Causes of bleeding Classification How to stop?
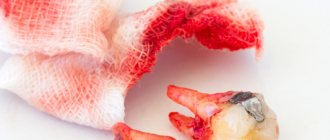
Dentist's help Prevention Tooth extraction is a surgical procedure that cannot be performed without damaging tissues and blood vessels. This causes bleeding from the tooth socket. The blood forms a clot that protects the wound from bacteria. Usually, it stops coming out of the wound after a few minutes, but there are cases when bleeding continues for several hours or even days.
Local reasons
- Vascular rupture during traumatic surgery;
- breaking off the root septum or alveoli (socket);
- inflammation in the area of the tooth that was removed;
- the effect of adrenaline (after the narrowing of blood vessels, the second phase begins - their expansion);
- melting of blood clots clogging blood vessels under the influence of purulent secretions;
- local hyperemia (overflow of blood vessels). Occurs from hot food, drinks, rinses or compresses.
Under no circumstances should you apply heat to the wound after extraction!
Thus, the occurrence of bleeding can be provoked not only by a doctor’s error, but also by the patient’s actions.
Common reasons
The most common of them is a sharp rise in blood pressure as a result of a hypertensive crisis, excessive physical activity, and thermal procedures (bath, sauna, hot bath).
In second place are diseases that affect blood clotting: hemophilia, leukemia, hemorrhagic diseases.
Profuse bleeding occurs with unrecognized vascular tumors (hemangiomas). Therefore, it is important to conduct an X-ray examination, which shows such changes.
Taking anticoagulants can also provoke socket bleeding after removal.
Classification of bleeding
Bleeding is divided into primary, which begins immediately after surgery, and secondary, when bleeding begins after some time.
The intensity of bleeding is determined depending on how much the hole bleeds after removal:
1st degree
– blood flows
for 20-30 minutes
, saturates the tampons and colors the saliva.
2nd degree
– bleeding continues for more than 40 minutes, blood and saliva mix intensively.
3rd degree
– the bleeding does not stop for more than an hour, the patient spits blood.
With prolonged bleeding, the patient's general condition worsens. Weakness, dizziness appear, and the skin turns pale. Blood pressure drops, the heart begins to beat less frequently. In case of bleeding, dentists advise not to delay a visit to the doctor so that he can take measures to stop the bleeding and prevent the condition from worsening.
Bad breath due to bleeding gums
Bleeding from the gums is often accompanied by bad breath. There are several reasons for this:
- proliferation of bacteria against the background of inflammation;
- accumulation of soft and hard dental plaque;
- the presence of deposits under the gum that are not visible to the naked eye.
An unpleasant odor is a formidable symptom, since it does not appear immediately. This means the disease is already progressing. It is impossible to find out the cause and eliminate it on your own (without a dentist); The pathology will become chronic and it will be more difficult to cure.
How to stop bleeding from a socket after tooth extraction
After the tooth is removed, the dental surgeon cleans the wound and applies a sterile swab. The patient is asked to tightly clamp the tampon with his teeth and hold it for about half an hour. If the tampon quickly becomes saturated with blood, it should be changed.
If the bleeding does not stop after 20-30 minutes
, the dry swab is replaced with one moistened with a solution of hydrogen peroxide.
A cold compress can be used to constrict blood vessels. Ice is applied to the cheek, after wrapping it in a towel so as not to freeze the skin. Keep the compress for 10-15 minutes
, then take a break and repeat the procedure.
After surgery, the dentist recommends painkillers. You should follow these recommendations to avoid accidentally taking a product containing aspirin, which thins the blood and can cause bleeding.
If after all the manipulations there is still bleeding from the tooth socket, you need to contact a dental clinic.
SOS remedies against bleeding gums
Sometimes it’s impossible to get to the doctor and you need to wait 1-2 days until the appointment. In this case, several SOS tools will help.
- Rinses: chlorhexidine, oak bark decoction, LACALUT Aktiv rinses with aluminum lactate and sodium fluoride, PRESIDENT Antibacterial with plant extracts - relieve inflammation, prevent bleeding.
- Gels: Cholisal, Parodontocid - reduce pain, remove signs of inflammation.
- Pastes: Forest balm - contains oak bark, stops bleeding, strengthens gums.
All means must be used comprehensively. First, brush your teeth, then rinse (1 minute). After this, the solution is spat out and the gums are dried with gauze: this way the gel is better fixed. Then use ointments, applying with your finger to the entire inflamed surface. If saliva comes out during treatment, you should not swallow it, you need to spit it out.
