizures |
| Femur, talus, tibia | Unusual gait, swelling of the legs, muscle pain while walking |
| Temporal and parietal bones | Only an aesthetic defect, no unpleasant symptoms |
| Knee-joint | The tumor makes it difficult to walk normally |
| Edge | Chest pain |
| Vertebrae | Scoliosis develops |
| "Turkish saddle" | Hormonal disorders |
When to see a doctor
If signs of pathology appear, the only correct decision is to consult a doctor. The answer to the question of which doctor treats osteoma depends on the location of the tumor. You should make an appointment with a doctor if you experience:
- paroxysmal headaches, muscle cramps, problems with memory and concentration (localization in the skull);
- deformation of the skull, severe pain, breakdown with chewing (osteoma of the jaw);
- difficulties when moving, etc.
If signs appear, the patient must contact a traumatologist, who, based on the results of the examination, will refer to a specialist (maxillofacial surgeon, neurosurgeon).
Our clinic in the center of Moscow offers the services of highly qualified doctors - specialists of the highest categories. They have knowledge and experience in diagnosing and treating osteoma.
Types of osteomas
Depending on the origin of osteomas, there are:
- Heteroplastic
- formed from connective tissue. This includes osteophytes. They are found not only on bones, but in soft tissues and organs - in the diaphragm, tendon attachment points, lining of the heart, etc. - Hyperplastic
- formed from bone tissue. This group includes osteoid osteomas and osteomas.
Let's look at the subspecies that belong to two main groups.
1) Internal and external osteophytes
.
- The internal ones are called “enostoses”, they grow into the bone marrow canal. Usually solitary, except for osteopoikilosis. They do not produce symptoms and are usually discovered incidentally when a person has an x-ray.
- External ones are called “exostoses”. They grow on the surface of the bones and can appear for no reason or due to certain pathological processes. Causeless exostoses usually appear on the bones of the skull, facial and pelvic bones. They may not cause symptoms and may only be an aesthetic defect or put pressure on neighboring organs. In some cases, a fracture of the exostosis leg occurs and bone deformation occurs.
2) Osteoma
– does not differ in structure from bone tissue, usually found on the facial and cranial bones, including the paranasal sinuses. Bone osteoma is diagnosed twice as often in men, in the area of the facial bones – three times more often. These are almost always single tumors, but with Gardner's disease multiple tumors can grow on long bones. They are painless and do not cause symptoms, but when adjacent structures are compressed, various symptoms appear. Separately, there are multiple congenital osteomas of the cranial bones, which are combined with other developmental defects.
3) Osteoid osteoma
– highly differentiated bone tumor. However, it has a different structure - it consists of vascular-rich elements of osteogenic tissue, zones of bone tissue destruction, and bone beams. Usually there is no pain 1 cm in diameter. It is a common disease, accounting for approximately 12% of all benign bone tumors.
Osteoma of the condylar process of the mandible
Osteoma is a benign tumor of bone tissue, occurring in 2.7-5.9% of patients with benign tumors of the facial bones. Currently, it is suggested that the number of true osteomas is significantly smaller, since this diagnosis is often mistakenly made in cases of reactive hyperplasia, exostoses of the jaws, and some forms of fibrous dysplasia [3, 17].
Osteomas, as a rule, grow very slowly and painlessly, without making themselves felt for a long time. Their clinical picture is mild and depends on the location and size of the tumor. Developing in the area of the body of the lower jaw, osteomas lead to deformation of the corresponding area, aesthetic and functional disorders. Osteomas of the upper jaw with significant sizes cause exophthalmos, diplopia, lacrimation, impaired nasal breathing and neuralgic pain due to compression of the branches of the trigeminal nerve. When localized in the area of the frontal sinus and ethmoid labyrinth, the tumor is capable of deforming the walls of the sinuses, destroying them, growing into the orbit and cranial cavity [3, 15].
