A child has a sore throat: what and how should parents do in this case?
consultation with a pediatrician at a medical center Sore throat is one of the common reasons for outpatient and emergency visits by parents of children to doctors for help. Upper respiratory tract infections are very common in both children and adults and have significant economic consequences associated with the frequent prescribing of antibiotics by physicians, even when the causative agent is not bacteria. About a quarter of children suffering from tonsillitis also suffer from bacterial pharyngitis. Identification and adequate antibiotic treatment of group A streptococcal sore throat is important for the primary prevention of acute rheumatic fever, which occurs in 3% of cases. Therefore, in any case, if you have a sore throat, you need to show your child to a doctor to rule out diseases that are dangerous to health and life.
Immunity in children. Why do children get sick more often?
The immune system of children develops throughout childhood.
The immunity of infants is imperfect and this feature is a special mechanism that protects the body from too violent immune reactions to infections.
In the first weeks of life, the baby is protected by the antibodies that he received from his mother and then continues to receive them through breast milk. But such protection is sometimes not enough.
Moreover, while immunity is just developing, periods of maximum risk of developing infectious diseases arise; they are called critical periods:
First critical period
This is a period of vulnerability for newborns, which occurs in the first 28 days of life. During this period of time, the child’s body is protected only thanks to antibodies received from the mother through the placenta and breast milk. The risk of contracting bacterial and viral infections during this period is very high. Premature newborns are a special risk group.
Second critical period
Lasts from 4 to 6 months of life and is accompanied by a decrease in the amount of maternal antibodies.
Due to some mechanisms, which are also still poorly developed, the child’s own antibodies are produced, but they are not yet sufficient to protect the baby. Therefore, the body’s susceptibility to airborne and intestinal infections during this period is also high. Thus, in children under one year of age, all the basic mechanisms of the body’s defense against bacteria and viruses are weakened.
Third critical period
Occurs in the 2nd year of life. It is from this age that the child begins to have more and more contact with the outside world and various infections. The child's sensitivity to respiratory and intestinal infections is still high. The baby's immune defense mechanisms are not yet fully developed.
Fourth critical period
Appears at 6-7 years of age. Children of this age are also prone to infectious diseases, as some indicators of the immune system change.
Fifth critical period
Adolescence from 12-15 years, and the age may vary slightly for boys and girls. This is due to an increase in the secretion of sex hormones, which slightly weakens the immune system. Children of this age are characterized by high sensitivity to viral infections.2
How does a sore throat manifest?
The main symptom of a sore throat is pain, both at rest and when swallowing or talking. A sore throat is the primary symptom of pharyngitis. The terms "angina" and "pharyngitis or pharyngotonsillitis" are often used interchangeably. Pharyngitis refers to objective signs of inflammation of the pharynx: swelling, exudation, ulceration or obvious erythema. Redness of the throat may occur as part of a general redness of all mucous membranes of the upper respiratory tract in young patients with fever. The diagnosis of pharyngitis is justified only when the pharynx is objectively redder than the rest of the mucous membranes.
Non-drug therapy
Treatment of acute laryngitis depends on the age of the child. This may include:
- compliance with bed rest;
- limiting vocal load (for 5–7 days it is better for the baby to remain silent or talk as little as possible);
- maintaining the optimal temperature (+18…+20°C) and air humidity (50–70%) in the room where the sick child is located;
- drink plenty of fortified drinks (the liquid should be warm and unsweetened);
- following a hypoallergenic diet - if there are symptoms of laryngitis, it is strictly not recommended for a child to give sour, spicy, too hot or cold foods and carbonated drinks.
When treating inflammation of the mucous membrane of the larynx, children are allowed to apply wet and dry warming compresses to the neck area and gargle with a warm infusion/decoction of chamomile or sage, if recommended by a doctor.
What could be the causes of a sore throat?
Most often, sore throats are caused by viruses. Less commonly, sore throats occur due to bacterial infections. Viral pathogens such as corona virus, rhinovirus, adenovirus, influenza and parainfluenza are the most common and usually present as a cold. Other viral infections that may present with a sore throat are the Epstein-Barr virus and HIV, which lead to the development of a sore throat early in the disease.
Recurrent tonsillitis may occur due to cytomegalovirus or fungal infections in young patients with immunodeficiency.
