- Types of products
- Ceramic inlay e max: main indications
- Contraindications for installing ceramic inlays
- Ceramic tooth inlay: advantages and disadvantages of products
- Manufacturing and installation stages
- Ceramic dental inlay: care features
If it is necessary to carry out extensive restoration, they often resort not to filling material, but to ceramic inlays (onlays).
They are one of the best methods of dental restoration and provide high-quality results. Ceramic inlays are a microprosthesis that is fixed in the tooth cavity. Such orthopedic structures are characterized by high aesthetics and durability; they are completely identical to healthy enamel, due to which they have become widespread. The e max ceramic inlay is in particular demand; it can be installed in a reliable dental clinic “A-medic”. The company's pricing policy is loyal, the cost of the service starts from 15,000 rubles. Before installing a microprosthesis, dentists conduct an examination and diagnosis to identify possible contraindications. In dentistry, a ceramic inlay is installed in just 2 stages, which allows you to quickly make your smile more attractive. An individual approach to each patient is guaranteed.
Types of products
Experts distinguish between two main types of orthopedic structures: stump and restorative. A ceramic core inlay is required to restore the tooth core for subsequent fixation of the crown. Most often it is used for prosthetics of incisors. Restorative structures are used for chewing teeth when one or two surfaces are damaged. In addition to high aesthetics, they are characterized by reliability and durability. Also, the tabs are distinguished by the material used. Below are the most common materials from which products are made.
- pressed ceramics. Products are produced using porcelain injection molding. The procedure is carried out under conditions of high temperature and pressure. Compared to orthopedic structures made of metal or zirconium dioxide, they are not as durable, but are ideal from an aesthetic point of view;
- zirconium dioxide. They are made by grinding finished metal oxide blanks. Grinding is carried out automatically using a ready-made impression (plaster model) of a damaged molar or premolar. Thanks to computer control, finished structures are characterized by high quality. Upon completion, the workpiece is fired, fusing the porcelain mass. Zirconium dioxide is a high-tech material for orthopedic structures, and therefore is in special demand. From an aesthetic point of view, such inlays are in no way inferior to porcelain products, and in terms of strength they are not inferior to metal products;
- metal. The metal most often used is gold or a silver-palladium alloy. Such designs are reliable, but do not have high aesthetics;
- metal ceramics. This is the latest orthopedic design, which is distinguished by high aesthetics, but at the same time cannot boast of proper quality. Due to thermal exposure, such products often fall out of the mouth. Most experts advise installing a structure made of zirconium dioxide or pressed ceramics rather than metal ceramics.
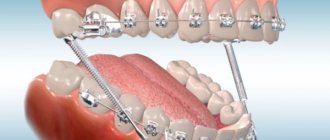
Anchor pins for tooth restoration
Anchor pins are often used to restore pulpless teeth. Anchor pins are metal pins that are fixed into a canal to build a tooth stump for a future crown or direct restoration.
They are threaded and fixed into the root canal using special cement. At one time they were very widely used in dentistry. However, they soon began to be abandoned, and we tried to figure out why.
Positive and negative properties of anchor pins
If we talk about the advantages of using anchor pins for restoration, they include:
- strength - such pins do not break
- affordable price
- speed and ease of use
What's wrong then? Let's look at all the shortcomings:
- low connection - there is no chemical connection between the intra-root and coronal parts, so they can easily separate
- poor aesthetics, especially if the work is done on the front teeth
- high risk of root fracture, since when installing an anchor pin, tension occurs inside the tooth root, which leads to a wedging effect, plus necrosis of the tissue around the tooth root, which leads to tooth extraction
The speed of installation of the anchor pin also plays an unpleasant role here. Fast does not mean easy. After all, each anchor pin system has its own installation rules and special auxiliary tools, which, unfortunately, are often neglected.
Ceramic inlay e max: main indications
Many people mistakenly believe that ceramic inlays are a type of regular filling. In fact, they belong to the category of high-tech microprostheses. Its parameters and characteristics significantly exceed any, even the most modern and high-quality filling material. Among the main indications for installing ceramic inlays are:
- destruction of the coronal part by 30% or more;
- preparing a molar or premolar for the installation of permanent orthopedic structures, for example, bridges;
- increased abrasion of enamel;
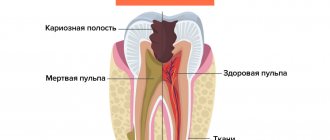
- the presence of a large cavity that was formed as a result of an advanced carious process;
- increased sensitivity of molars or premolars to external factors;
- mechanical damage.
