630
It is believed that fixed functional orthodontic appliances are not effective enough to treat people with a mature dental system.
Doctors often recommend that such patients resort to maxillofacial surgery to correct dental anomalies.
However, recently developed orthodontic devices can, in many cases, eliminate the need for invasive and expensive bone grafting. Such devices include the Forsus device.
General presentation and purpose
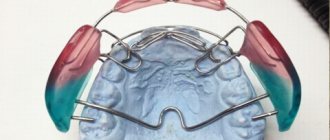
The Forsus device is a non-removable orthodontic device of a functional-mechanical type. This means that the corrective force is created in it both by a constantly operating mechanical device (spring) and by the work of the masticatory muscles.
The device is intended for the correction of distal occlusion (class 2 anomaly), which is characterized by retraction of the lower jaw relative to the upper jaw.
The orthodontic system assembled using the Forsus apparatus consists of the following elements:
- upper buccal tubes (right and left);
- maxillary arch with braces;
- mandibular arch with braces;
- EZ module;
- mandibular rod.
The corrective action of the device consists of stimulating growth (moving forward) of the lower jaw through the pressure of the mandibular rod on the mandibular vestibular arch.
At the same time the growth of the upper jaw is inhibited , thanks to the reactive force from the spring transmitted to the buccal tube, through it to the arch and all the teeth of the upper jaw.
The design can be supplemented with other elements, in particular, ligatures, which have the desired effect on individual teeth.
For what purpose is the bite height determined and the methods used.
Come here to review techniques for determining centric occlusion and centric relation of the jaws.
At this address https://www.vash-dentist.ru/ortodontiya/prikus/mehanizm-stanovleniya-molochnogo.html we will talk about the features of the period of change in the primary occlusion.
General overview
Forsus is a non-removable orthodontic device of functional-mechanical action, designed to correct distal occlusion in adolescence.
Forsus consists of 2 identical parts - left and right. The main effect of the device is to move the bass forward and simultaneously slow down the development of the high frequency.
The device is made of medical steel and is intermaxillary in type (connected to both jaws). The device works in conjunction with mandibular and maxillary braces, which complement some of its actions.
Forsus is not noticeable in the mouth. It has a compact size, making it easy to get used to and the absence of any significant discomfort. Irritation of the buccal mucosa from the device is minimized.
One of the main advantages of Forsus is the ability to avoid surgical correction of the distal bite. But this advantage is realized only if the correction is carried out at the age of 10-16 years - during the period when the bones of the maxillofacial area are still in the stage of formation and development.
The Forsus device can also be used in adults. But, as a rule, in combination with surgical methods, since the jaw of an adult is fully formed and is difficult to undergo purely orthodontic correction.
Advantages of using the Hyrex device for maxillary expansion.
Come here if you are interested in the design of the McNamara apparatus.
At this address https://orto-info.ru/sistemyi-vyiravnivaniya-zubov/lechebno-profilakticheskie-apparatyi/plastinka-hintsa.html we will consider the characteristics of a Hintz plate with an inclined plane.
Specifications
The Forsus device is a universal system that can be adjusted to the jaw of any adult. Its main parameters are the pressure force on the lower vestibular arch and the distance from the edge of the buccal tube to the surface of the bracket installed on the lower canine (that is, the length of the intermaxillary traction).
The pressure of the rod on the arc should be about 200 g. It is regulated using stoppers installed on the mandibular rod to change the degree of compression of the spring.
The length of the intermaxillary rod varies depending on the size of the jaw and is established by selecting a rod of the required length, as well as by installing stoppers on the lower vestibular arch.
All structural elements are made of durable material with high fatigue strength.
Purpose of individual system elements
- Spring assembly. Consists of three telescopic springs that provide the necessary correction force. The consistency of its action makes the treatment independent of the patient’s behavior, with the mouth open and closed.
- Clip . It is used to attach the EZ module to the buccal tube. Thanks to a special design (presence of an anti-rotation shoulder), the clip prevents the occurrence of torque on the buccal tubes, which prevents rotation of the abutment tooth and increases the comfort of wearing the device.
- Buccal tube. It is the base (support) against which correction is carried out.
