Impression taking technique
Custom impression trays are created by a podiatrist in the dental office. The impressions obtained after the functional test are clearly aligned with the prosthetic fields. The product is pre-fitted.
Correction of the frenulum of the tongue, cheeks and lower lip is performed. Recesses are formed along the edges of the product. Depending on the location and size, the tubercles on the mucous membrane are closed completely or partially.
It is necessary to block the false mylohyoid lines and preserve the function of saliva drainage by Wharton's ducts.
During the manufacturing process of prosthetic products for edentulous jaws, potential changes in the structure of the gums are taken into account. To achieve reliable stabilization and fixation of orthopedic structures, it is necessary to obtain a clear image of the relief of the mucous membrane of the prosthetic bed. When making a dental tray for patients with edentia, the functional state of the soft tissues of the prosthetic field is taken into account.
When creating a prosthesis for toothless jaws, the tray is used as the base layer of the impression. Using corrective material of low viscosity, the doctor reliably recreates the relief of the mucous membrane.
Herbst tests are ineffective in cases of severe atrophy of the alveolar process. This is due to the fact that the methodology is standardized.
The material used to mark the boundaries of the print is plaster or silicone. Some dentists prefer silicone due to its plasticity.
The art of taking impressions
High-quality impressions form the basis for successful prosthetic restorations. However, the variety of materials and methods for obtaining them provokes confusion, which can negatively affect the success of dental treatment. In this article we will look at the impression as a unique form of art, analyze the characteristics of the most commonly used materials, indications for their use and techniques of use that allow us to achieve the proper quality of the negative image of the tissues of the prosthetic bed.
Despite the fact that scanners represent an excellent alternative to classic impressions, the latter continue to be frequently used in everyday dental practice. According to a recent survey, it was found that about 76% of dentists prefer to use a scanner rather than taking a physical impression, but only 48% of dentists actually use a scanner in all practical cases where there is a choice between one and a classic impression . In essence, an adequate impression is a detailed representation of the tissues of the oral cavity. It allows you to accurately copy the boundaries of the preparation and soft tissues, and the tooth stumps themselves in relation to other structures of the dentofacial apparatus. The quality of the impression directly affects the further accuracy of the fit of the orthopedic structure. However, obtaining them is sometimes complicated due to the gag reflex and the patient’s feeling of subjective discomfort. The correct choice of material and technique for obtaining an impression largely determines the ability to bypass all potential limitations during manipulation.
Evolution of impression materials
Impression materials were first introduced around the 1700s when Philipp Pfaff proposed the use of softened wax. Later, doctors began to use other materials. The main disadvantage of wax was that it became too distorted during removal from the mouth. Different types of gypsum and zinc-oxide-eugenol materials, on the contrary, were characterized by a deficiency of elastic properties. The development of hydrocolloid materials, agar and alginate (photo 1-2) has made it possible to obtain much greater precision with lower resistance to destruction.
Photo 1. Alginate impression.
Photo 2. Alginate impression material.
The only drawback was the loss of dimensional stability over a certain period of time. In order to improve the fracture resistance, a new type of material was introduced into practice - polysulfide, which, however, was also characterized by a decreasing pattern of dimensional stability. These materials were also quite difficult to mix and had a specific unpleasant odor. In the 1960s, the first attempt was made to bring polyesters to market, and in the 1970s, type A and C silicones were introduced. The chemical composition of these materials made it possible to almost completely solve the problem of dimensional stability and low tensile strength. But they are also imperfect, since there is still no material that would be suitable for absolutely all clinical situations. Dentists use impressions for one purpose - to obtain an exact replica of the hard and soft tissues of the prosthetic bed. Improved material properties make it possible to recreate a given replica with a higher level of accuracy.