Among bacterial infections, group A beta-hemolytic streptococcus (GABHS) is the most common cause of bacterial sore throat. It accounts for 15–36% of cases of acute pharyngitis in children in developed industrial countries. Other pathogens may include streptococci types C and G.
Rarer causes of sore throat include infections with Staphylococcus aureus, Mycoplasma, Chlamydia pneumoniae, Moraxella catarrhalis and Yersinia.
Fusobacterium necrophorum infection is an uncommon infection that begins with fever and sore throat and may subsequently develop into Lemierre's syndrome, which is characterized by blood poisoning, thrombosis of the internal jugular vein, and at least one metastatic site of infection.
Another group of causes of sore throat in children are peritonsillar, retropharyngeal and lateral pharyngeal abscesses, which arise due to the spread of infection from local sources, for example, bacterial tonsillitis. Along with fever and sore throat, these cases may present other symptoms such as painful swallowing, drooling, trismus, visible swelling under the lower jaw and deviation of the uvula away from the source of inflammation.
Allergies can also be the cause of a sore throat, especially when it is complicated by nasal bleeding. Irritants such as dust, tobacco and silt stove smoke, and chemical air pollutants can lead to chronic sore throat.
Talking for a long time in a raised voice or shouting for a long time also lead to a sore throat.
A sore throat can also occur due to damage to the larynx by stomach acid due to gastroesophageal reflux disease (GERD).
Drug therapy
How to fight infection?
Drug therapy for laryngitis that appears in a child against the background of an acute respiratory infection includes the use of antiviral and immunomodulatory drugs.
Antihistamines, which are usually prescribed for allergies, help relieve swelling of the mucous membrane and calm the baby. They should be given before bedtime, strictly according to the recommendation of the attending physician. What to do if you have a cough?
Remedies for this symptom are another essential component of treatment.
In the early stages of laryngitis, if a child has a dry hacking cough, drugs that block the cough center are used. Next, at the first signs of coughing, mucolytics are prescribed to thin the mucus and improve expectoration of sputum. Doctor MOM® cough syrup has similar properties. This complex herbal medicine, containing extracts of 10 medicinal plants, helps not only to liquefy mucus, but also to relieve swelling and inflammation. Herbal syrup is approved for long-term use in the treatment of laryngitis in children over 3 years of age. Actions at temperature.
If a child has a hard time tolerating a high temperature, he is prescribed an antipyretic. Treatment of laryngitis with antibiotics is justified only in the presence of serious bacterial complications and only as prescribed by a doctor.
What signs of the disease are assessed by the doctor?
When collecting an anamnesis and examining a child, the doctor will pay attention to the following symptoms:
- Onset and duration of sore throat
- Severity of fever
- Associated cough, runny nose, conjunctivitis, headache, myalgia (muscle pain)
- Any difficulty breathing, especially snoring at night or stridor
- History of rash, diarrhea, or allergies
- Regurgitation (reflux of gastric contents into the esophagus), pain in the epigastric or retrosternal region.
- Family history of sore throat in the past 2 weeks.
- Similar complaints in the past,
- Vaccination history
When examining the throat, the doctor may reveal:
- White or gray plaques on the surface of the tonsils or pharynx that rub off easily without bleeding.
- Ulcerations
- Plaques in the form of films, characteristic of infectious mononucleosis, diphtheria and sometimes streptococcal infection. Tularemia can also be a rare cause of such plaques.
- Films of gray or black color, extending beyond the tonsils, with swallowing problems and the absence of severe fever, are characteristic of diphtheria.
- Oral thrush, which is common in newborns and infants, may have a pseudomembrane (curdled plaques), the removal of which can cause mild pinpoint bleeding.
- Convexity of the oropharynx or lateral displacement of the uvula indicates a parapharyngeal or peritonsillar abscess.
- Herpetic sore throat is characterized by painful vesicular (bubble-like) formations on the pharynx and tonsils. Herpes simplex causes painful blisters limited to the front of the mouth, which can sometimes spread to the front of the tonsils.
- Lymphadenopathy (enlarged and painful anterior and posterior cervical lymph nodes is characteristic of bacterial tonsillitis or Epstein-Barr virus infection.
- Streptococcal pharyngitis is characterized by sore throat, temperature ≥38.3°C, tonsil and pharyngeal plaque, and cervical lymphadenopathy.
- Cough, runny nose and diarrhea are more common with viral pharyngitis.