It consists of a ring put on a tooth (molar or premolar) and 2 soldered tubes. The upper one is used to attach the maxillary facebow, the lower one, located at the level of the occlusal surface, is for attaching the EZ module clip. The length of the down tube ranges from 3.6 to 4.3 mm. - EZ module .
This is the main element of the system. It is a prefabricated unit that includes a spring unit and a clip, the elements are connected to each other by a lever. According to their function, the EZ module is an intermaxillary rod that transmits force from a compressed spring to the lower vestibular arch. This creates a constant correction force independent of the patient. - Mandibular rod .
Transfers force from the spring to the lower vestibular arch. Available in five sizes - 25, 29, 32, 35 and 38 mm. The connection of the rod to the arc is carried out using a loop located at its end. The latter is thrown onto the arc and compressed with pliers to prevent it from falling off. - Inferior vestibular arch . Receives pressure from the mandibular rod and transmits it to the teeth of the lower jaw, through glued braces. The force is directed forward to advance the lower jaw.
- Superior vestibular arch . Connects the teeth of the upper jaw into a single supporting system. Receives reactive correction force and transmits it to the upper jaw, inhibiting its development.
Control of support in cases with removal
A common Class-II treatment problem is the extraction of posterior teeth in patients with a posteriorly recessed mandible. Protrusion of the mandibular incisors or lack of space for the lateral units cause their extraction. Moving the lateral teeth of the lower jaw forward without disturbing the position of the incisors is a difficult task.
Another problem is the position of the maxillary molars after the socket in the gum is closed. Their unwanted movement, as well as the expansion of the periodontal groove of the mandibular incisors, is fraught with expansion of the sagittal fissure. Identified problems become an obstacle to bite correction.
Using the Forsus device allows you to control the position of the mandibular incisors, hold in place or distalize the maxillary molars at the stage of closing spaces. The treatment protocol for problems requiring maxillary arch augmentation, removal and control of the maxillary support now includes the use of the Forsus appliance.
Indications and contraindications
The Forsus appliance is used to correct moderate class II anomalies (distal occlusion).
In particular, the following clinical cases are indications for its use.
- The need for skeletal correction in mild and borderline distal occlusion. (Reference: Skeletal correction, unlike dentoalveolar correction, involves influencing the entire jaw bone, and not just the dentoalveolar process).
- Dentoalveolar anomaly class 2.
- Unilateral class 2 anomaly (distal bite + displacement of the midline of the lower jaw). In this case, different correction forces are set for different sides of the jaw. The result of treatment is the correction of the distal bite with simultaneous correction of the position of the midline.
The Forsus device is contraindicated if there is a risk of negative changes in facial aesthetics.
Reasons for distalization of lower molars and features of the device.
In this publication, read how orthodontic tooth traction is performed.
Here https://www.vash-dentist.ru/ortodontiya/prikus/deprogrammator-koysa.html all the most important things about using the Koysa deprogrammer in dentistry.
Rules and terms of wearing
In addition to more thorough oral hygiene during treatment, the patient is required to periodically visit the doctor according to the schedule established by him. Although rare, the device must be activated - approximately once every 6-8 weeks.
If the facial midline is displaced, unilateral activation can be performed. The optimal corrective force is considered to be 200 g.
Various sources indicate different average duration of wearing Forsus - from 2 to 5 months. This may be explained by differences in treatment-related factors.
The duration of correction is influenced by the type and severity of the anomaly, the individual characteristics of the patient’s dental apparatus, the condition of his bone tissue, etc.
In general, for the treatment of distal occlusion, the average duration of treatment can be considered 4-5 months. By this time, several months of using the device as a retainer may be added.
The first results of treatment can be seen 3-4 weeks after installing Forsus.
In the video, watch how the Forsus device works.
Fixation stages
Installation of the device, if it is used at the very beginning of treatment, begins with fixation of buccal tubes on the second molars of the upper jaw.
The maxillary and mandibular arch with braces are installed using standard technology - the adhesive method. The ends of the mandibular arch should be curved after the outermost brackets (installed on the second molars). For reliability, you need to attach the arches to the locks not with elastic, but with wire ligatures.
After fixing the arches, begin installing the EZ module. Using Weingard forceps or another instrument, insert the module clip from the mesial side into the lower tube until it clicks.
