A healthy oral cavity is a factor that has a positive impact on a person’s overall well-being and psychological state. Performing hygiene procedures is an accessible method of preventing various diseases, thanks to which you can prevent negative consequences for teeth and gums, as well as maintain the aesthetic appeal of your smile. As part of a clinical examination, dental indices are used to assess the condition of the oral cavity, which indicate the degree of development of identified pathologies.
The formula will help determine the condition of the mouth
To determine the condition of the oral cavity in medicine, there are about 80 different hygiene indices, based on the principle of staining the enamel with a special solution and identifying dental plaque.
According to the parameters they define, indices can be classified into 4 groups, assessing:
- area affected by plaque;
- thickness of plaque on teeth;
- mass of plaque;
- other parameters of dental plaque (chemical, physical and microbiological).
Assessing the condition of the gums using clinical methods
The periodontal index allows you to assess the health of the gums and bone tissue of the alveoli. It is placed on each tooth separately. Special indicators are used: for gum pathological processes they are relatively low, for pathologies of the tooth alveoli - vice versa. The data for an individual tooth is added together. Then the number must be divided by how many teeth there are in the mouth. The data obtained allow us to talk about the course of periodontal diseases. Causes of diseases and types are not taken into account.
Periodontal index
CPU in dentistry
Dentists should use these calculations during the initial examination of the patient. So, for example, the average values of the indices KPU, kp. KPU+KP of teeth and cavities in dentistry allows you to determine the intensity of carious lesions. These abbreviations contain the following meanings:
- K – carious permanent teeth;
- P – permanent teeth in which a filling is installed;
- U – extracted molars;
- j – temporary teeth affected by caries;
- p – filled temporary teeth.
- According to the World Health Organization, the average CP index for children 12 years old should be from 2.7 to 4.4, and for citizens aged 35-44 years 6.3-12.7.
Assessment of plaque deposits in young children
Characteristics are given to absolutely all children's teeth. The procedure can be done from the moment the first teeth appear up to three years. You can make an assessment “by eye” or using tools.
Even if there are few teeth in the baby's mouth, an analysis should be carried out.
Criteria:
- 0 – no plaque;
- 1 – there is plaque.
Assessment of plaque deposits in young children
Simplified index (IGR-U)
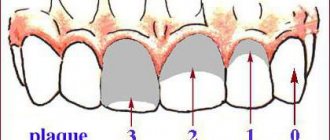
The Green Vermillion Hygiene Index measures plaque and tartar on the surfaces of the 2 upper first molars, 2 lower first molars and 2 upper incisors.
Ratings are given as follows:
- 0 – no plaque;
- 1 – no more than 1/3 of the tooth surface is covered with plaque;
- 2 – plaque affects from 1/3 to 2/3 of the tooth;
- 3 – dental plaque covers more than 2/3 of the surface.
The simplified hygienic index is calculated by adding the plaque index and tartar index on 6 teeth.
General overview
The index is a collection of data obtained during the survey process. As part of the diagnosis, the doctor evaluates the contamination of the enamel surface, determines the presence of pathological bacteria and the volume of tartar deposits, and also identifies the ratio of healthy and caries-affected units. The results that form the indications of the clinical picture are used to determine the cause of diseases, and make it possible to determine the appropriate method of treatment and prevention.
Dental indices include assessment of:
- Oral health conditions;
- The stage of destruction to which individual elements have been subjected;
- The need to remove units that cannot be restored;
- Degree of thoroughness of dental cleaning;
- Development of the bite and correct position of the teeth;
- Results of prescribed therapy.
Depending on the specifics of the lesion, different sets of specialized data are used for analysis.
PMA – papillary-alveolar-marginal index
When calculating the PMA index, a solution of iodine or Lugol is used, which is applied to the gums and the degree of tissue inflammation is determined by the reaction to the irritant.
The evaluation criteria are:
- 1 – if the papilla (P) is inflamed;
- 2 – in case of inflammation of the marginal edge (M);
- 3 – inflammation of the alveolar part of the gum (A).
Formula RMA = Sum of points/n*3 (in percentage), where n is the number of teeth (up to 6 years – 20 teeth; 6–12 years – 24 teeth; 12-14 years – 28 teeth; over 15 years – 30 teeth) .
If the value is less than 30%, then the degree of damage is mild, 31-60% is moderate, 61% or more is severe.
Iodine index of enamel remineralization.
The active permeability of iodine in tooth tissue is known. Remineralization index (RI), which characterizes the effectiveness of the remineralization therapy used. It is assessed using a four-point system:
1 point – no staining of the tooth area;
2 points - light yellow coloration of the tooth area;
3 points - light brown or yellow staining of the tooth area;
4 points - dark brown staining of the tooth area.