If, after fixing the orthopedic structure, pronounced painful sensations occur, you should not delay your visit to the dentist. Most often, pain and discomfort are a sign that the product was installed incorrectly. To avoid such situations, treatment should be carried out only in trusted dental clinics.
Contraindications for installing ceramic inlays
The emax tab also has some contraindications for installation. There are no absolute contraindications, but there are relative and temporary ones, which are recommended to be eliminated before installing a ceramic onlay. Among them, insufficient oral hygiene is the most common contraindication. In this case, a specialist performs professional cleaning and prescribes additional oral care methods that can be done at home.
In case of carious lesions of the teeth, the dentist carries out treatment, and after it proceeds to install the structure. Experts do not recommend installing onlays on the last molars (“eights”). They do not perform a chewing function, so in case of severe destruction, the easiest way is to completely get rid of them without spending time on restoration.
It will not be possible to carry out the installation if only one wall of the tooth remains (at least two remaining walls are required). Problems can arise when the cavity depth is insignificant (less than 2 mm) or the presence of pathological cavities that go deep into the dentin. For bruxism (teeth grinding), the installation of pads is not recommended, since they will quickly wear out, which will significantly reduce the service life. However, you can use a special device (night guard) that will prevent the teeth of the lower jaw from rubbing against the teeth of the upper jaw.
Ceramic tooth inlay: advantages and disadvantages of products
Currently, ceramic onlays are the most common method of restoring incisors, molars or premolars; they are recognized as reliable and durable. Unlike composite fillings, they are not made in the patient’s mouth, but in isolation, in a dental laboratory (using impressions). This allows you to create an anatomically correct tooth shape with increased accuracy. This factor is very important for the area of contact with the adjacent incisor, molar or premolar. The use of ceramic inlays makes it possible not to resort to crowns if the root bases of the teeth are intact. The main advantages of the products include:
- high aesthetic qualities. Ceramic onlays are no different from natural molars or premolars. The material fully matches their visual characteristics. Only a specialist can notice the difference upon careful close examination;
- durability (compared to a conventional filling). If you follow all the recommendations prescribed by your doctor, the orthopedic design can last more than 10 years. For comparison, a regular filling lasts about 3-4 years;
- no changes in appearance. Ceramics do not darken over the course of a year, so the original color remains intact for the entire duration of wear. It is completely resistant to dyes and other external factors;
- no shrinkage and polymerization after fastening. The main factor influencing the development of secondary carious lesions is pathogenic microorganisms that enter the gap between dentin and filling material. It occurs as a result of shrinkage of the filling. Under the influence of ultraviolet radiation, the filling significantly decreases in volume and sags. e max structures retain their dimensions and do not change during the manufacturing and installation process. Their grinding occurs at the same time as the tooth tissues;
- complete safety. The material does not have a negative effect on the human body and does not provoke the development of allergic reactions;
- high strength. Unlike conventional fillings (light, chemical), the inlay is more securely fixed and is characterized by increased resistance to mechanical and thermal stress.
The emax ceramic inlay has no significant disadvantages. Some are confused by the time spent on manufacturing and installing orthopedic structures, which, unlike conventional fillings, require several visits to the dentist's office. Relative disadvantages include the high price (compared to inlays made of other metals). It is worth noting that their quality, aesthetics and long service life justify their relatively high cost.
Orthopedic treatment of tooth crown defects using inlays
For several decades, the search for optimal ways to replace defects in the crown of the tooth has been ongoing. The development of technology constantly tilts the scales, which tilts towards either therapeutic or orthopedic techniques. Our goal was not to conduct a comparative analysis of various methods for restoring crown defects. This publication is devoted only to illustrating certain recovery methods that, in our opinion, deserve attention.
The main method of eliminating defects in the crown of a tooth, especially in the initial and middle forms, is undoubtedly filling. Dental filling compared to prosthetics is a less labor-intensive process, which consists of surgical removal of the affected tissue, medicinal treatment of the cavity and filling the defect with filling material. However, this method of treatment, even at the modern level of development of dentistry, cannot always provide a solution to the problem of restoring the shape and function of teeth, especially with carious defects of classes II, IV of the Black classification, systemic hypoplasia, increased abrasion, hereditary disorders and malformations of hard tissues, etc.