Using a special tool in the form of a ruler, measure the distance from the rear edge of the tube to the distal surface of the bracket installed on the canine. If a stopper installed on the arch is used as a support for the mandibular rod, then the distance to it is measured.
When measuring, the lower jaw should be in its natural position (without moving forward). Based on the measurement results, a mandibular rod of suitable length is selected.
The loop of the selected rod is placed on the lower vestibular arch in the intervals between the first premolar and the canine. The point of application of the rod can be changed using a stopper installed on the vestibular arch (the stopper serves to stop the rod and is installed at the point where it is necessary to apply force).
When the patient's mouth is open, the module spring is compressed and a rod is inserted into it. If it is discovered that when the teeth are closed, the rod comes out from the far edge of the spring, you need to use a smaller standard size.
The final manipulation is to compress the rod loop with pliers to prevent it from falling off the arc.
The device is activated (if necessary) by installing a locking ring on the rod in front of the spring (to do this, it must be compressed). The correction step is 2-3 mm.
Watch the video to see how the Forsus device is installed and operates.
Using the Forsus device to control support during extraction
One of the most common clinical situations that arise during the treatment of class II anomalies is the need for extraction - or removal of premolars - in the presence of mandibular retrognathia. As a rule, indications for the procedure are insufficient free space, as well as protrusion of individual units.
Shifting the lateral areas without correcting the position of the teeth is a difficult task; In addition, the problem is the need to ensure the safety of the upper antagonists during the period of closing the gaps formed after the removal of elements of the series. Mesialization of the maxillary molars and retraction of the lower anterior units can lead to an increase in the sagittal gap, and ultimately negatively affect the results of correction. The use of the Forsus orthodontic corrector provides a sufficient level of control over the position of the elements of both rows, holding them in the correct position, or distalizing them in the intermediate closure phase, and allowing you to adhere to a given treatment protocol.
Duration of wearing
The duration of treatment varies widely, depending on the severity of the abnormality. The device can be used not from the beginning of treatment, but at some stage (installation of the EZ module on a previously installed brace system).
It is also possible to remove the module before the end of treatment, and continue correction with braces without it. In general, the duration of treatment can range from 1 month to 2 years.
Control inspections of the system are recommended at least once every 6 weeks.
Use of the Forsus™ device for Class II correction: taking into account patient comfort.
We have found that patients accept the Forsus™ device well during the initial consultation. Very often, parents experience relief after learning that the device works automatically, regardless of the degree of patient cooperation. They also liked the fact that although the device is not a monolithic structure, it is quite durable. As an orthodontist, I appreciate the predictability of the machine, which allows me to accurately time my treatment.
The convenience of this appliance may be due to what we call the “first premolar connection.” Using this fixation technique, we almost completely eliminate the possibility of developing irritation of the mucous membrane of the cheek or lips in the commissure area. For this type of placement, we fix the rod distal to the first lower premolars. Clinically, this technique does not significantly affect the vertical and horizontal components of force. The figures below show that when the appliance is secured to both the canines and the first premolars, the forces are developed in the correct direction for a Class II correction.
We use elastic ligatures with a protective pad (3M Unitek 406-429). Placed under the archwire on the first premolar brackets and fused distally, the ligature with a protective pad acts as a shock absorber. Once the ligatures are placed, a 0.019” x 0.025” steel archwire is placed and curved downward distal to the molars. After this, the premolar bracket is tied with a metal ligature. The safety pad relieves excess stress on the premolar bracket, protecting it from the sliding rod and reducing the risk of debonding (Figure 3-4).
To achieve the desired level of activation, it is sometimes necessary to modify the rod when placing it distal to the first premolar. Most often this occurs when treating patients with a small lower jaw, as well as with a pronounced posterior position of the lower jaw.
The modification involves grinding down the stopper on the rod using abrasive discs. This allows the spring to be distributed throughout the rod before it bends. The rod must then be shortened so that it does not protrude beyond the spring when it is compressed and active. (Fig. 5-6)
In addition to patient comfort, an additional benefit of the “first premolar connection” is improved control of the position of the mandibular incisors. Undesirable protrusive position of the incisors can be reduced by including the first premolars in the anterior abutment block. This is especially true for patients with severe mandibular retrognathia, when it is necessary to minimize the movement of the lower incisors and move the lower jaw forward as much as possible. In the case presented below, incisor angulation was maintained during the Class II correction phase. The patient wore a Forsus™ appliance placed distal to the first mandibular premolars for 5 months. The total duration of her treatment was 24 months (Fig. 7-12).