The calculation is carried out according to the formula:
IR = IRNP x number of teeth with hypersensitivity / n,
where IR is the remineralization index;
RRI—remineralization index of one non-carious lesion;
n is the number of teeth being examined.
Dark brown and light brown staining indicates demineralization of the tooth area with non-carious lesions; light yellow - indicates a certain level of remineralization processes in this area of the tooth, and the absence of staining or its slightly yellow color demonstrates a good level of the remineralization process of a particular non-carious tooth lesion.
Php Index
Scientists Podszadlej and Haley developed an oral hygiene performance index. First, a dye solution is applied to the teeth, then the patient rinses his mouth with water, and 6 teeth are examined. In this case, their surface is divided into 5 sections: medial, distal, mid-occlusal, central, mid-cervical. The absence of staining is determined by zero, and the presence - by one.
When calculating, use the formula: IG = ZN/n, where ZN is the sum of codes for all teeth; n – number of teeth examined. With a value of 0, the condition of the oral cavity is considered excellent, and with a value of 1.7 or more, it is considered unsatisfactory.
Fedorov-Volodkina hygienic index
To assess a person’s independent oral hygiene, they use this index. It is best suited for children under six years of age. To calculate the index, the surface of six teeth from the lips is examined. A special composition paints the enamel, allowing plaque to be found. The probe allows you to detect stone formations of various types. To calculate the index, you need to add up all the resulting numbers and divide by the number of surfaces examined. Then they are folded.
Fedorov-Volodkina hygienic index
CPITN (periodontal disease treatment need index)
This method covers 10 teeth, allowing the dentist to see the condition of the gums of the upper and lower jaws. Grades are given as follows:
- 0 – no disease symptoms;
- 1 – gums are bleeding;
- 2 – tartar was found above and below the gum;
- 3 – gum pocket 4-5 mm deep;
- 4 – gum pocket more than 6 mm.
It may come as a surprise to many that the condition of teeth can be determined using a formula, but this is the truth. Therefore, do not neglect maintaining oral hygiene, so as not to be a poor student in this calculation.
The iOrtho clinic network provides high-quality services for correcting malocclusion with Invisalign aligners, sign up for a consultation now!
Indices used in dental examination
The prevalence of caries is expressed as a percentage. To do this, the number of people who were found to have certain manifestations of dental caries (except for focal demineralization) is divided by the total number of people examined in this group and multiplied by 100.
In order to assess the prevalence of dental caries in a particular region or compare the value of this indicator in different regions, the following assessment criteria for the level of prevalence among 12-year-old children are used:
Intensity level
LOW - 0-30% MEDIUM - 31 - 80% HIGH - 81 - 100%
To assess the intensity of dental caries, the following indices are used:
a) intensity of caries of temporary (baby) teeth: index kp (z) - the sum of teeth affected by untreated caries and filled in one individual;
index kp (n) - the sum of surfaces affected by untreated caries and filled in one individual;
In order to calculate the average value of the indices kp(z) and kp(p) in a group of subjects, one should determine the index for each person examined, add up all the values and divide the resulting amount by the number of people in the group.
b) intensity of caries of permanent teeth:
index KPU(z) - the sum of carious, filled and extracted teeth in one individual;
index KPU (n) - the sum of all surfaces of the teeth on which caries or a filling is diagnosed in one individual. (If a tooth is removed, then in this index it is considered 5 surfaces).
When determining these indices, early forms of dental caries in the form of white and pigmented spots are not taken into account. In order to calculate the average value of indices for a group, you should find the sum of individual indices and divide it by the number of people examined in this group.
c) assessment of the intensity of dental caries among the population. To compare the intensity of dental caries between different regions or countries, the average values of the KPU index are used.
WHO distinguishes 5 levels of intensity of dental caries:
Periodontal indices. CPITN Index
To assess the prevalence and intensity of periodontal diseases, almost all countries use the index of need for the treatment of periodontal diseases - CPITN . This index was proposed by specialists of the WHO working group to assess the condition of periodontal tissues during epidemiological surveys of the population. Currently, the scope of the index has expanded, and it is used to plan and evaluate the effectiveness of prevention programs, as well as calculate the required number of dental personnel. In addition, the CPITN index is currently used in clinical practice to examine and monitor the periodontal condition of individual patients. In this regard, the CPITN index can be considered a screening test at both the population and individual levels. This index registers only those clinical signs that may undergo reverse development: inflammatory changes in the gums, which are judged by bleeding, tartar. The index does not record irreversible changes (gingival recession, tooth mobility, loss of epithelial attachment), does not indicate the activity of the process and cannot be used to plan specific clinical treatment in patients with developed periodontitis. The main advantages of the CPITN index are the simplicity and speed of its determination, information content and the ability to compare results. To determine the CPITN index, the dentition is conventionally divided into 6 parts (sextants), including the following teeth: 17/14 13/23 24/27 34/37 43/33 47/44.