Damage to the condylar process of the mandible is quite rare and is characterized by specific symptoms. Osteomas of this localization present a certain difficulty for diagnosis and surgical treatment, remaining asymptomatic for a long time, but in later stages they can cause severe aesthetic and functional disorders [3, 9, 17].
Osteoma of the condylar process was first described in detail by Eckert (1899), pointing out displacement of the lower jaw, impaired mouth opening, as well as changes in facial contours on the side of the lesion of the condylar process of the mandible among its main clinical manifestations [1]. Subsequently, a few reports were presented in the literature, mainly about isolated observations of this disease [1, 11, 13, 14]. Deboise A. (1981), noting that osteoma is the most common benign neoplasm of the structures of the temporomandibular joint (TMJ), provides only 3 of his own observations [9]. The largest number of clinical observations of osteomas of the condylar process - 23 - belongs to H. Zhang (1997) [18]. The author, however, does not indicate whether in all cases the diagnosis of true osteoma was confirmed histologically.
Clinical observation
Patient K., 36 years old, medical history No. 4408 dated March 19, 2004, was admitted to the maxillofacial department No. 2 of City Clinical Hospital No. 12 in Kiev with complaints of facial deformation due to displacement of the lower jaw, malocclusion, difficulty chewing food, crunching in the left TMJ, moderate pain with increased load on the joint. For the first time, he noticed a facial deformity—a displacement of the chin to the right—in November 2002. Later, a clearer clinical picture emerged; the severity of the displacement and malocclusion slowly progressed until the moment of treatment. Objectively, the patient had pronounced facial asymmetry due to displacement of the lower jaw to the right (Fig. 1).
Rice. 1. The chin is shifted to the right side, a state of physiological rest.
In the pretragus area, the laterally displaced head of the left TMJ was clearly palpated. Mouth opening was up to 4.5 cm, with a crunch in the area of the left TMJ and a Z-shaped deviation of the lower jaw. Lateral movements of the jaw to the right were limited, the bite was oblique, and the midline shifted to the right by 1 cm (Fig. 2).
Rice. 2. In the pretragus area, the laterally displaced head of the left TMJ is clearly palpated.
A series of radiographs (orthopantomogram, radiograph of the mandible in direct projection and in the Haenisch position on the left, computed tomogram of the joint area with 3D reproduction) revealed a shadow of bone density with a size of 2x1.7 cm, associated with the left condylar process and located in the infratemporal fossa. The structures of the left TMJ were preserved, although somewhat deformed. When planning surgical intervention, a stereolithographic model of the patient’s skull was made (Fig. 3), on which the necessary measurements were made and the surgical approach was determined.
Rice. 3. Stereolithographic model of the skull, neoplasm of the left condylar process of the mandible.
On March 23, 2004, the patient underwent surgery: removal of a neoplasm of the condylar process of the lower jaw under endotracheal anesthesia with intubation through the nose. To do this, a preauricular and semicoronal approach was provided to the zygomatic arch, which was then resected and displaced downward on the fibers of the masseter muscle (Fig. 4).
Rice. 4. Surgical wound, coronal access, osteotomy of the zygomatic arch: 1 - zygomatic arch, 2 - osteotomy areas.
The fibers of the temporalis muscle were partially transected and detached, allowing access to the infratemporal fossa, where a bone formation was visualized anterior and medial to the head of the jaw (Fig. 5).
Rice. 5. The area of the infratemporal fossa, access to the tumor has been created.
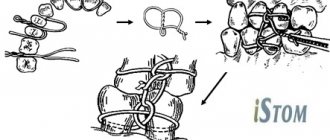
The tumor is separated from the soft tissues and fixed using a special bone fixation made in the form of a corkscrew (Fig. 6).
Rice. 6. Macroscopic specimen of osteoma of the condylar process of the mandible.
The tumor was removed within the healthy bone. The zygomatic arch is placed in place and fixed with two wire bone sutures. The soft tissue flap was put in place, the wound was sutured in layers. The postoperative period proceeded without complications. Closing of the jaws in the correct position was noted the next day after surgery without any orthopedic measures (Fig. 7).