After the procedure, you should refrain from drinking for 30 minutes and from eating for 2 hours. Treatment is carried out twice a day: after breakfast and at night.
The most effective remedy for diseases in which the gums begin to bleed is antibiotics. They help to quickly relieve inflammation and improve well-being. But they are available with a prescription and are taken only as prescribed by a doctor. Therefore, you won’t be able to buy and prescribe antibiotics yourself. It is better to immediately make an appointment with a specialist so as not to waste time and money on something that will not solve the problem, but will only delay the inevitable.
What does a dentist do?
First of all, the doctor will conduct an examination and make a diagnosis. In accordance with it, the dentist will carry out treatment.
First aid is to stop blood loss. To do this, local anesthesia is performed, blood clots are removed, the wound is dried and the place where the blood is coming from is determined.
Methods to stop alveolar bleeding depend on its cause and location:
- if there is a rupture of the gums or mucous membrane, they are sutured;
- a ligature (a special thread for ligating blood vessels) is applied to the bleeding vessel;
- If there is bleeding from the alveoli (socket), a tampon of iodoform gauze is placed on it. It is left in the wound for several days.
Tamponation is used as a prophylactic measure if there is a risk of bleeding. The tampon is left in the hole for several days. Then they take it out and see how well the wound has healed.
Removing wisdom teeth is potentially dangerous. Such operations are often difficult. Sometimes you have to cut the gum, saw the roots or the tooth itself and remove it piece by piece. Bleeding after such complex operations occurs more often than after ordinary ones.
Measures taken when a hole bleeds after wisdom tooth removal are the same as after regular removal. If there is a history of blood diseases, preparations are made for such an operation in advance. A blood test is carried out, in some cases calcium chloride injections and vitamin C
and
K.
_
If the cause of alveolar bleeding is systemic diseases, general hemostatic agents are used (calcium chloride, calcium gluconate, aminocaproic acid, dicinone, vikasol).
For hypertension, antihypertensive therapy is prescribed. After the pressure normalizes, the bleeding usually stops.
Stopping bleeding during dental restoration
November 7, 2013
Introduction
Traxodent paste
It would be great if the gums did not bleed, since blood entering the surgical field greatly complicates the restoration of teeth. The cause of bleeding gums during restoration operations is dental plaque or trauma. Plaque leads to gingivitis, caries or periodontitis. Trauma that results in bleeding may occur during surgery. The wedges exert lateral pressure on the periodontal papilla. The cavity sealing process uses metal or plastic matrices with sharp edges that can injure healthy or inflamed tissue. Dental burs are used to remove caries, excise inflamed tissue and widen the gingival sulcus. Retraction cords are placed to deflect or pull back the gum in an attempt to reach the edges of the cavity. All this leads to blood contamination of the restoration area, which in turn complicates procedures such as taking accurate impressions, preparing the dental cavity, prosthetics and cementing. This problem is typical for orthopedic dentistry.
Dental prosthetics and periodontal condition are interconnected. Poor dentures may have ridges and difficult-to-clean areas that allow plaque to accumulate. In adolescents and older adults, oral hygiene may be poor. Insufficient prevention of plaque formation leads to the need for dentures. In addition, the main contributing factor to dental prosthetics in patients in the following case studies is a diet high in highly refined carbohydrates (carbonated drinks) and lack of nutrients (refined foods).
Rice. 1 Blood got into the first impression, resulting in voids
In order to exclude the development of gingivitis or periodontal pathology, it is necessary to ensure an accurate marginal fit of the prosthesis. A good example is fixed orthopedic restoration. The fit of the prosthesis depends on the completeness of the impression. If the dental laboratory receives an impression that is incorrect due to blood contamination, problems with the prosthesis arise. Based on such impressions, stamps will be inaccurate due to the formation of voids and bubbles. (Picture 1). If a commercial dental laboratory produces a denture using an inaccurate die, the dentist will receive an inaccurate denture that will not fit the patient and will be rejected. Everyone will be disappointed - the patient, the doctor, and the dental laboratory. As a result, everyone loses income. The patient will need to take time off work, the doctor will need to provide additional chair time, and the dental laboratory will need to facilitate the entire process. When a problem occurs, people usually blame it on someone else. For the dentist this may seem like a personal failure, but in reality it is a systemic failure. If this system is not corrected, the dental office's main source of income will suffer. The main task is to understand how blood and gingival fluid enter the surgical field during restoration work, and what can be done to improve the control system.