The periodontium is examined in each sextant, and for epidemiological purposes only in the area of the so-called “index” teeth. When using the index for clinical practice, the periodontium is examined in the area of all teeth and the most severe lesion is identified. It should be remembered that a sextant is examined if it contains two or more teeth that cannot be removed. If only one tooth remains in the sextant, it is included in the adjacent sextant, and this sextant is excluded from the examination. In the adult population, starting from 20 years of age and older, 10 index teeth are examined, which are identified as the most informative: 17/16 11 26/27 47/46 31 36/37.
When examining each pair of molars, only one code characterizing the worst condition is taken into account and recorded. For persons under 20 years of age, 6 index teeth are examined during an epidemiological survey: 16, 11, 26, 36, 31, 46
CODE 1 : bleeding observed during or after probing. Note: bleeding may appear immediately or after 10-30 seconds. after probing. CODE 2 : tartar or other plaque-retaining factors (overhanging edges of fillings, etc.) are visible or felt during probing. CODE 3 : pathological pocket 4 or 5 mm (the edge of the gum is in the black area of the probe or the 3.5 mm mark is hidden). CODE 4 : pathological pocket 6 mm deep or more (with the 5.5 mm mark or black area of the probe hidden in the pocket). CODE X : When only one or no teeth are present in the sextant (third molars are excluded unless they are in place of second molars).
To determine the need for periodontal disease treatment, population groups or individual patients can be categorized based on the following criteria. 0: CODE 0 (healthy) or X (excluded) for all 6 sextants means that there is no need for treatment for this patient. 1: A CODE of 1 or higher indicates that this patient needs to improve his oral hygiene status. 2: a) CODE 2 or higher indicates the need for professional hygiene and the elimination of factors that contribute to plaque retention. In addition, the patient needs training in oral hygiene. b) CODE 3 indicates the need for oral hygiene and curettage, which usually reduces inflammation and reduces pocket depth to values equal to or less than 3 mm. 3: Sextant with CODE 4 can sometimes be successfully treated with deep curettage and adequate oral hygiene. In other cases, this treatment does not help, and then complex treatment is required, which includes deep curettage. The prevalence and intensity of periodontal disease in the population is assessed based on the results of a survey of 15-year-old adolescents.
Gingivitis Index (GIA)
To assess the severity of gingivitis (and subsequently record the dynamics of the process), the papillary-marginal-alveolar index (PMA) . Various modifications of this index have been proposed, but in practice the PMA index as modified by Parma (1960) is more often used.
The RMA index is assessed using the following codes and criteria:
0—no inflammation; 1 - inflammation of only the gingival papilla (P); 2 - inflammation of the marginal gum (M); 3 - inflammation of the alveolar gum (A).
The PMA index is calculated using the formula: sum of PMA = ———————- x 100% 3 x number of teeth The number of teeth (while maintaining the integrity of the dentition) is taken into account depending on age: 6 – 11 years – 24 teeth, 12 – 14 years - 28 teeth, 15 years and older - 30 teeth.
Note: if there are missing teeth, then divide by the number of teeth present in the oral cavity. Normally, the PMA index is 0. The higher the digital value of the index, the higher the intensity of gingivitis.
Evaluation criteria for the RMA index:
30% or less - mild gingivitis; 31-60% - moderate severity; 61% and above—severe degree.
Oral hygiene assessment
Fedorov-Volodkina hygienic index (1971)
The index is recommended to be used to assess the hygienic state of the oral cavity in children under 5-6 years of age. To determine the index, the labial surface of six teeth is examined: 43, 42, 41, 31, 32, 33. These teeth are stained using special solutions (Schiller-Pisarev, fuchsin, erythrosine) and the presence of plaque is assessed using the following codes: 1 - plaque not identified; 2 - staining one quarter of the surface of the tooth crown; 3 - staining half the surface of the tooth crown; 4 - staining three quarters of the surface of the tooth crown; 5 - staining the entire surface of the tooth crown. Determination of supra- and subgingival tartar is carried out using a dental probe.