Rice. 7. State of physiological rest of the lower jaw on the first day after surgery. Closing of teeth in a physiological occlusion with restoration of the midline.
The radicality of tumor removal was confirmed by computed tomography data (Fig. 8).
Fig.8. Facial symmetry, state of physiological rest, 9 years after surgery.
Vertical movements of the lower jaw were fully restored on the 5th day. There was a slight paresis of the frontal and zygomatic branches of the facial nerve, the function of which was completely restored on the 7th day after surgery. Postoperative swelling of the temporal and zygomatic areas persisted for 8 days. On April 2, 2004, the patient was discharged in satisfactory condition with recommendations for rational prosthetics.
On January 16, 2013, patient K. underwent a repeated scheduled examination using clinical and instrumental research methods. The patient did not have any complaints from the TMJ. On bilateral palpation of the TMJ, no crunching or crepitus was observed, and there were no pain symptoms. Objectively: the contours of the face are symmetrical, the maximum opening of the mouth is 4 cm (Fig. 9, 10), the midline of the face is restored, the movements of the lower jaw are not limited, without signs of lateral deviation.
Rice. 9. Maximum mouth opening, 9 years after surgery. Rice. 10. Orthopantomogram, 9 years after surgery.
According to an orthopantomogram and computed tomography in 3D reconstruction mode, the structural elements of the left TMJ have clear anatomical contours and the structure of bone tissue is within normal limits. The relationship between the condylar process and the glenoid fossa ensured the functional stability of the TMJ and was considered acceptable (Fig. 11, 12).
Fig. 11. Computed tomography data. Rice. 12. 3D reconstruction of the skull, 9 years after surgery.
Discussion
Localization of osteoma in the TMJ region is a rare clinical situation. The paucity of clinical symptoms characteristic of osteomas determines the dominance in the clinical picture of nonspecific functional disorders of the TMJ, which makes it necessary to carry out differential diagnosis with other diseases of the joint - hyperplasia of the branch, deforming arthrosis, ankylosis, intra-articular disorders, habitual dislocation, etc. X-ray studies in standard settings are quite informative for making a correct diagnosis, but are clearly insufficient for choosing a method of surgical treatment. To clarify the localization of the tumor, taking into account the changed anatomical relationships, its relationship with the elements of the joint and the nature of structural changes in the latter, it is necessary to conduct computed tomography with 3D reconstruction. A thorough examination allows you to decide on further surgical tactics.
When the osteoma is anteromedial in relation to the condylar process, it is located in the region of the infratemporal fossa. Removing the tumor in this case is associated with significant difficulties, and sometimes even with a risk to the patient’s life. Chen Y. (2003) states that when the tumor is localized in the area of the articular process, in most cases its resection followed by arthroplasty and orthopedic treatment is indicated [8]. Other authors adhere to the same point of view, recommending combining resection of the condylar process with subsequent plastic surgery of the joint, lengthening of the ramus, combined operations on the upper and lower jaw to correct the bite and hardware treatment [4, 7, 18]. At the same time, the above observation indicates that in some cases it is possible and even necessary to remove the tumor while preserving the elements of the joint. This is also evidenced by the data of Piattelli A. (1995) and other authors [11, 13].
It should be noted, however, that when the osteoma is anteromedial in relation to the condylar process (according to the literature, this is the most typical localization), it is located in the region of the infratemporal fossa. This area is surgically extremely difficult to access and is located near vital structures, so removing the tumor in this case is associated with significant difficulties and sometimes even a risk to the patient’s life.
The main anatomical obstacles to reaching the infratemporal fossa are the zygomatic arch, the ramus of the mandible, the parotid gland and the facial nerve - formations that are extremely important in functional and aesthetic terms. Access to the tumor should be sufficient for its radical removal and provide a good overview.
