According to antiplagiat.ru, the uniqueness of the text as of October 16, 2018 is 90.3%.
Key words, tags: tooth extraction, wisdom tooth, bone tissue, implant installation, augmentation, implantation.
Despite the rapid development of modern dentistry, tooth extraction is still a very common operation. When a doctor removes a tooth, be it a dystopic wisdom tooth or a severely rotted molar, in its place there remains a hole, a cavity, which is called the alveolar socket. Previously, the affected tooth was simply removed, and the resulting cavity, the socket, healed on its own, with a significant decrease in bone tissue. But today, when talking about qualified dental care, we should talk about preserving the alveoli in its original state, even in the absence of a tooth.
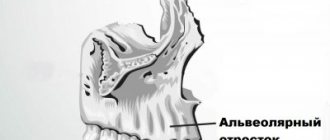
Anatomy of the alveolar process
The alveolar, or dental, process (from Latin - processus alveolaris) is the part of the upper and lower jaws that extends from their bodies and contains teeth. The development and normal functioning of this structure is ensured by the roots of the teeth located in it. The alveolar process appears only after teeth erupt and almost completely disappears with their loss. After a tooth is removed, the corresponding area undergoes resorption (resorption). Dental alveoli, or sockets, are individual cells of the alveolar process in which teeth are located. They are separated from each other by bony interdental (interalveolar) partitions. Inside the alveoli of multi-rooted teeth there are also internal (intra-alveolar) interradicular septa, which extend from the bottom of the alveoli and divide the alveoli into chambers (according to the number of roots). The alveolar socket of the tooth has clear, defined boundaries, and it has all the conditions for bone regeneration; you just need to help it maintain its contour.
Proper oral care after removal.
It is important to follow your dentist's advice regarding oral care after the extraction procedure. Your doctor will explain to you in detail how to prevent pain, discomfort and inflammation. After recovery, you can contact us for implantation and prosthetics. Our qualified dentists will help restore the beauty and naturalness of your smile using the most modern prosthetic methods.
Tooth extraction RUB 3,500.
Tooth extraction (complicated) RUB 5,000.
Tooth extraction with bone grafting RUB 15,000.
Removal of an impacted tooth RUB 15,000.
Curettage of tooth socket RUB 1,000.
Resection of the root apex 10,000 rub.
Increasing the anatomical length of a tooth RUB 10,000.
Excision of the hood (pericoronitis) RUB 3,000.
Lip frenuloplasty RUB 3,000.
Tongue frenuloplasty RUB 2,500.
Gum correction with laser RUB 2,500.
Laser gum retraction (1 tooth) 500 rub.
Treatment of alveolitis (curettage, drug treatment) RUB 1,500.
Open curettage (1 tooth) 1500 rub.
Opening an abscess 2000 rub.
Hole preservation procedure
Preservation of the socket of an extracted tooth is a fairly simple and effective operation for preserving bone volume and maximizing the preservation of the natural contours of the alveolar socket. This surgical procedure is performed under local anesthesia and does not pose any risk.
Usually the operation is carried out in several stages:
- treatment of the hole after tooth extraction with special antiseptic compounds;
- installation of a membrane to protect the vestibular wall;
- filling the socket cavity with granular bone-forming substance;
- fixation of the operating surface by tensioning the free edges of the connective tissue;
- applying a bandage or a thin, neat suture.
Complete healing of the postoperative area occurs by the fourth week, and after 3–4 months, in some cases 6 months, if the condition is satisfactory, this area can be used to install an implant.
The mucous membrane of the alveolar ridge - what do you need to know about it?
The mucous membrane covering the alveolar ridge can be divided into two types, attached and mobile:
In earlier literature, the mobile mucosa is called lining, and the attached mucous membrane is called chewing - and this, in my opinion, is a more correct terminology, and therefore in this article we will use it.
The border between the lining mucous membrane and the chewing gum is called the transitional fold. Its position and configuration is an important factor influencing the condition of the gums around teeth and implants, and we will talk about this a little later.
From a clinical point of view, we can distinguish two significant parameters of the chewing gum:
Collectively, they are called a phenotype, but, for greater understanding, hereinafter we will separate them and simply call them:
– D – chewing gum thickness (biotype)
– L – width of the chewing gum area.