Codes and criteria for assessing dental calculus
O —tartar is not detected; 1 - supragingival tartar, covering no more than 1/3 of the tooth surface; 2 - supragingival tartar, covering more than 1/3, but less than 2/3 of the tooth surface, or the presence of individual deposits of subgingival tartar in the cervical area of the tooth; 3 - supragingival calculus covering more than 2/3 of the tooth surface, or significant deposits of subgingival calculus around the cervical area of the tooth.
The calculation of the index consists of the values obtained for each component of the index, divided by the number of surfaces surveyed, followed by the summation of both values.
Formula for calculation:
IGR-U stone values = ———————————- + ——————————— quantity. number of surfaces surfaces
Evaluation criteria
a) IGR-U values: Level of oral hygiene 0, 0 - 1, 2 good 1, 3 - 3, 0 satisfactory 3, 1 - 6, 0 poor
b) Values of plaque or tartar indicators: 0.0 - 0.6 good 0.7 - 1.8 satisfactory 1.9 - 3.0 bad
Oral Hygiene Performance Index (OHP) Podshadley, Haley, (1968)
To quantitatively assess dental plaque, 6 teeth are stained: 16, 26, 11, 31—vestibular surfaces; 36, 46 - lingual surfaces.
1 - medial 2 - distal 3 - mid-cervical 4 - central 5 - mid-occlusal
Codes and criteria for assessing dental plaque
O - no staining 1 - staining detected
The index is calculated by determining the code for each tooth by adding the codes for each section. Then the codes for all examined teeth are summed up and the resulting sum is divided by the number of teeth:
The index is calculated using the following formula:
sum of codes of all teeth RNR = —————————————————— number of teeth examined
Evaluation criteria
Index value Hygiene level 0 excellent 0.1 - 0.6 good 0.7 - 1.6 satisfactory 1.7 or more unsatisfactory
Dental aesthetic index NC Cons et al., (1986)
A special dental aesthetic index is used to assess the condition of the bite. In the clinic, the index is used at the individual level and when conducting epidemiological surveys of the population. This index determines the position of the teeth and the state of the bite in the sagittal, vertical and transversal directions. Recommended for use from 12 years of age in key age groups. The examination is carried out visually and using a button probe. The index includes the definition of the following components: • lack of teeth; • crowding in the incisal segments; • gap in the incisal segments; • diastema; • deviations in the anterior part of the upper jaw; • deviations in the anterior region of the lower jaw; • anterior maxillary overlap; • anterior mandibular overlap; • vertical front gap; • anteroposterior relationship of molars. Lack of teeth. The number of incisors, canines and premolars on the upper and lower jaws is counted (from 15 to 25 and from 35 to 45) and the number of missing teeth in this group is determined.
Teeth are not considered removed if: 1. with a missing tooth, the space is closed; 2. the baby tooth is in the dentition, but the permanent tooth has not yet erupted; 3. The space is restored with a bridge. Crowding in the incisal segments. Each segment consists of 4 incisors. Crowding is a condition of the dental arches when the space between the right and left canines is not enough to accommodate all 4 incisors in a normal position. The teeth may be rotated or out of line with the arch.
Codes and evaluation criteria
O - no crowding 1 - crowding of one segment 2 - crowding of two segments
Spacing in incisal segments. Gap is a condition where the space located between the right and left canine teeth is greater than the space required to accommodate all 4 incisors in their normal position. If one of the incisors has proximal surfaces without interproximal contact, the segment is considered to have a spacing. If the bite is mixed, you should not consider the space from a recently fallen temporary tooth to be empty if it is obvious that the permanent tooth will erupt soon.
Codes and criteria:
O - no gap in segment 1 - one segment with a gap 2 - two segments with a gap. If in doubt, evaluate to a lower score. Diastema is the space between the two permanent upper central incisors. Measurements are taken with a button probe at any level between the mesial surfaces of the teeth and expressed in mm.
The largest deviation between adjacent teeth is measured. To do this, the tip of a button probe is placed on the labial surface of the tooth most deviated in the lingual direction or rotated around its axis at an angle of 90° to the normal line of the dental arch. Registered in mm. Anterior maxillary overlap. The measurement is carried out in central occlusion. The working part of the periodontal probe is placed parallel to the occlusal plane and the distance (in mm) from the labial-incisal edge of the most protruding upper incisor in relation to the labial surface of the lower incisor projected onto it is assessed. This index component is not taken into account if all the upper incisors are missing and/or in a lingual position (crossbite). If the incisors close to the edge, then you can put code 0. Anterior mandibular overlap. This sign is assessed when either lower incisor is advanced anteriorly or vestibular to the opposing upper incisor. The greatest forward movement of the tooth (in mm) is recorded. Measurements are carried out in the same way as on the upper jaw.