The defective impression was made according to a standard procedure using a retraction cord soaked in a hemostatic solution and a one-step impression. The thread was placed on the inflamed tissue to treat subgingival caries. Treatment of subgingival caries required subgingival extension of the tooth core, which led to the need for subgingival preparation for a crown. Bleeding of the tissue is typical for such cases. The system used must control bleeding during the impression taking process.
Rice. 2 Traxodent paste is applied to the bleeding groove
To ensure the accuracy of the indirect technique, a new impression must be taken. You should wash the bleeding tissue and try to dry the wet area. A straight cannula is attached to the Traxodent syringe. In this case, the cannula was bent over the handle of the mirror at an angle of 90°. This facilitates positioning in posterior areas of the mouth where direct access is not possible. Traxodent paste should be applied over the bleeding tissue, slowly squeezing over the gingival sulcus along the edge of the preparation.
The paste can remain in the groove for 1-2 minutes (Figure 2), then it must be rinsed with a water/air gun. After washing and drying, no bleeding is observed, the gingival sulcus becomes dry. To obtain a one-stage impression, impression material of low and medium viscosity is used. Other types of impression material are used with no less success.
Fig. 3 The repeated impression, in which no blood has entered thanks to Traxodent paste, has no voids
Traxodent paste is a retraction system based on Hemodent paste. The paste contains aluminum chloride, which causes tissue retraction and contraction. Aluminum chloride promotes protein precipitation, contraction of blood vessels and removal of fluid from tissues. Aluminum chloride-based paste reduces the risk of postoperative inflammation. Aluminum chloride is the least irritating of the retraction medications. This drug, placed in the groove, does not cause noticeable gum recession. Pallor of the gums is the first sign of the paste's action. After this, the oozing blood turns brown and stops flowing. These two signs indicate hemostasis and a positive result of impression taking. (Figure 3).
Thanks to the methods used in this system, a flawless re-impression is obtained without the use of additional retraction cords. A re-impression using Traxodent paste is preferable because a small amount of impression material is left behind the preparation edge. This ensures that the edges of the plaster die are precisely processed in the laboratory, resulting in a precise fitting prosthesis.
Rotational curettage with Traxodent paste
Rice. 4 Blood and fluid in the gingival groove
Let's consider the case when the tooth has an inlay for building amalgam on pins. This tooth requires support from the entire crown. This tooth had a healthy groove and sufficient amount of attached gum. The entire crown requires a clasp to improve prognosis. Creating a clasp requires preparing the tooth to the bottom of the gingival sulcus. Rotary curettage was used to create a groove using a high-speed diamond bur to quickly remove epithelial tissue in the groove adjacent to the margin. Studies have shown that rotary curettage has little effect on gingival margin height if there is adequate gingival keratinization.
Rice. 5 Traxodent paste applied close to bleeding tissue
Rotational curettage is necessary to create 0.2 mm of thickness in the sulcus to maintain adequate thickness of the polyvinylsiloxane impression material. This thickness is required to create tensile strength and prevent breakage when removed from the oral cavity. Removal of the sulcus mucosa resulted in bleeding in the repair area (Figure 4).
Traditional methods would require the application of a retraction cord for 4 to 10 minutes to widen the groove. In this case, Traxodent paste was applied for 2 minutes to control the bleeding caused by rotary curettage (Figure 5). Additional deflection was mediated by the use of the Premier retraction cap (Figure 6). After rinsing with a water/air gun, only amalgam residues are retained. The groove is dry, hemostasis has been achieved (Figure 7).
|
|
Application of Traxodent paste in the aesthetic area
For aesthetic procedures on anterior teeth, creating a groove around the edge with a bur, floss or laser may not be desirable as it may detract from the appearance. Cosmetic restoration procedures are difficult because the preparation line is in close contact with the gum. If the root of the tooth is very dark, a dark line appears in the area of the neck of the tooth. Patients view this as a cosmetic defect.
Applying a thread can lead to ulceration or inflammation of the connective epithelium. The problem is that it is difficult to control the force of thread application. Other trauma, such as mechanical pressure or surgical damage, can cause unwanted migration of the gum line away from the margin. Traxodent paste is the least traumatic method of drying the field and causes slight displacement and retraction of the tissue.