Characteristics of impression materials
Hydrophilicity
Hydrophilicity, in essence, demonstrates the nature of the interaction of the impression with water, as well as how it reacts to its presence in the oral cavity. This characteristic significantly influences the final accuracy of the impression regarding the detailing of the structures of the prosthetic bed. Hydrophilic materials are characterized by a high “level of affinity” with moisture and provide a high level of tissue detail due to their high surface wetting properties. Hydrophobic materials, on the contrary, demonstrate a low level of interaction with moisture, therefore, they are characterized by poor wetting properties, which makes it difficult to achieve high detail. Hydroactive materials provide a combination of both hydrophobic and hydrophilic characteristics. They are hydrophobic in nature, but the addition of surfactants can increase their level of hydrophilicity. This type of hybrid materials has significantly improved capabilities for detailing the structures of the prosthetic bed, due to its unique surface wettability.
Elasticity and tensile strength
Elasticity and tensile strength demonstrate the nature of changes in the impression material when it is removed from the oral cavity. Ideally, the elasticity of a material should allow it to stretch and then return to its original shape. If the stretch of the print goes beyond the limits of its elasticity, then it is clear that it cannot return to its original shape. Similarly, tensile strength demonstrates the ability of a material to return to its original shape without tearing. The magnitude of this parameter is influenced by several factors, including gingival retraction, depth of the subgingival margin, intensity of bleeding, the presence of sharp edges on the surface of the prepared tooth, as well as preparation designs that increase the level of resistance when removing the impression from the oral cavity. Understanding these material characteristics is imperative to prevent the need for a repeat impression procedure. In addition, it is important to choose a material for work that can be properly disinfected, because the protocols for this procedure are also material-specific.
Viscosity
Viscosity characterizes the fluidity of a material that has not yet hardened. Viscosity classifications include low (eg, syringe-injected materials), medium (eg, single-stage monophasic or heavy body), high (eg, impression tray material), and very high (eg, putty-type material). Viscosity directly depends on the amount of filler in the structure of the material. In this case, viscosity directly affects the ability to fully detail the condition of the tissues of the prosthetic bed. Essentially speaking, the lower the viscosity of the material, the greater the chance of getting a detailed impression, but at the same time, the shrinkage of the material during its polymerization also increases significantly. It is much more difficult to work with low-viscosity materials than with high-viscosity materials. Depending on how accurate the doctor needs to achieve the impression, he can use different types of materials.
Working time and curing time
Working time and setting time characterize the amount of time required to mix the material and place it in the spoon, as well as the time required for the material to completely harden in the oral cavity. Working time depends on the number of material components used, the use of manual or automatic mixing methods and the viscosity of the material. Manufacturers provide the clinician with a huge selection of impression materials with different working time characteristics. The temperature parameter affects both the working time and the curing time. We should also not forget that the working time of the material also depends on the direct recommendations of the manufacturer, and on the manipulation skills of the assistant or the dentist himself.
Dimensional stability
Dimensional stability is a parameter that directly affects whether the dental laboratory receives accurate and stable impressions, or whether the structure of such impressions does change during short-term storage. Ideally, the resulting impression can be stored for a sufficiently long period of time without affecting the ability to obtain several plaster models from it. The dimensional stability indicator depends on the influence of temperature, moisture absorption and the level of reduction in spatial volume as a result of polymerization.
Material selection
Preprints
Preliminary impressions are not characterized by the need for high detail of the tissues of the prosthetic bed; therefore, less expensive materials such as hydrocolloids, alginates or polysulfates can be used to obtain them. However, the use of these materials should be avoided when obtaining final impressions. Firstly, hydrocolloids are 80% water. They are extremely delicate and have low tensile strength. Polysulfates, in turn, are characterized by low dimensional stability, which, however, is sufficient for treatment planning. It is important to understand that although preliminary impressions do not involve super-details, they must be accurate enough for further planning of a complex of dental procedures. Typically, these impressions are used to analyze occlusion, the shape of the dental arch, the occlusal plane, and aesthetic relationships. Polyvinylsiloxane materials are ideal for obtaining optimal diagnostic impressions. They are characterized by fairly high dimensional stability, therefore, eliminating the need for immediate casting of the model. Before taking an impression, you should thoroughly dry your teeth and be sure that there is enough material to record all surfaces of the teeth, including the area behind the free gingival margin (photo 3-4).