Gum phenotype is an individual thing, depends on the genotype or, more simply put, is inherited in the same way as eye color, hair color or leg size. There are people with pronounced and developed chewing gums, and vice versa, there are those who have a little less attached gum area than none:
In 2016, I conducted a large study, part of which I used for my report on the preservation and formation of the gingival contour during the stages of implantological treatment. In general terms, we examined the gingival phenotype (albeit in relation to immediate implantation) in 330 clinical situations:
That is, in almost two-thirds of clinical situations, the width of the chewing gum area L exceeds 3 mm, while biotype D is more than 1 mm in the vast majority of patients:
The study itself and its clinical interpretation are here>>
I'll explain a little later why we need insight into these numbers.
Important note: the phenotype of the mucous membrane, along with the state of the bite, is one of the factors predisposing to periodontitis, an extremely unpleasant disease of the dentofacial apparatus.
From this point of view, it is worth noting that it is not the “susceptibility to periodontitis” and not “periodontitis” itself that is inherited, but only phenotypic risk factors for the development of this disease. Accordingly, knowing the etiology and pathogenesis of recessions, peri-implantitis, periodontitis and the role that the gum phenotype plays in this pathogenesis, a simple question comes to mind:
Can we, by influencing the gum phenotype, reduce the risks of developing recessions, peri-implantitis and periodontitis?
It turns out we can.
Treatment quality criteria
The main criterion for the quality of an alveolar socket preservation operation is its independent complete healing and maximum preservation of bone tissue, preservation of the natural contour and volume of the alveolar ridge, improvement of the condition of soft tissues and simplification of further stages of treatment. If the operation is successful, there will be enough bone tissue in the socket to install a dental implant. Separately, it is worth highlighting the advantages of condomization for the doctor and the patient - this is improved long-term treatment results, more predictable aesthetics and, of course, saving time for the doctor and the patient.
Where does it all begin?
And it all starts with a low-traumatic tooth extraction.
And this is the real problem. Neither patients nor some doctors consider this an important procedure, although proper tooth extraction could save a lot of effort and money during further implantation.
Let's reformulate the problem of the delete operation. Let us designate it not as “ tooth removal at any cost ,” but as “ tooth removal with maximum preservation of surrounding tissue .” Even in case of acute pain. Because if a tooth is literally ripped out with half of the alveolar ridge, no subsequent preservation will help avoid osteoplasty.
Therefore, sometimes low-traumatic tooth extraction takes a long time and requires more than just working with forceps:
then
In general, friends, by spending a little more time and effort on tooth extraction, you can seriously make your future implant treatment easier.
Indications for condom
Preservation of the socket of an extracted tooth is indicated for everyone who in the future wants to install a dental implant in its place. The process of loss and resorption of the jaw bone at the site of the extracted tooth begins immediately after the operation. In the first year, bone tissue resorption will be 25% in volume, and over the next 3 years the loss in width will be 40 - 60%. In the case of socket preservation after tooth extraction, a larger volume of bone tissue in the jaw and the most natural contours of the alveolar process are preserved. And then, subsequently, the likelihood of such a complex operation as alveolar bone augmentation when installing an implant will most likely not be required.
How is the procedure carried out?
Tooth extraction at the Doctor Bon clinic is carried out as carefully and carefully as possible. Our specialists will do everything to ensure that this procedure becomes:
— Painless
. The dentist will carefully administer an anesthetic to the patient.
— Fast
. Our doctors use special surgical or classical instruments, taking into account the specifics of the upcoming procedure.
— Has no negative consequences
. The doctor will provide detailed information about the necessary procedures to speed up the healing and recovery process
Following important rules of oral hygiene after a dental procedure will help you avoid unpleasant painful sensations by speeding up the healing of your gums.
Contraindications
Preservation surgery is subject to the same restrictions as any osteoplastic surgery. Separately, I would like to note that it is not recommended to preserve a hole after tooth extraction in a state of acute pain, since the risk of complications increases. But in each specific clinical case, the actions of a professional dentist are strictly individual. Sometimes situations arise when you have to take risks, but this is due solely to medical indications. In any case, it is necessary to understand that performing a tooth extraction operation and subsequent preservation on a planned basis is better than as part of emergency care.
this is the paradox...
... that there are very few clear manuals, recommendations and described experience in the conservation of holes. The authors are content with either drawings or not entirely convincing “before” and “after” photographs, from which it is not clear whether the tooth socket healed “on its own” or such healing is a consequence of the conservation procedure.