The significant and most characteristic disadvantages of fillings include, first of all, secondary caries and loss of fillings (Abolmasov N. G. et al., 2003). M. B. Bushan and V. N. Kopeikin note that filling materials have a lower coefficient of wear resistance compared to metal and porcelain. They may be porous and not strong enough. Therefore, interest in alternative types of treatment and, in particular, in replacing tooth crown defects with inlays is quite justified.
Inlays are called microprostheses used to restore defects in the coronal part destroyed as a result of carious and non-carious lesions. Unlike a filling, the tab is inserted into the prepared cavity not in a plastic state, but in a solid state. This avoids shrinkage that occurs when the filling material hardens, and therefore improves the marginal fit and reduces the frequency of caries relapses.
The design of the inlay is selected taking into account the topography, shape, size of the defect, anatomical and topographic relationships of hard and soft tissues, type of bite, direction of loads, tooth inclination, radiographic results, presence or absence of pulp. Depending on the material from which the inlays are made, they are divided into: a) metal (gold 900, 750, cobalt-chrome alloy, silver-palladium alloy, titanium alloys, for example VT5L); b) non-metallic (porcelain, composite); c) combined metal-ceramic and metal-composite (Fig. 1).
Rice. 1a. Inlay made of 900-carat gold alloy.
Rice. 1b. Inlay made of 900-carat gold alloy.
For a number of years, the main structural material for inlays has been gold alloys. The method of manufacturing a cast inlay using a wax model was described by Taggart in 1907. Since then, the technology has undergone certain changes, but the high strength characteristics and accuracy of the fit of the gold inlays to the walls of the cavity, maintaining a constant volume, protecting the edges of the enamel from chipping, inertness, non-oxidation in the oral cavity, the ability to unravel during chewing and better adapt to the walls of the cavity.
In connection with the increasing requirements for the aesthetics of restorations and constantly improving technologies for the manufacture of dentures, one of the most promising areas is the prosthetics of partial defects in the coronal part of the tooth with ceramic inlays. The current level of development of dentistry makes it possible to produce these structures in the following ways:
- firing on foil;
- firing on a fireproof model;
- production of a ceramic frame by firing on a refractory model, followed by cladding;
- production of ceramic inlays by pressing;
- manufacturing a frame from aluminum oxide and zirconium dioxide by electrophoretic deposition with subsequent lining;
- manufacturing the inlay frame by ultrasonic condensation of aluminum oxide with the addition of zirconium dioxide, followed by layer-by-layer application and firing of porcelain;
- firing of the aluminum oxide frame followed by cladding;
- milling using a computer program.
The technology for manufacturing ceramic dentures by hot pressing is implemented using the IPS-Empress I, II systems. One of the advantages of these systems is the use of fluorapatite as a structural material, which, compared to other ceramic materials, causes less abrasion of natural antagonist teeth (Fig. 2).
Rice. 2a. Porcelain inlay made by pressing (painting technique).
Rice. 2b. Porcelain inlay made by pressing (painting technique).
Initially, the IPS-Empress I system provided for the complete reconstruction of the anatomical shape of the coronal part of the tooth from wax and the subsequent simultaneous hot pressing of the ceramic mass. Thus, the finished restoration was monochrome, with a high degree of transparency, since porcelain of the same color was used. Color correction was carried out by applying dyes before glazing, which did not always make it possible to optimize the color rendition of the restoration with the individual coloring characteristics of natural teeth (coloring technique).
Ivoclar specialists continued to work on this issue, which was reflected in their later developments. When working with the IPS-Empress II system, you can create a wax model of the base of the inlay with subsequent pressing. Subsequently, dentin and enamel masses are applied to the model on the frame, ceramics are modeled and fired (layer-by-layer porcelain application technique).
The manufacture of the inlay frame by ultrasonic condensation of aluminum oxide with the addition of zirconium dioxide, followed by layer-by-layer application and firing of porcelain involves the introduction of a suspension of the VITA In-Ceram ZIRCONYA material into the cavity of the double model of the prepared tooth, compacted in a Vita Sonic II type apparatus, drying, and correction of the shape of the inlay base , glass infiltration and firing. After trying on the base in the oral cavity, it is veneered with ceramic mass (Fig. 3).