Advantages and disadvantages
The main advantage of the Forsus apparatus is its effectiveness in correcting distal occlusion in people with a mature dental system.
In addition, a number of advantages are due to the design features of the device.
- Predictability of the result, thanks to the efficiency of the system and the elimination of the human factor. The adjustment does not require patient participation. The constant action of the corrective force is ensured by the presence of a spring.
- Easy to install. The EZ module attaches to the buccal tube with one click. This became possible thanks to the special design of the clip. The mandibular rod is also easily attached to the vestibular arch. The loop is thrown onto the arc and compressed with pliers to prevent it from jumping off the arc.
- Easy to use , does not require long-term staff training.
- Compatible with any braces ; it is possible to simultaneously use rigid and elastic ligatures to move an individual tooth in the desired direction.
- High adaptability , adaptability to different jaws. The magnitude, application point and direction vector of the corrective force can be easily changed.
- Structural strength. Breakdowns cannot be completely ruled out, but the device is quite reliable.
- Comfortable to wear. In most cases, patients do not complain of discomfort. This is ensured by the design of the device itself. The close location of the spring and the rod to the teeth, as a rule, relieves the cheek mucosa from irritation.
- Practical invisibility.
Flaws:
- volumetric design , in rare cases, due to the structural features of the jaws, irritation of the mucous membranes by the spring and rod is possible;
- relatively low degree of correction for skeletal (jaw) anomalies (dental-alveolar movement occurs more easily).
Lisa Alvetro, Ph.D.
Dr. Lisa Alvetro received her MD from The Ohio State University in Australia.
She has been in successful practice in Sidney, Ohio for 13 years, committed to incorporating the latest innovations in orthodontics. Dr. Alvetro currently teaches a practicum course at Case Western Reserve University. Like many orthodontists, we are faced with increasingly busy and challenging lives for our patients. They require excellent treatment results in the shortest possible time and the best price/quality ratio. The parents of our patients want the treatment of their children to be as comfortable and convenient as possible. Based on these requirements, we decided to include the Forsus™ device in most cases of treatment during the planning stage.
There was a time in my practice when fixed Class II corrective appliances were used only after unsatisfactory treatment results with devices that required patient cooperation. Now, treatment planning using the Forsus™ device initially provides the benefits of treatment with a fixed device that does not require patient cooperation. The design of the device makes it easy to install and also provides reliability for a variety of use cases.
The treatment protocol for cases requiring Class II correction, maxillary distalization to increase arch length, and cases requiring extraction and support control in the maxilla now includes the Forsus™ appliance. Every orthodontist recognizes that one of his most valuable assets is the time spent seeing patients (chair time).
Longer treatment means more patient visits. Thus, this approach also improves productivity: the most productive and cost-effective way to use the Forsus™ device is to include it in the treatment plan at the initial stage. If you wait until you recognize the patient's lack of cooperation, you will lose valuable chairside time and prolong the patient's treatment time.
Reviews
The Forsus device has been used in orthodontics relatively recently. If you had to undergo treatment with its help, share your impressions about it.
Was a positive result achieved, how long did it take? The comment form is at the bottom of the page.
If you find an error, please select a piece of text and press Ctrl+Enter.
Tags devices: bite correction
Did you like the article? stay tuned
Previous article
The use of aesthetic abutments in dental practice
Next article
Is it possible to do dental implantation without a sinus lift?
Author: Dr. Neal D. Kravitz
Dr. Neal D. Kravitz is a board certified member of the American Board of Orthodontics and a clinical research faculty member at the University of Maryland and Washington Hospital Center. Dr. Kravitz received his undergraduate education from Columbia University and his DMD from the University of Pennsylvania.
Dr. Kravitz has published in many orthodontic journals, books, and educational pamphlets. He lectures throughout the country and internationally on the topic of modern advanced orthodontics and treatment planning. Dr. Kravitz currently owns two orthodontic practices in South Riding, Virginia and White Plains, Maryland. Dr. Kravitz is one of the leaders in promoting the Incognito system.