Let's consider a clinical case. The patient is very concerned about the aesthetic outcome and does not like the dark contrasting color along the gum line. She had a cracked porcelain veneer that needed replacing. The tooth has already been prepared at the edge of the gingival sulcus. The tooth has already been prepared at the crest of the gingival sulcus, and the edges will remain in the same position (Figure 8). Due to accidental contact of the bur with the groove, some areas were damaged and began to bleed. Traxodent paste is applied to the groove and remains there for 1-2 minutes (Figure 9). The tooth is washed with an air-water jet and dried. The area is ready to receive an impression (Figure 10). A one-step impression using low to medium viscosity tray material will produce an accurate impression without bubbles or voids. When examined after 3 months, the margin remains stable and within the aesthetic zone (Figure 11).
|
|
|
|
Hemostasis with Traxodent paste for class II fillings
Rice. 12 The gums are accidentally damaged when drilling out caries
The risk of blood entering during the filling of class II cavities is as high as when installing a crown or bridge. This problem may mean longer procedures for the patient and changes in the dentist's chair schedule. Bleeding in the interproximal area is usually associated with caries (Figure 12). Bleeding begins from the inflamed interproximal gingival area if it is touched with a bur during removal of carious dentin.
Bleeding also occurs during isolation of a carious lesion when a ring, wedge or rubber gasket comes into contact with inflamed tissue (Figure 13). Traxodent paste is applied to the bleeding area located in the deepest part of the interproximal pocket (Figure 14). After 1-2 minutes, the paste is washed off with an air-water jet and hemostasis is confirmed. It is obvious that the entire surface of the cavity can be visualized, after which filling is carried out in the usual way.
|
|
Discussion
The value of these case reports is that they demonstrate a new hemostasis technology (Traxodent paste) that can solve common bleeding problems in the area of restorative treatment.
Thanks to its balanced fluidity, the paste can penetrate and remain in hard-to-reach areas of the groove. This balanced flow is important when treating the upper and lower dental arches, as the drug remains in the groove without getting into the laryngeal vestibule or throat. This is important for the patient, as the procedure becomes less unpleasant. Typically, hemostatic agents are strong astringents that create a dry, tight, and rough feeling in the mouth. This new technology is important for the dentist because it allows the drug to remain in direct contact and in its entirety in the gingival sulcus. There is no need to re-apply the drug due to dissolution by saliva or leakage. After application, the drug remains in place, even in contact with the tongue or cheek. Paste differs from liquid hemostatic agents in its ability to absorb liquids. Treatment areas adjacent to the mucous membrane of the alveolar processes of the jaw may become contaminated to deeper spaces. The physician should be aware of the problems that arise in such areas with insufficient adjacent keratinized tissue. As one of the warnings, we can mention the risk of leaching of the hemostatic drug into deep areas between tissues that are not intended for applying the product. The paste is not intended for the treatment of gingivitis, periodontitis and other diseases. The doctor should supervise the application of the paste to the dental treatment area. Traxodent paste is intended to be inserted onto the surface of the tissue, like a bandage, and not to be inserted into the submucosa.
Conclusion
Bleeding is a common problem that occurs during the dental restoration process. Common causes include plaque-induced erythema due to gingivitis, along with the use of instruments in the treatment area or the inadvertent use of instruments that create tears in the gingival tissue during restorative procedures. Any injury to the inflamed tissue leads to bleeding in the restoration area. Bleeding leads to deformation of the impressions, lack of adhesion of the filling and contamination of the cement.
Traxodent paste is a retraction system based on Hemodent paste, which contains aluminum chloride. Traxodent stops gum bleeding and causes temporary soft tissue contraction without further tissue damage.
Dean Eledge DDS, MD Associate Professor, AEGD
see also
September 13, 2013
Traxodent/Traksodent - material for hemostasis and gum retraction, Premier
Retraction system based on Hemodent® paste
March 21, 2012
PREMIER. Unconditional quality of dental materials
The American company Premier was founded in 1913. Soon it will be 100 years since Premier cherishes its traditions and values its reputation, so the company’s specialists carefully monitor the production process and always strive to improve the level of product delivery. UNIDENT presents the Premier line of dental materials, in which you can find materials that are indispensable for a dentist’s work.
October 30, 2011
Traxodent System: Predictive Management of Gingival Tissue
In modern dentistry, control of gingival fluid and gingival tissue is the primary criterion required for a successful clinical procedure. "Traxodent" is a unique system for high-level hemostatic processes. It is available in convenient syringes. Its paste-like consistency improves the retraction of gingival tissue, and 15% aluminum chloride, which is part of the paste, has very high hemostatic properties. Return to section