In other words, in theory everyone knows how and why this is done. I am sure that most doctors are fine with their practice, but very few colleagues are able to clearly demonstrate their own experience. Therefore, in fact, I had to master everything on my own, simultaneously making mistakes and complicating my own work. But who said that implantology and surgery are easy?
Restrictions
It is logical to perform a preservation operation after the removal of permanent molars, within the so-called sevens, second molars (except for wisdom teeth, eights), since when baby teeth fall out, bone tissue does not resorption. There is no upper age limit for performing an operation aimed at preserving the natural contours of the alveolar process.
Advantages of preserving the socket of an extracted tooth
- excellent preservation of bone tissue integrity;
- no need for complex and expensive procedures for artificial bone augmentation;
- protecting the socket from infection throughout the healing period;
- an ideal method for working with bone areas on the upper jaw located adjacent to the maxillary sinuses (the risk of injury to the air cavities during certain types of bone augmentation is eliminated).
Price
According to the classifier of surgical interventions in the oral cavity, condomation is not among the standard surgical interventions and this, of course, affects the cost of its implementation. In addition, the price of osteoplastic materials and related products is quite high. Some materials are used only in conjunction with a special membrane to avoid ingrowth of soft tissue into the alveolar socket. The price is also affected by the method of tooth extraction. Removal of a tooth or tooth root is sometimes still a traumatic procedure, leading to direct loss of alveolar bone and soft tissue. With atraumatic removal, the alveolar bone is preserved in a larger volume, which reduces the final cost of the operation.
Preservation of the socket after tooth extraction is an important procedure when planning the installation of an implant. Timely preservation of the socket will allow you to preserve such valuable bone tissue and avoid a much more complex and expensive operation to build it up - augmentation, as well as significantly reduce the overall treatment time. The cost of preserving the natural contours of the alveolar socket pays off, because you thereby provide the teeth surrounding it with a reliable position, and as a result, during implantation, you get an imitation of the removed tooth root. This procedure applies even to those patients who do not intend to restore or replace a lost tooth with an implant, because in this case the gingival contour will have the most aesthetic appearance, without failures, and will allow for the most aesthetic bridge prosthetics. Therefore, reservation is gaining increasing popularity in dental dentistry.
According to antiplagiat.ru, the uniqueness of the text as of October 16, 2018 is 90.3%.
Key words, tags: tooth extraction, wisdom tooth, bone tissue, implant installation, augmentation, implantation.
*Images: Astra Tech Dentsply Implants; Principles of hard tessue regeneration and implant therapy.
In what cases is tooth extraction necessary?
Our specialists always strive to preserve the teeth of their patients. Removal is carried out only in the following cases:
- Tooth fracture
.
- Difficulties with wisdom teeth
. Removal is necessary if wisdom teeth shift and deform the dentition, damage the soft tissues of the cheeks during chewing and interfere with a full life in general.
- Deformation of the dentition
. If there is an incorrect bite and if there is deformation of the dentition, the removal of interfering teeth is recommended on the recommendation of an orthodontist.
- The occurrence of dental diseases
. These include purulent periostitis, sinusitis of the maxillary sinuses, etc.
- If it is not possible to carry out prosthetics and install a crown
.
In some situations, resorting to such a radical treatment method is not recommended. This procedure should not be carried out in case of exacerbation of mental illnesses and chronic heart diseases. Contraindications are also certain periods of pregnancy and infectious diseases in the acute phase. In these cases, visiting the dental office should be postponed.
Make an appointment
Mucogingivoplasty - essence and meaning
This unpronounceable word refers to a group of surgical interventions to change the gum phenotype in the area of teeth and implants. By analogy with the classification of osteoplastic operations, we can divide them into two large groups:
Note: of course, there are also “pedicle flaps”, etc., they can be placed in the green sector.
The topic of today's article is collagen matrices, and therefore we will leave modifications alone, then we will only talk about transplantations - those operations when something is transplanted somewhere. And here we are very limited in our choice - we can carry out either autotransplantation, using our own mucous membrane (SDT) or one of its layers (SST) as a transplant (graft), or xenotransplantation - if we try to replace the body’s own tissues with some inert biomaterial.
The goal of all gingivoplastic operations without exception is to change the gum phenotype, or some of its parameters , L and D. In the context of our topic today, we can do this using, among other things, xenografts and collagen matrices.
How possible is it to replace autografts with xenografts? To answer this question, we need to understand what collagen matrices are and how they work.
Types of material and types of stitches
In dental practice, the removal of a permanent tooth is a fairly serious procedure, which in some cases is equal in complexity to surgical operations. The only difference is that it is performed in a dental chair.