Photo 3. View of the full print.
Photo 4. Impression of a quadrant of the jaw.
Final prints
Polyesters are the optimal material of choice for final prints. They are hydrophilic, characterized by long dimensional stability and short curing time. In addition, the level of deformation of polyesters during removal from the oral cavity is minimal, and the tensile strength is sufficient to eliminate the possibility of permanent deformation. The disadvantage of polyesters is their rigidity, unpleasant taste and smell, and the ability to absorb moisture from the atmosphere and swell over time. In addition, polyester impressions are quite difficult to remove from the oral cavity. Vinyl siloxanes remain another optimal choice for final print materials. The latter are less harsh than ethers, have a neutral taste and odor, and do not absorb excessive amounts of moisture. Vinylsiloxane prints can be used to produce multiple models at once and have high accuracy, excellent elasticity, improved dimensional stability and sufficient tensile strength. The hydrophilicity of polyvinylsiloxanes is increased by adding surfactants to their structure. The disadvantage of these materials is a decrease in the polymerization pattern in the presence of latex contamination. There are also hybrid materials that combine polyvinylsiloxanes and polyesters - vinyl-polyesters. Hybrid materials are characterized by high tensile strength and increased dimensional stability parameters. The polyester component of the hybrids ensures their hydrophilic nature without the need to add surfactants, and the silicone component increases dimensional stability and elasticity parameters. Like some silicones, hybrid materials have a pleasant taste and odor, unlike polyesters (photo 5).
Photo 5. Full impression made using polyvinylsiloxane.
Impression technique
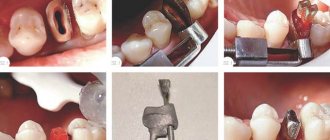
Photos 6-7 show a step-by-step protocol for obtaining impressions. Methods for obtaining impressions using the retraction technique are described below.
Photo 6. Algorithm for obtaining impressions from the upper jaw.
Photo 7. Algorithm for obtaining impressions from the lower jaw.
Retraction methods
It is important to recognize that retraction and hemostasis essentially have two different goals. Of course, sometimes both of them can be achieved through the same manipulation. Retraction is the temporary movement of gum tissue away from the surface of the tooth to expose the subgingival margin and create a space into which the impression material must be placed. Retraction can be carried out even before tooth preparation begins. In this case, it allows better visualization of the preparation margin area, which minimizes the risk of iatrogenic damage to the gums in the cervical area, and thus does not compromise the level of periodontal support of the tooth. There are four main retraction methods available today. The choice among them should be based on the doctor’s familiarity with the technique, localization, quality and condition of the soft tissues, as well as the complexity of the clinical situation as a whole.
Thread technique
The retraction suture packing technique is one of the most popular retraction methods, which is performed using twisted, knitted, woven or braided suture. To make them, different types of fibers are used, including wool, cotton and silk. These threads are available in two versions: impregnated with a hemostatic agent or not impregnated. When packing filament, it is important to understand the required size. Ideally, it is best to use the smallest suture size possible, as this will minimize the risk of gum injury, bleeding, or rupture of the sulcular epithelium. Typically, the sutures are packaged after preparation and removed immediately before the impression is taken.
Single thread technique. The technique of packing one retraction cord allows you to “push back” the soft tissue and create the necessary space in the area of the supragingival edge of the preparation. Although this manipulation is somewhat uncomfortable, it allows one to visualize the required boundary of enamel and dentin reduction, as well as to recreate the conditions for penetration of the impression material into this area. Typically, the packaged filament remains in the groove until the impression begins. The tip of the packer (the instrument used to pack the thread) must be thin enough so as not to damage surrounding tissue or cause bleeding (photo 8). The correct inclination of the packer working head allows you to optimize the thread packing procedure.
Photo 8. Packaging of retraction thread.