Rice. 3a. Ceramic inlay made using ultrasonic condensation technology of VITA In-Ceram ZIRCONYA material, followed by firing and layer-by-layer application and firing of ceramics.
Rice. 3b. Ceramic inlay made using ultrasonic condensation technology of VITA In-Ceram ZIRCONYA material, followed by firing and layer-by-layer application and firing of ceramics.
Rice. 3c. Ceramic inlay made using ultrasonic condensation technology of VITA In-Ceram ZIRCONYA material, followed by firing and layer-by-layer application and firing of ceramics.
The most interesting direction may be related to milling a ceramic block using a computer program. Since the early 90s, zirconium oxide has been increasingly used in dentistry. According to in-vitro studies, zirconium oxide denture frames have high tensile strength comparable to that of metal alloys. The introduction of CAD/CAM technology in dental prosthetics makes it possible to produce structures with high accuracy and predictably reproducible quality. Based on the general user algorithm and hardware layout, CAD/CAM systems can be divided into 3 main groups:
- Centralized macrosystems (Procera, Decim).
- Individual mini-systems (Hint-Els, Precident).
- Custom microsystems (Cerec).
The use of modern computer technologies can significantly increase the accuracy of restoration manufacturing and minimize the influence of the human factor. However, most of the well-known CAD/CAM systems are expensive, which limits their distribution in the dental market. A number of inventors set out to create compact and inexpensive milling equipment that makes it possible to produce extended structures from zirconium oxide (Fig. 4).
Rice. 4a. Manufacturing of inlays using copy-milling technology and a zirkonzahn machine.
Rice. 4b. Manufacturing of inlays using copy-milling technology and a zirkonzahn machine.
Rice. 4c. Manufacturing of inlays using copy-milling technology and a zirkonzahn machine.
Rice. 4g. Manufacturing of inlays using copy-milling technology and a zirkonzahn machine.
One of them was Enrico Steger, inventor, owner and CEO of Zirkonzahn. The operation of his system is based on copy-milling technology. First, a prototype of the product is created from a light-curing composite material, then it is milled from a zirconium oxide blank in a copy-milling machine.
To facilitate this process and reduce wear on grinding tools, the Zirkonzahn machine works with an unsintered (pre-agglomerated) form of zirconium dioxide. The zirconium oxide inlay blank is 25% larger than the composite counterpart, since further firing of the product will lead to significant shrinkage of the material. The author managed to calculate these volumetric changes and transfer them with high accuracy into the basis of the operation of his copy-milling machine.
Along with the above-described methods for making inlays, restoration of defects in the coronal part of the tooth is also currently used using inlays made of light-curing composite materials. Compared to porcelain and metal-ceramic inlays, composite inlays have a less abrasive effect on natural teeth; due to the elasticity of the composite, they absorb part of the occlusal load, are less labor-intensive to manufacture and do not require expensive bulky equipment and specially trained dental technicians, and can be easily restored in the oral cavity. , much cheaper.
The disadvantages of composite inlays include insufficient color stability, the possibility of allergic reactions to the composite, and the abrasion of modern composite materials, although close to the abrasion of tooth enamel, is somewhat higher, which can lead over time to a decrease in the height of the lower third of the face in the position of central occlusion with multiple restoration of lateral teeth, with single restorations - to the development of deformation of the occlusal curves. Composite inlays have lower strength, greater porosity, and, compared to porcelain and metal ones, are characterized by less tolerance to the gingival margin, but despite this, they can be a serious alternative to direct restorations (Fig. 5).
Rice. 5a. Stages of tooth restoration using a composite inlay.
Rice. 5 B. Stages of tooth restoration using a composite inlay.
Rice. 5th century Stages of tooth restoration using a composite inlay.
Rice. 5g. Stages of tooth restoration using a composite inlay.
Rice. 5d. Stages of tooth restoration using a composite inlay.
Rice. 5e. Stages of tooth restoration using a composite inlay.
The development of dentistry at the present stage is characterized by the rapid growth of new technologies for the manufacture of dentures. And it’s quite difficult for a dentist to navigate this diversity. We hope that this publication expands the horizons of choosing restoration techniques for defects in the coronal part of the tooth.
LITERATURE
- Abolmasov N. G. Replacement of defects of teeth and dentition with fixed dentures N. G. Abolmasov, N. N. Abolmasov, V. A. Bychkov, V. R. Shashmurina. - Smolensk, 1995. - 175 p.