Often the teeth have a fairly wide crown and a deep root part. To remove such an organ, the doctor has to make additional incisions in the gum, which must be sutured at the end of the procedure. The material for these purposes must be of high quality.
The main objectives of the performed operation are to achieve rapid healing of the empty area in the jaw arch, provide a good aesthetic effect, and prevent the occurrence of undesirable consequences.
During operations, suture material is a foreign body that remains in living tissue until complete healing. Therefore, it is important that the thread is of high quality and has an optimal chemical composition and structure.
Absorbable and non-absorbable sutures are used in dentistry. Below we will consider both types in more detail.
Absorbable sutures
Surgical sutures that dissolve are characterized by sterility, strength along the entire length, resistance to infections and ease of handling. They are divided into natural and synthetic. During tissue regeneration, no procedure is required to remove the tissue.
Depending on the type of raw material, the threads may decompose without leaving any residual components. These include:
- Dexon. Braided suture thread made of synthetic material.
The raw material used is glycolic acid hypopolymer. It does not contain collagen. Dexon is contraindicated in clinical cases where constant tension of the tissues being connected is expected. The resorption process starts hydrolysis. On the 20th day, the thread retains its strength by 35%. Complete resorption occurs approximately 2 months after application. - Catgut. Material made from natural collagen thread. The resorption process is triggered by the action of proteolytic enzymes.
Strength lasts up to 20 days. It is eliminated from the body by an enzymatic effect within 55-65 days. The thread is characterized by elasticity, smooth surface, good handling properties, high breaking load, and knot reliability.Among the disadvantages, dentists point out the ability to cause mild aseptic inflammation of surrounding tissues.
- Vicryl. Polyfilament absorbable sterile suture material. It features reliable knot fixation and good handling properties.
May cause minimal initial inflammatory response in tissue. Tensile strength is lost 20 days after application. Complete dissolution occurs after 3 months.Compared to Catgut, Vicryl is much easier to work with, despite its synthetic origin. It does not have a slipping effect, is more durable and has a predictable time frame for complete resorption. The suture thread decomposes gradually, transforming into acids.
Intestinal sutures (absorbable stitches) have the advantage that they do not need to be removed. They disappear on their own, without damaging the wound and surrounding soft tissues.
Non-absorbable sutures
Modern non-absorbable suture materials used in surgical dentistry today are polymer threads and silk. They have high strength, good handling properties, are distinguished by manufacturability, affordable cost, and are able to remain in tissues for a long time without adverse reactions of the body.
The following surgical threads are widely used by doctors:
- Polyester. Non-absorbable suture material of synthetic origin.
It is distinguished by its ductility and resistance to tearing. The basis of the multifilament thread is terephthalate (a thermoplastic polymer) with or without a sheath. Living tissues show minimal reaction to a synthetic base. - Nylon. The material is a synthetic insoluble monofilament.
Made from polyamide by extrusion (pressing a melt of material through a forming device). It has a uniform diameter along its entire length and easily passes through damaged structures without injuring them. Among the advantages, it is worth highlighting the high and constant strength of the node, resistance to infections, and excellent visibility in the surgical field. - Silk. The material is made from a protein of organic origin – fibroin.
The thread can be twisted or braided, coated or uncoated. Dentists often prefer it for its strength, flexibility, ease of manipulation, and ability to securely hold knots. Negative properties are expressed in terms of hygroscopicity and the ability to provoke pronounced inflammatory reactions in surrounding tissues.
When suturing the gum, the dentist selects a suture that is appropriate for a particular clinical case. These can be interrupted or continuous stitches.
The first type is most often used in surgery. Characterized by the presence of stitches independent of each other. Each of them is fixed by a separate unit.
This method of suturing a wound allows you to maintain the integrity of the tissue even if one of the stitches breaks.
Continuous suturing is the tightening of the edges of the wound area with a suture thread, which is fixed at the end of the suture with one knot. For the doctor, manipulation in this way is faster, but leaves the risk of damage to one of the stitches and failure of the entire thread structure.
All the pros and cons of laser removal of a dental cyst, the procedure for carrying out the procedure.
In this publication we will talk about the reality of removing teeth at home for disabled people.
Here https://www.vash-dentist.ru/hirurgiya/udalenie-zubov/molochnyih-u-detey.html we’ll talk about the indications for removing a baby tooth in a child and the cost of the issue.