Currently, a number of options for surgical access to the infratemporal fossa have been proposed, more or less satisfying these requirements, but not all of them are appropriate in the case of osteoma of the condylar process.
In 1961, JF Barbosa developed an approach to the infratemporal fossa, which involved performing a Weber-Fergusson incision followed by mobilization of the zygomatic complex and resection of the mandibular ramus [6]. DJ Crockett (1963), using a similar approach, limited the resection of the branch to the coronoid process only [10, 16]. This so-called anterior route is usually combined with maxillary resection and provides a wide view, but at the same time it is very traumatic and unfavorable from a cosmetic point of view. The infratemporal fossa can also be achieved by making a premaxillary incision followed by osteotomies of the mandibular ramus at various levels, rotation or removal of the bone fragment from the surgical site. In case of resection of a section of the branch, the latter can be returned to its place at the end of the operation and fixed in the form of a free autograft [16].
The main anatomical obstacles to reaching the infratemporal fossa are the zygomatic arch, the ramus of the mandible, the parotid gland and the facial nerve - formations that are extremely important in functional and aesthetic terms. In 1985, NR Attenborough proposed the use of a coronal approach to visualize the structures of the pterygopalatine and infratemporal fossa. This method involved making pre-auricular and semi-coronal incisions with subsequent removal of the zygomatic arch and coronoid process [5]. HL Obwegeser improved this technique by combining mobilization of the entire zygomatic complex with osteotomy of the coronoid process. In this case, the zygomatic bone was displaced downward on the fibers of the masticatory muscle, and the coronoid process was retracted upward [12]. In addition to the above, numerous modifications and combinations of access are used depending on the clinical situation [10]. As our experience shows, the use of coronary access is the method of choice when removing tumors localized in the infratemporal fossa. It provides a good overview and freedom of surgical manipulations, avoids injury to large vessels and branches of the facial nerve, and is also most cosmetically acceptable.
We also note that with long-growing bone tumors in the TMJ area, the joint can undergo significant morphofunctional changes that require postoperative orthopedic correction, however, as was shown in our observation, the compensatory capabilities of the joint are quite high, which in some cases with low-traumatic and radical removal tumor allows you to achieve restoration of function without additional measures in the postoperative period.
Thus, observation of the patient in the long term after surgery (9 years), indicating a relapse-free course and the absence of deep functional disorders, confirms the effectiveness of the approaches used to remove the TMJ tumor. Careful diagnosis and surgical intervention using approaches that provide wide access to the infratemporal fossa allowed for radical removal of osteoma of the condylar process of the mandible, while avoiding additional trauma to the anatomical formations of this localization, providing a quick postoperative recovery period and a satisfactory result for 9 years with complete restoration of TMJ function.
Tumor diagnosis
To establish that the tumor is indeed an osteoma, the following procedures are performed:
- X-ray;
- CT scan;
- Magnetic resonance imaging;
- rhinoscopy of the nose;
- histological examination of part of the tumor tissue.
During diagnosis, the doctor must determine:
- degree of functionality of the affected limb or tissue;
- pain of the tumor when pressed;
- the growth rate of the tumor by the ratio of its size and the duration of the presence of pathology in the patient;
- location of osteoma.
The main method of diagnosis is radiography
. On the image it will look like a homogeneous round tumor with clear boundaries. Osteoid osteoma in the image is a vague defect - a focus of destruction.
- Radiography allows you to find out: the location of the osteoma in the bone, the structure of the tumor, the degree of destruction of the bone on which the tumor is located, and also determine whether the tumor is a single tumor or multiple growths.
- The benign nature of the tumor is confirmed by slow growth, regular structure and geometry, clear contour, and minimal calcification.
- A blood test is also prescribed because the blood formula is of great importance.
- For very small osteomas, radiography is not informative, so computed tomography is performed, which allows one to visualize the smallest details of the tumor structure and measure the size of destruction.
- Differential diagnostics with chronic Brody's abscess, osteochondrosis dissecans, osteoperiostitis, sclerosing osteomyelitis, and osteogenic sarcoma are mandatory. This applies to osteoid osteomas.