Two thread technique. This approach is similar to that described above, but another one is packaged on top of the initially installed thread. In this way, it is possible to achieve greater retraction of the mucosa and recreate the required volume of free space. Packing two threads at once allows you to create conditions for detailing the area of the gingival margin. However, when performing this procedure, the patient may complain of a certain feeling of discomfort.
Gum retraction technique using paste
The paste gum retraction technique is designed to minimize pain and discomfort during the procedure. When placed in the sulcus, the paste provides soft tissue displacement, thereby increasing the visualization of the preparation margin (Figure 9). The chemical composition of the paste also provides a hemostasis function, and this method can be used as an alternative to single suture retraction.
Photo 9. Retraction using paste.
Treatment of soft tissues using laser
Using a laser, surgical retraction of soft tissue can be achieved. This approach is safer than using a device for electrosurgical interventions, since the active agent is high-intensity radiation instead of electric current. Delivery of the laser beam to the intervention area is ensured using thin glass fiber or optical fiber (photo 10). Lasers cause shallow cellular necrotic burns in tissue adjacent to the epithelial layer, so healing is faster and more predictable. Although lasers can also cause burns to dentin, cementum, and attached soft tissue, the risk of such burns is minimal. The laser can also be used completely safely for patients with pacemakers, or in cases of concurrent general anesthesia with a mixture of gases. Depending on the type and wavelength of the laser, they may or may not be helpful in assisting hemostasis. The use of lasers is especially recommended in cases where the gingival margin is too deep, or when there is heavy bleeding in the intervention area.
Photo 10. Treatment of soft tissues using a laser.
conclusions
An ideal impression allows you to accurately copy all the structural features of the tissues of the prosthetic bed, while ensuring proper dimensional stability and the possibility of further obtaining several plaster models from it at once. Over the past 250 years, improvements in dental technology have enabled dental professionals to obtain highly accurate impressions through fairly simple manipulative approaches without compromising patient comfort during such procedures. The success of taking an impression depends on a careful evaluation of the original clinical restoration, the type of restoration planned, and the technique the clinician plans to use to accurately record the condition of the tissues of the prosthetic bed.
Author: Shannon Pace Brinker, CDA, CDD
Impression from the lower jaw
There are six stages of creating a functional impression:
- Setting the workpiece to LF. The visitor closes his mouth and swallows the accumulated secretion. The muscles that compress the pharynx contract. When the spoon is dropped, distal shortening occurs.
- The person presses his tongue on his cheeks one by one. After dropping, the workpiece is shortened along internal oblique lines.
- The patient reaches his tongue to the corners of his mouth. The product is cut in zones 3, 4 and from the mouth.
- A man sticks out his tongue and reaches for the tip of his nose. Then he runs his tongue along his upper lip. The chin muscles become tense. The displaced tray is shortened near the front teeth on the intraoral side.
- The patient strains the pterygomaxillary muscles with the mouth wide open. Distal shortening.
- The cheeks are retracted, and as the position of the spoon changes, shortening is performed near 6, 7 and 8 units. As a result of tension in the mental muscles, the device is reset and created in the corresponding area.
Taking impressions to make a diagnostic model for 1 jaw
Taking impressions is necessary at the initial stage of orthodontic or orthopedic treatment, when an examination is necessary before treatment to correct malocclusion, or it is necessary to make a model or several models for the correct manufacture of a crown or orthopedic structure.
Some doctors like to work with a specific impression material, highlighting its properties as the main and most suitable. Let's look at it in order.
Sign up online
Wax impressions.
They are made at a certain stage, after taking impressions with hardening plaster. While the plaster hardens, another wax impression is taken in the patient's mouth and placed on the hardened plaster model. This is convenient because it can be corrected, corrected and modeled right there on the model. Next will be embedding and casting the model.
Taking an impression of teeth with alginate mass
Alginate impression mass is a very durable and high-precision material. An impression of this mass will represent a reverse imprint of the mucous membrane of the oral cavity and teeth. In order to make such an impression you will need a special spoon.
Such an impression is made to make a plaster model, which later serves as the basis for the manufacture of prostheses. Impressions with this material can be made functional and anatomical, made with a standard spoon without taking into account the functional mobility of the tissues of the oral cavity.