If there is no occlusion on the first molars due to the absence of one or two teeth, incomplete eruption or disruption of their shape due to caries or filling, then the relationship of the canines or premolars is determined.
Codes and criteria:
O - norm 1 - displacement by 1/2 of the tuberosity mesially or distally in relation to the norm 2 - displacement by the size of the tuberosity mesially or distally in relation to the norm.
The dental aesthetic index allows you to analyze each of the components of the index or group them by anomalies of the dentition and bite.
Classification and types of CPU
The amount of damage to teeth by the carious process is expressed by the KPU index. This abbreviation stands for:
- K – total number of teeth with caries;
- P – number of sealed elements;
- Y is the number of units removed.
The sum of these three indicators determines the dynamics and speed of the carious phenomenon.
There are 3 types of CPU:
- teeth (otherwise KPUz) – the number of filled and carious units in a person;
- all surfaces (or KPUps) – the number of dental surfaces infected with caries;
- cavities (i.e. KPUpol) – the number of carious and filled cavities.
For milk units, other decodings are used:
- KPz – the number of treated and carious elements;
- Kppov – number of affected dental surfaces;
- Kppol – number of fillings and cavities.
In children, elements in the primary occlusion that are removed or lost during physiological changes are not taken into account.
They use 2 types of indices simultaneously: KPU and KP. To determine the intensity of the pathology, both of these indicators are summed up.
If the CPU is within the limit:
- from 6 to 10 – the speed and intensity of caries is high;
- 3-5 – moderate;
- up to 2 – low.
These indicators do not reveal an objective picture of the state of oral health, since they have the following negative aspects:
- Simultaneously treated and removed units are taken into account.
- Show the past picture of the disease and increase with a person’s age.
- The initial stage of the pathological process is not taken into account.
A serious drawback is also considered to be the unreliability of the indices when problem elements increase due to the appearance of new cavities in the treated units, the loss of old fillings, and the development of secondary caries.
The prevalence of the pathological process is expressed as a percentage. A certain number of individuals with different manifestations of the disease (with the exception of focal demineralization) is taken, divided by the total number examined in this group, and multiplied by 100.
When comparing the prevalence of the disease by region, a scheme is used based on the assessment criteria of the multiplicity of cases among 11-13 year old children:
| Index | Level |
| no more than 30% | isolated |
| up to 80% | average |
| over 80% | high |
To find out the dynamics and speed of caries, dentists rely on the following indices:
- KPU (P) – surfaces sealed and affected by pathology;
- KPU (Z) – elements sealed and affected by disease.
To track this process in adult patients, slightly different criteria are used:
- KPU (P) – treated and carious surfaces;
- KPU (Z) – cured, carious and removed elements.
Important! When calculating the result, carious lesions that look like pigment spots are not taken into account.
To calculate the average for a group, it is necessary to determine the total value of individual indicators and divide them by the number of people surveyed.
How effective is teeth whitening varnish, judging by reviews from experts and users.
Read here about how to quickly whiten your teeth at home.
At this address https://www.vash-dentist.ru/krasota-i-uxod/otbelivanie/maslo-chaynogo-dereva-dlya-domashnego-zubov.html you will find out whether there is any harm from the method of teeth whitening with tea tree oil.
WHO survey
Epidemiology is a special branch of medicine that studies the nature of the manifestation and spread of pathologies among various segments of the population. It is also applicable in dentistry.
Epidemiological research takes place in 3 stages:
- Preparatory. Planning is done for upcoming research, defining objectives, methods and research dates.
The place of execution and the necessary equipment for this are being prepared. A group of junior medical staff and trained doctors is being created.Population groups differing from each other in living conditions are identified, with an equal number of men and women.
- Examination. A registration card is created in which the research data will be entered (for children and adolescents under 15 years of age its form is simplified).
It is prohibited to make corrections or additions to this document. All entries are recorded in coding, with each code indicating a specific symptom or its absence.To obtain an accurate picture of health, information about the extraoral zone and mucous membrane is also taken.
- Evaluation of the results obtained. Data is calculated - the degree of prevalence of caries, the threshold for the incidence of periodontitis, etc. The result is displayed as a percentage.
Such an examination helps to analyze the dental situation in a certain region, find out the dependence of oral health on social class or environmental living conditions, and track the degree of change in these data with a person’s age.
It is important to determine the most common diseases, their intensity by region and age. Based on the results obtained, preventive actions are developed and hygiene training is provided.
The video provides additional information on the topic of the article.