Diagnosis of osteoma
If a patient is suspected of having osteoma, diagnosis is carried out using all diagnostic methods (clinical and radiological). The main goal of diagnosis is to determine the nature of the tumor. The list of diagnostic methods includes:
- palpation;
- blood analysis;
- x-ray to assess the functioning of the affected areas (joints);
- MRI to accurately determine the type of tumor;
- computed tomography with 3D reconstruction to determine the size and density of the pathology and select the appropriate course of treatment;
- histological analysis (biopsy) to exclude the possibility of developing an oncological process;
- scintigraphy;
Treatment of osteomas
If the tumor does not cause any discomfort to the patient, then medical specialists recommend observational tactics. If a small osteoma stops growing, it does not need to be treated or removed.
Osteoma is treated only surgically. Indications for removal are as follows:
- too big size;
- pain caused by osteoma;
- cosmetic defect.
Removal is carried out if the osteoma compresses neighboring organs, causing pain and discomfort, is an aesthetic defect, changes the shape of bones, causes scoliosis, limits a person’s mobility, and provokes pain. Most often, specialists remove tumors in the sinuses, jaws, ear canals, hip and knee joints.
Preparation for the operation is standard. These include blood and urine tests, ECG, fluorography, consultations with a therapist and anesthesiologist. The intervention is carried out under general anesthesia; you need to spend from 1 to 3 days in the hospital, depending on the extent of the operation performed.
The SM-Clinic employs some of the best maxillofacial surgeons and neurosurgeons who perform minimally traumatic operations using modern techniques and instruments.
During the operation, soft tissues are dissected; access can be external or internal - through the mucous membranes of the mouth and nose. The tumor and part of the soft and bone tissue surrounding it are removed to avoid recurrence.
Basic removal methods:
- curettage – external access, tumor removal, curettage of the tumor focus;
- complete removal – indicated for osteomas in the sphenoid sinus;
- endoscopic removal - is carried out for small tumors and difficulties in accessing them, CT is necessarily used to monitor the progress of the intervention, the duration of the operation is about two hours.
If the removal was not completed completely, then in 10% of cases a relapse occurs. Therefore, it is important to contact a reliable clinic and an experienced surgeon.
Another method for removing osteomas is laser evaporation. A laser beam is directed at the tumor, which actually burns it out. Typically this technique is used for small tumors.
Treatment of osteoma and prognosis
If the tumors are small and do not cause symptoms, it is enough to observe the development of the tumor. In other cases, treatment consists of surgical removal of the tumor. During the procedure, it may turn out that in order to completely get rid of osteoma, it is necessary to remove fragments of healthy bone. These cavities are then filled with special materials, most often titanium plates. In some cases of osteomas from the cranial region, it is possible to perform the procedure through a less invasive transnasal approach using the endoscopic method. Osteomas are benign formations, so the prognosis is good. These tumors do not metastasize to distant tissues, and their harmful effects mainly depend on their location.
Prevention
There are no special preventive measures to prevent the occurrence of osteoma. Doctors recommend taking an x-ray every year to detect the tumor in a timely manner and, if necessary, remove it.
Specialists of the medical surgical department successfully perform operations to remove various types of osteomas. If you notice a lump on any bone, contact a specialist who will make a diagnosis and promptly prescribe treatment.
There is no special prevention for this disease. The main cause of osteomas is considered to be genetic predisposition.
Some recommendations:
- avoid injury;
- timely cure diseases of the musculoskeletal system;
- undergo examination if any neoplasms of unknown origin are detected.
Osteoid osteoma
Osteoid osteoma of the jaw is a type of benign bone formation that is rarely encountered in dental practice. It is usually detected in adult men and is localized on the lower jaw.
The formation is loose, has a gray-red or just red color. Adipose tissue and bone marrow cells are absent, osteoid fibers are calcified and vary depending on the level of maturity.