- Bragin E. A. Fundamentals of microprosthetics. Pin structures of dentures, inlays, veneers, artificial crowns, decorative dental onlays. / E. A. Bragin, A. V. Skryl. - M.: Medical press, 2009. - 508 p.: ill.
- Volvach S.I. CAD/CAM technologies in the dental laboratory - myth or reality? / S. I. Volvach // New in dentistry for dental technicians. - 2000, No. 4 (12). - P. 3-13.
- Dyakonenko E. E. Orthopedic treatment with metal-free ceramics as an alternative method of tooth restoration / E. E. Dyakonenko // New in dentistry for dental technicians. - 2000, No. 1 (9). - P. 3-14.
- Prosthetic restoration of teeth. CEREC system. Textbook, ed. prof. V. N. Trezubova, S. D. Arutyunova. - St. Petersburg: Spetslit, 2003. - 64 p.
- Skryl A.V. Restoration of defects in tooth crowns with ceramic inlays / A.V. Skryl // Modern orthopedic dentistry. - 2008, No. 10. - P. 46-48.
- Steger E. ZIRKON milling technology / E. Steger // Dental technician. - 2007, No. 4. - P. 33-41.
Manufacturing and installation stages
Manufacturing and installation of an orthopedic structure is not difficult and does not take much time. At the initial appointment, the dentist examines the oral cavity to determine indications and contraindications for the procedure. If contraindications are identified, they are eliminated, after which they proceed to therapy. If necessary, endodontic treatment and hygienic treatment of the diseased tooth are carried out. By analogy with standard filling, the specialist removes all destroyed tissue from the tooth, forming an area for a microprosthesis. After this, a cast is made that exactly repeats its shape.
The production time for an emax ceramic inlay based on the impression obtained (3D modeling results) is about 5-10 days. At this time, a temporary filling material is placed in the patient's cavity. The onlay is made in laboratory conditions, taking into account the individual characteristics of the patient’s dental system. The orthopedic structure is fired and covered with layers of ceramics. At the secondary appointment, the patient’s temporary filling is removed and a finished microprosthesis is installed. It is attached using special cement, which firmly adheres to the ceramics and enamel of the tooth. This guarantees a secure fit. At the end of the process, the surface is polished. The whole procedure takes no more than 120-150 minutes.
Ceramic dental inlay: care features
The ceramic inlay and onlay do not require complex care. You need to care for your teeth like you would for regular teeth - brush twice a day, use floss and mouth rinses after each meal. It is worth noting that ceramic inlays, due to their physical properties, do not require additional care (unlike light fillings) - professional cleaning.
In order to promptly detect leaks in the Emax tab, you need to regularly visit the dentist’s office (once every six months). When a dark stripe appears, there is a high probability that pathogenic microorganisms have begun to penetrate under the ceramic inlay, which provoke the development of a carious process. On average, the service life of ceramic structures is about 7-8 years. Subject to all rules and hygiene standards, as well as the absence of increased stress, they can last several years longer.
You can install a ceramic inlay in Moscow at the reliable A-Medic clinic. Qualified specialists with extensive experience work here, which guarantees a positive result. The orthopedic design is no different from natural teeth and can last for many years. In the event that there are contraindications to the installation of this product, A-Medic dentists will be able to select another method of tooth restoration.
Materials for manufacturing pin stump inlays
Stump pin inlays can be made from different materials - ceramics or metal. Stump inlays with metal pins are most often made from an alloy of cobalt and chromium and are used for the installation of metal or metal-ceramic prostheses.
Cobalt-chrome core inlays have a number of specific advantages:
- They have good biocompatibility with human body tissues;
- Stump pin inlays made of this metal alloy fit quite tightly to natural tissues and therefore, when used, the risks of caries, inflammatory processes and further tooth destruction are reduced;
- Cobalt-chrome alloy has high strength and therefore a crown installed on a pin insert made of this material will not shrink during operation.
Stump inlays made of cobalt-chrome alloy allow for proper distribution of the chewing load, which reduces the risk of cracks and tooth destruction. The advantages of inlays made from this material include their affordable cost.
Ceramic pin inlays are used for the installation of metal-free dentures. This allows you to obtain impeccable aesthetics of the restored tooth. If you place a metal stump insert under the ceramic structure, it can be quite noticeable and, of course, it will spoil the appearance of the restored tooth. Therefore, only ceramic pin inlays are placed under ceramics.