Still have questions?
Get an online consultation from leading pediatricians in St. Petersburg!
A professional and experienced pediatrician will answer your questions.
Medical care for a child without leaving home at a convenient time.
sign up for a consultation
A Skype consultation lasts 45 minutes.
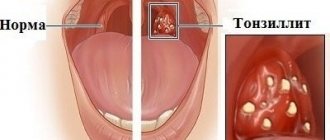
What is a sore throat?
Sore throat, or tonsillitis, is a disease in which an inflammatory process occurs in the palatine tonsils, or, in other words, tonsils. Tonsils are a collection of lymphoid tissue. They perform the most important function in the body - protective. If bacteria or viruses enter the body during breathing or through food intake, the tonsils “meet” them first, neutralize them and remove them from the body. As long as the number of pathogenic microorganisms does not exceed the permissible norm, the tonsils easily cope with their task, but as soon as the microorganisms become active, the tonsils begin to work doubly intensely, as a result of which an inflammatory process occurs in them. The body begins to produce an increased number of white blood cells to cope with enemies. And such a “fight” lasts three to four days until the pathogens are eliminated. But the situation is complicated by the fact that inflammation is accompanied by swelling, enlarged tonsils and other unpleasant symptoms, which will be discussed later.
Additional research for sore throat
The main problem when diagnosing a sore throat is not to miss the dangerous diagnoses of diphtheria and GABHS sore throat. To do this, a throat swab is taken from the child for bacterial and culture tests, including Albert's stain for diphtheria. A provisional diagnosis of diphtheria is suggested if the smear shows typical drumstick organisms. However, definitive diagnosis requires confirmation of C. diphtherium growth in culture.
To diagnose GABHS sore throat, there are antigen rapid tests. Their action is based on the extraction of group A carbohydrate antigen from throat swab materials with nitrous acid. These rapid tests are very specific (>95%) and provide immediate results, but have variable sensitivity. Confirmation of a positive result is not required, and if negative, a culture is recommended to exclude an infection dangerous to the child. Streptococcal antibody titers are not useful for diagnosing streptococcal pharyngitis and are not generally recommended.
Other studies:
- General blood analysis
- Peripheral blood smears - for the presence of atypical lymphocytes.
- Serology of Epstein-Barr virus (IgM antibodies)
- X-ray of the soft tissues of the neck (lateral view) if a retropharyngeal abscess is suspected.
- CT scan of the neck, including the base of the skull, to look for an abscess.
How does a sore throat appear?
Tonsillitis most often has a bacterial nature: the causative agent of the disease is bacteria such as staphylococcus, streptococcus and adenoviruses. Two thirds of all diseases are caused by β-hemolytic streptococcus. But this bacterium has an unpleasant property: it secretes a special enzyme and becomes invulnerable to cells of the immune system (phagocytes), which normally absorb harmful bacteria, thereby destroying them. What should a child’s body do in this case? Nature has found a way out: the body begins to intensively produce antibodies that successfully cope with foreign microorganisms. But the problem is that these antibodies begin to mistake the body’s own cells for “enemies.” And this is already fraught with the development of serious complications. Therefore, sore throat is considered to be an insidious disease: incorrect or late treatment of the disease in children or its complete absence can lead to serious consequences.
There are a number of reasons that contribute to the development of the disease. These include:
- weak immunity;
- the presence of chronic inflammation in the tonsils;
- the presence of infection in the ENT organs (sinusitis, otitis media);
- adenoids, a deformed nasal septum, polypous formations - all this interferes with normal nasal breathing and contributes to the development of inflammation;
- source of infection in the oral cavity (for example, carious teeth).
It is worth noting that sore throat is a highly contagious disease. To get sick, it is enough to share the same household items with the sick person. In the case of children - only toys. Therefore, it is not surprising that if one child in a kindergarten or school gets sick, the majority will get sick.
Treatment for a child with a sore throat
Prescriptions must be made by a doctor based on the established diagnosis and the identified or suspected pathogen. Self-prescription of medications by parents is unacceptable. This can lead to serious consequences for the child's health.
Farnigitis caused by GABHS infection is a disease that goes away on its own. However, treatment with antibiotics in this case provides rapid relief of symptoms, prevents purulent (otitis media, sinusitis, tonsillitis) and non-purulent complications, and also reduces the possibility of transmission of infection. Antibiotics reduce the incidence of rheumatic fever by more than two-thirds.