Functional impressions are made with a custom tray using various jaw movements and functional tests. Fingerprints can also be main and auxiliary.
Taking impressions with silicone-A
Silicones-A consist of two pastes of the same consistency and different colors based on polyvinylsiloxane. This is a material of either high viscosity or low. High viscosity material is produced in a plastic jar, low viscosity material is produced in a container with a dispensing gun. Silicone-A is used in all types of dental treatment.
This silicone has advantages and disadvantages. Advantages: high hardness, no irritation of the mucous membrane, silicone can withstand disinfection in any solution, reproduces oral tissues down to the smallest details, is resistant to deformation and tearing, tasteless and odorless, several models can be cast from the print within 30 days after receiving it .
Disadvantages: has insignificant shrinkage, high cost, it is necessary to work in a thoroughly dried oral cavity, since silicones are hydrophobic, a special substance must be used to improve adhesion to the impression tray (adhesive), contact with latex dentist gloves can inhibit the polymerization of the material.
Taking an impression with silicone-S
Silicones-S are available in several forms: paste, gel in tubes using tetraethyl silicate (cross-linking agent). This impression material (gel) is pre-mixed with precise dosage of components. After mixing, a polycondensation reaction begins, resulting in the formation of silicone rubber and the release of ethyl alcohol with increasing temperature.
A two-layer impression is obtained by combining two impression compounds of different degrees of viscosity. This is done for a more accurate imprint of the subgingival part of the tooth crown. It is obtained in one step using one-step or sandwich techniques.
Zinc oxide eugenol impression materials have high fluidity in the initial phase and quite clearly display the smallest details of the prosthetic bed. The disadvantage is that when removing it from the oral cavity, the material may crumble and deform. It is difficult to clean off the skin and instruments.
And some components of the material (eugenol or clove oil) can cause irritation of the patient's mucous membranes.
Sign up online
Taking impressions with polyester mass is a fairly promising group of impression materials containing various polyesters, plasticizers and inert fillers. Among the advantages: hydrophilicity, small linear shrinkage, good fluidity, display accuracy.
Impression from the upper jaw
The specialist’s algorithm of actions includes 4 stages:
- The mouth opens wide and the spoon is placed on the high frequency. The displaced product is shortened behind the modular tubercle.
- Cheeks retract. The device is shed by the buccal cords, and its dimensions decrease near the sixth, seventh and eighth teeth.
- The upper lip is pulled down and forward. When the location changes, the device is shortened by about 3, 4 and 5 teeth.
- Pulling the lips forward with a long tube. Shortening is performed around 12 dental units.
The test is considered completed if there are no displacements. Fitting should be done carefully to prevent significant reductions in the basis boundaries.
Evaluating the results of the HF fitting allows the specialist to create an impression tray of the ideal shape. After adjusting the listed parameters, the dentist begins to form an impression.
Materials and features of the procedure
To obtain high-quality dental impressions, the preferred option is to combine materials with different viscosity parameters. The high-viscosity formulation provides sufficient rigidity, while fine-grained correction materials improve imaging accuracy. Standard protocols also provide for the possibility of three-phase (the number of phases means the number of compounds) impression taking, with the addition of medium-viscosity material.
One of the elements provided by the technology for obtaining dental impressions is an impression tray. From a technical point of view, this is a design that is mass-produced or made individually, the structure of which repeats the anatomical structure of the jaw and looks like a horseshoe.
To obtain two-phase impressions, a one- or two-step approach is used. In the first case, an individual tray is used for simultaneous application of both compositions, while the corrective mass can also be applied to the surface of the tissue area of the prosthetic bed - followed by indentation of the element. The two-stage method differs in the number of placements of the spoon in the oral cavity - in the second case, the instrument is used twice, first with the base material and then with the corrective material. Practice shows that such an approach provides an accurate result, but leaves the possibility of making a technical error, which is practically impossible to identify before manufacturing a replacement structure.