Effective non-extraction Class II correction is part of running a successful orthodontic practice. While there are many different traditional appliances available for vestibular techniques to reduce the sagittal gap, it seems that in aesthetic orthodontics there is a limited choice, especially with removable aligners.
This article is devoted to an overview of the treatment of class II pathology without excision using the Forsus device in conjunction with the Incognito system. Several different techniques will be covered, including a combination of lingual treatment in the upper jaw with vestibular technique in the lower jaw, together with laboratory-fabricated rings, and lingual treatment with double arches with traditional rings.
The Incognito system offers fully customized, digitally designed and manufactured lingual brackets and archwires for effective and accurately predictable discreet orthodontic treatment (Figure 1 AC).
Fig 1 AC. Manufacturing of the Incognito system. Setup models are scanned to digitally create custom braces. Braces are made of gold alloy.
The Forsus appliance is a spring-loaded, permanent Class II corrector fixed to the facebow tube of the maxillary first molar and to the labial arch of the mandible, resulting in rapid dentoalveolar compensation (Fig. 2).
Figure 2. The Forsus appliance operates similarly to the Herbst appliance, resulting in rapid distalization of the maxillary molars and deflection of the mandibular incisors.
A patient aged 31 years with pathology in class II, subclass 1, moderate crowding in the upper jaw with rotation of the incisors and edentulous second left premolar in the lower jaw. The treatment plan included class II correction using the non-cooperative Forsus device. Even in cooperative patients with class II and canine displacement of more than 50%, simply wearing elastics may not be sufficient. Combined treatment (lingual and vestibular technique) with laboratory-made rings.
In the Incognito order, we informed the technician that saddle rings would be made for the upper first and second molars. First molar rings were made with buccal facebow tubes to secure the Forsus appliance. The order also stated that good fixation of the ring on the first molar should be ensured by extending its length to the gingival margin (Fig. 3A-C). It is recommended to use saddle rings on second molars to facilitate insertion of the arch, open the bite and reduce the risk of detachment.
Figure 3A-C: Digital creation of saddle rings with a facebow tube for fixation of the Forsus device. Strengthening the fixation was required by lengthening the ring platform to the gingival margin. Occlusal photo immediately after indirect bonding of the Incognito system from the second premolar to the second premolar and direct bonding of rings to the molars followed by installation of a .014 NiTi archwire. The Forsus unit was not installed until the spaces on the .016×.024 steel arch were consolidated.
After initial alignment and leveling, .016×.022 steel archwires were installed on the upper and lower jaws. Bracket ligation when installing steel ligatures may seem difficult on a lingual system, so the practitioner may use a single or double chain. The period for correction of most class II pathologies with the Forsus device is approximately 6 months. (Figure 4A-I, 5A-J, 6)
Figure 4A-I: (Same patient as Figure 3). Combined system: Incognito on the upper jaw, vestibular ceramic braces with the Forsus apparatus on the lower jaw (second row). Installation of the Forsus device. Note the facebow tubes into which the Forsus L-pin is inserted. The lower part of the device is curved vestibular for greater comfort. The teeth of the lower jaw are connected to enhance support and prevent unwanted opening of the teeth. After removal of the Forsus device, Class II elastics are used for stabilization. To improve the aesthetics of the smile, recontouring of the incisal edges was performed.
Fig. 5 AJ: Installation of the Forsus device in an adult patient with pathology in class II, subclass 2 with deep overlap. A .016×.024 steel arch was installed on the upper jaw, and .016×.022 on the lower jaw. The L-shaped pin of the Forsus apparatus was installed in the spring eye; The “ball” of the pin should be directed buccally. Using Weingart forceps, the pin was inserted into the facebow tube. The pin was curved towards the teeth for better fixation and comfort; This also helps prevent unwanted jumping out of the device’s springs. Please note: these photographs are provided as an example, but when you order the system, it is advisable to specify that the saddles be extended towards the gums to improve fixation.
Fig. 6. The upper dentition is prepared for the Forsus apparatus. A .016×.024 steel archwire is placed and bent distally behind the second molars. All spaces are closed and consolidated with a double elastic chain. If desired, a metal ligature can be used for this purpose.