Clinical features, epidemiological criteria, and the judgment of an experienced clinician, with or without additional testing, usually indicate the need for antibiotics. The currently used pharyngitis decision score was adapted by adding age to the four components of the original Centor score (no cough, no swollen and tender anterior cervical nodes, temperature >38°C, tonsil plaque or swelling. Each component is given 1 point. age from 3 to 14 years is also given 1 point. Children or adolescents with a score of 0 or 1 do not need antibiotic therapy. Patients with a score of 2 or 3 points should undergo microbiological diagnosis of the pathogen and receive antibiotics if the results are positive. Children with A score of 4 or higher is at high risk for streptococcal GABHS pharyngitis and should receive antibiotic therapy.
Due to cost, narrow spectrum of action, safety and effectiveness, penicillin is the drug of choice. A shorter duration of treatment increases the risk of bacteriological relapse of the disease. The unjustified use of macrolides for the treatment of GABHS pharyngitis has become the main reason for the formation of resistant strains of pathogens.
Fever due to ARVI and influenza
Fever is a temporary increase in body temperature due to some illness. Fever is one of the symptoms of ARVI and influenza.
High temperature is the body’s protective reaction to a pathogen that has entered the body. Many viruses and bacteria stop reproducing at temperatures above 37-38°C, and the formation of antibodies is also stimulated.
There are “pink” and “white” fever.
For pink fever:
- heat production and heat transfer mechanisms are adjusted correctly
- baby's skin is pink and hot to the touch
For white fever:
- centralization of blood circulation (blood circulation is aimed at preserving the functioning of the heart, lungs, brain) and disruption of blood microcirculation
- limbs are cold, pale
- bluish leather with marble pattern
- "goose pimples"
- chills
Such a course of fever may be unfavorable.3
What are the complications?
Complications after an illness can be quite serious. The most common complication is rheumatism. This means that the pathogen has penetrated the heart and joints. To avoid cardiac rheumatism - myocarditis, and sometimes bacterial endocarditis, it is necessary to minimize the child’s physical activity during the illness.
Another common complication is kidney dysfunction and inflammation - glomerulonephritis.
By moving towards the brain, the pathogen can provoke inflammation of its membrane - meningitis. This disease is extremely difficult to treat, and its consequences for the child’s body are irreparable. If the disease is not treated, there is a high probability of death.
The occurrence of parathonsillar and parapharyngeal abscess, chronic tonsillitis, adenoids, hypertrophy (enlargement) of the palatine tonsils, otitis media, conductive hearing loss is only an incomplete list of the consequences of improper or delayed treatment of tonsillitis.
Types of sore throats
The mildest form of the disease is catarrhal. It is characterized by a slight increase in temperature, pain and dryness in the throat. With proper treatment, the illness lasts from three to five days. The disease can be easily confused with ARVI. Therefore, it is important to see a doctor to confirm the diagnosis - because treatment regimens for these two diseases differ.
Follicular tonsillitis is characterized by a more severe course. The body temperature rises to 38°C, the lymph nodes are greatly enlarged, and painful sensations appear when pressing on them. There are noticeable pustules on the tonsils, similar to white-yellow bumps, which burst within three to five days, after which significant relief occurs. The illness lasts about a week.
Another type of sore throat, very common in children, is lacunar. On the surface of the tonsils there are winding canals - lacunae. It is in them that bacteria and viruses often hide. With this type of disease, purulent masses fill the gaps, and a white coating becomes noticeable on the surface of the tonsils. The disease is quite difficult.
The signs of fibrous tonsillitis are very similar to those of follicular and lacunar tonsillitis. But a white film appears on the tonsils, which is why the disease can be confused with diphtheria. To make a correct diagnosis, it is necessary to take a smear from the surface of the tonsils.
Sometimes the disease is caused by a herpes virus. This type of sore throat is called herpes. It occurs with high fever up to 40°C, nausea, vomiting, and diarrhea. There are noticeable reddish blisters on the tonsils.
Fungal tonsillitis in childhood is rare. A characteristic symptom for it is the appearance of a cheesy coating on the tonsils.
The mixed form of the disease is especially difficult when the causative agents are several types of microorganisms. Mixed type tonsillitis can cause serious complications.