Osteoid osteoma of the mandible
Symptoms
The main symptom is constant or paroxysmal aching pain that tends to intensify in the evening. Periostitis may also be observed at the site of osteoid osteoma. During a medical examination, the doctor will easily identify it.
On x-ray, the affected area has uneven borders and a rounded shape. The size and width of the benign bone tissue of the compaction is directly related to the neglect of the pathological process.
Treatment
Like all bone tumors, osteoid osteoma can only be removed surgically. First, the dental surgeon administers general anesthesia. Then the tumor is cleaned out or the destructive part of the jaw is removed. To avoid recurrence, all pathological tissue must be removed.
After the operation, the functionality of the jaw is restored using a metal wire implant. The price of the operation depends on the degree of advanced disease and the complexity of the resection.
Popular questions
Can osteoma lead to cancer?
No. Osteoma is a benign tumor. It can cause adverse health effects if it grows into the cranial cavity. But the probability of degeneration into cancer is close to zero.
What causes osteoma?
The causes of the tumor are unknown. The role of hereditary predisposition has been established. If your relatives have been diagnosed with osteoma, you are more likely to develop it than the average population. The trigger for the growth of osteoma can be a bone injury or an acute inflammatory process. There is also a theory of intrauterine developmental defects. The reason for its occurrence was the fact that osteoma most often develops at the junction of the frontal and ethmoid bones, where membrane and cartilaginous tissues develop during embryogenesis.
Is it necessary to remove the osteoma?
The tumor grows very slowly. In most cases it is not dangerous. Only clinically significant osteomas that can grow into the orbit or skull bones are removed. The operation can also be performed for aesthetic reasons.
Sources:
- Kudaibergenova S.F. Osteoma of the nasal cavity / S.F. Kudaibergenova [and others] // Bulletin of KAZNMU. - 2012. - No. 2. - P. 92-93.
- Toropova I.A. Features of the clinical course of osteoma of the nose and paranasal sinuses / I.A. Toropova // Bulletin of RUDN University. — Medicine Series. - 2005. - No. 1(29). — P. 95-97.
The information in this article is provided for reference purposes and does not replace advice from a qualified professional. Don't self-medicate! At the first signs of illness, you should consult a doctor.
Types of osteoma
Osteomas are dense formations of the bone structure, most often located inside the skull, where they reach sizes of 1-4 cm. They are less common on the surface of other bones; if they appear, they become larger. A type of osteoma is osteoid osteoma. Like osteoma, osteoid osteoma is a benign bone tumor. It differs in location because it most often concerns the long bones and bones of the pelvis or scapula. It also happens to occur inside the vertebrae. Osteoid osteoma does not exceed a few centimeters in diameter and most often occurs in young men. A very characteristic feature of this neoplasm is the occurrence of pain after exercise, during night rest and pain relief under the influence of salicylates.
Another type of osteoma is osteoblastoma, a rare primary bone cancer. Most often this is a benign tumor, but in the literature there are cases where osteochondritis showed an aggressive course, reminiscent of bone sarcomas (malignant tumors).
This type of cancer is located in the long bones and bony parts of the spine. As with osteoid osteoma, patients with osteoblastoma do experience bone pain that does not go away with medication. The tumor grows larger than other types of osteomas and is most common in young people.
Diagnosis and differentiation
When a person discovers a lump in the lower or upper jaw, he must see a specialist. This is a pathology where it is impossible to diagnose or treat it on your own. Patients often come to specialists at an advanced stage, when osteoma has affected large areas of the jaw. It happens that the tumor is found by an ENT doctor during a standard appointment.
To diagnose osteoma of the upper and lower jaw, there are the following methods:
- Collection and analysis of information about the disease (history) based on a conversation with the patient;
- Visual inspection and palpation. The doctor determines the size of the osteoma itself, location, appearance;
- X-ray of the jaw. In the picture, osteoma is a spherical or oval compaction with a noticeable border. If images of the tumor and tooth root are combined, then osteoma is confused with odontoma. The compact peripheral appearance of osteoma is easily diagnosed (it is mainly located on the outer side of the lower jaw). A tumor located on cancellous bone tissue has a heterogeneous color in the image, because it has a heterogeneous structure, having different densities in different areas;
- Computed tomogram of the maxillofacial apparatus;
- Scintigraphy (used if x-ray examination does not help determine an accurate diagnosis);
- Biopsy of tumor tissue. Used to determine the degree of danger of osteoma;
- Biopsy of the inflamed lymph node under the jaw (near the place where the tumor is located);
- Consultation and examination with an ENT doctor and an ophthalmologist (more often with osteoma of the upper jaw, when the tumor reaches the bones of the orbit and nasal sinuses);
- Phonoscopy and rhinoscopy (more often necessary for maxillary osteoma);
- Puncture of the sinuses (if necessary);
- Maxillary sinusotomy (if necessary).
The main task of the doctor at the examination stage is to determine an accurate diagnosis, that is, to differentiate osteoma of the jaw from other neoplasms and pathologies:
- Hyperostosis (excessive accumulation of bone substance in unchanged bone tissue, inflammation of the periosteum);
- Odontoma (a benign tumor consisting of pathologically growing dental tissue; purulent fistulas sometimes appear);
- Osteoid osteoma (differing in cell composition, but being a benign tumor);
- Fibrous osteodysplasia (a defect in the growth and development of bone tissue; on an x-ray it looks like a spongy osteoma; it develops in childhood, adolescence, when the body (including bones) is still growing);
- Chondroma (similar to spongy osteoma; consists of mature cartilaginous cells; is rarely formed in the jaw bones, more often localized in the tubular bones of the arms; can transform into chondrosarcoma, malignant in nature);
- Intraosseous sclerosis (does not have a clear boundary between healthy cells and diseased cells; bone tissue becomes excessively dense and interferes with normal blood flow);
- Salivary stone (the main difference is severe pain when the salivary duct is blocked by a stone; the pathology is typical for people with chronic diseases (diabetes mellitus, urolithiasis, gout), lack of vitamin A and excess vitamin D);
- Osteoid-osteoma (a distinctive feature is pain from the moment the tumor appears, intensifying at night; a small tumor that does not deform the bone);
- Exastosis (in the X-ray image it does not differ from osteoma, it has clearly visible boundaries).
Reasons for development
The exact mechanism of tumor development is unknown. It is generally accepted that odontogenic tumors develop under the influence of malformations of jaw tissue.
Provoking factors:
- chronic inflammatory process of tissues of the jaws and adjacent organs;
- the impact of filling composition and other foreign objects on the maxillary sinus;
- damage to the jaw bones and soft tissues due to bruises and other mechanical impacts;
- the effect of nicotine, alcohol and other chemicals on the oral cavity.
Malignant tumors develop due to the spread of metastases from cancerous tumors in other organs.
Treatment
Surgery is the only way to treat this type of tumor. Neither folk recipes from healers nor medications will help get rid of a benign tumor. There are clear medical indications for surgical intervention:
- There is constant pain that can increase;
- Cosmetic discomfort in the patient;
- Chewing dysfunction;
- Obstruction to the installation of dentures, braces, crowns.
After the examination, where an accurate diagnosis is made, the size and location of the tumor, a surgical operation is performed. It is often combined with surgical plastic surgery.
The voids left by tumor removal need to be filled with something. The best material to fill the void is the patient's own tissue.
The surgeon performs an operation to excise osteoma of the jaw through the oral cavity, and the patient is given general anesthesia:
- The doctor frees the tumor for further manipulation by cutting the soft tissue and mucous membrane;
- Then holes are drilled into the neoplasm;
- The tumor is removed with a special surgical chisel;
- Plastic surgery as needed. The resulting void is filled with the tissues of the patient’s own body;
- The bone must be ground and the incision is sutured.