Central lower incisor
Average age of eruption: 6-7 years
Average age of root formation: 9 years
Average length: 20.7 mm
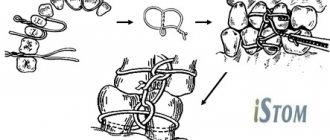
Narrow and flat in the labial-lingual direction, the lower central incisor is the smallest adult tooth. Radiologically it is visible in only one projection and thus appears more accessible than it actually is. The crown, narrow in lingual projection, has a limited area for access. For gentle access formation, a fissure bur and a spherical bur No. 2 are used. The access cavity should be oval and performed on the lingual side.
The lower central incisor often has two canals. One study reported that 41.4% of mandibular central incisors studied had two separate canals, of which only 1.3% had two separate apical foramina [1]. After completing the access formation, the doctor must examine the tooth cavity to identify an additional canal. Endodontic treatment failures in the lower incisor area are most often associated with an unidentified canal, usually in the lingual location. To create conditions for the straight entry of endodontic instruments into the additional canal, access can be expanded in the incisal direction.
There is a great danger of perforation of the vestibular wall, but it can be avoided if the doctor remembers that it is almost impossible to perforate in the lingual direction, since the bur axis is in contact with the incisal edge. The slit-like lumen of the canal is so common that it can be considered a normal variant, and this requires special attention when cleaning and shaping.
Lateral perforations and pulp anatomy will be discussed in an illustration of the lower second molar.
Lateral lower incisor
Average age of teething: 7-8 years
Average age of root formation: 10 years
Average length: 21.1 mm
Very similar to the lower central incisor, so access cavity preparation follows the same principles.
Their similarity can cause rare but serious errors. Hasty installation of a rubber dam, identical fillings and carelessness can lead to preparation of the access cavity on the wrong tooth. This error can be prevented by marking the vestibular surface of the tooth with a felt-tip pen before applying the rubber dam.
Trauma, periodontal disease, carious lesions and malocclusion can lead to obliteration of the canal. When moving apically to identify the orifice, great care must be taken to prevent unnecessary destruction of the crown and root. Labial perforations were discussed in Illustration IX. If the bur is not oriented along the long axis of the tooth, there is a risk of lateral perforation. The situation becomes more complicated with the traumatic loss of an anatomical crown. Without anatomical landmarks, a lateral perforation can be easily made when moving in a coronal direction. To prevent this, access is carried out without a rubber dam so that the root can be palpated.
Lateral perforation with endodontic files and Gates-Glidden burs is facilitated by the presence of slit-shaped canals with a narrow, hourglass-shaped cross-section. To avoid vertical fracture along the approximal root wall, minimal expansion and preparation of the space for the abutment pin is indicated.
Apical curves and accessory canals are common in the lower incisors.
Clinic, diagnosis and differential diagnosis of wear of hard dental tissues
Only a third of practicing dentists in Europe report erosive or other tooth wear in their medical records [13]. The codes and criteria used in medical documentation do not allow recording of non-carious lesions.
The classic description of erosion in the literature is “a saucer-shaped defect with clear boundaries and a smooth bottom, located on the vestibular surface between the neck of the tooth and its equator” [14].
| Table No. 1. Variants of clinical manifestations of erosive lesions of teeth depending on the etiological factor | |||
| Clinical picture | Saucer-shaped defects in the cervical region of the anterior group of teeth of the upper jaw, unilateral or bilateral | Defects on the oral surface of the chewing group of teeth in the upper jaw | Defects on the oral surface of the anterior group of teeth or all teeth of the upper jaw |
| Cause of erosion | Diet, medications | Gastrointestinal diseases gastroesophageal reflux | Vomiting in eating disorders |
However, today the clinical manifestations of erosion are more varied and depend on the etiological factors of this disease (Table No. 1).
In the early stages, erosive tooth wear appears as a loss of physiological surface gloss. In later stages, changes occur in the original morphology of the tooth.
With frequent consumption of foods and drinks with low pH, concavities appear on the vestibular surface of the front teeth, the width of which clearly exceeds the depth.
In patients with eating disorders [15], due to frequent vomiting, enamel loss first occurs on the palatal surfaces of the central and lateral incisors of the maxilla. The enamel loses its characteristic pattern and looks “glazed.” Next, in descending order, the palatal surface of the molars, the palatal surface of the canines, the occlusal surface of the molars, the palatal surface of the premolars, and the occlusal surface of the premolars are affected in the upper jaw. The cutting edge of the incisors becomes thinner, the chewing surfaces become flattened. In severe cases, the occlusal morphology disappears. The rate of decline depends on episodes of vomiting and usually becomes noticeable within 3 years.
In patients with gastroesophageal reflux, enamel is lost from the palatal and occlusal surfaces of the upper molars [16].
The clinical picture of an abfraction defect differs significantly from that of an erosive one: a defect in the form of a step or ledge with an acute angle at the base, occurs in the area of the tooth neck, and sometimes extends into the subgingival region (Fig. 1).
Rice. 1a. Abfraction defects.
Rice. 1b. Abfraction defects.
Gingival recession may complement the clinical picture, but its presence is not always observed.
To diagnose abfractions, a thorough history and diagnosis of occlusal relationships are very important. An abfraction defect, unlike erosion, necessarily has sharp edges. A wedge-shaped defect is always combined with gum recession, and its depth always exceeds its width (Fig. 2a, Table No. 3).
Rice. 2a. Wedge-shaped defects.
The wedge-shaped defect is localized in the cervical region on the vestibular surfaces of the teeth that protrude most strongly from the dental arch, most often the first premolars and canines. It may be more pronounced on one side depending on which hand the patient uses to brush their teeth. The shape resembles a triangle, the apex of which faces the tooth cavity.
For the purpose of differential diagnosis of wedge-shaped and abfraction defects, occlusal relationships are diagnosed. And if supracontacts are detected on teeth with V-shaped defects and overload of individual teeth and groups of teeth is recorded, then the diagnosis of “abfraction defect” is more justified. Sometimes in the same patient we can observe a combination of wedge-shaped and abfraction defects.
With increased abrasion, the teeth of the upper and lower jaws are affected. Tissue loss is observed on the chewing surfaces of molars and premolars, the cutting edges of the frontal teeth (Fig. 2b), the palatal surfaces of the anterior teeth of the upper jaw and the vestibular surfaces of the anterior teeth of the lower jaw. The affected surfaces are hard, smooth and shiny. Sharp edges and chips are observed in patients suffering from bruxism.
Rice. 2b. Increased erasure.
Differential diagnosis according to clinical manifestations is given in Table No. 2.
| Table No. 2. Clinical picture of various forms of tooth wear | ||
| Diagnosis | Characteristics of the lesion | Location of the lesion |
| K03.2 Erosion | An oval or saucer-shaped defect with clear boundaries, the bottom is smooth, shiny, loss of occlusal pattern, “vitrified” enamel |
|
| K03.1 Grinding (abrasive wear) of teeth - wedge-shaped defect | Defect in the shape of a triangle, the apex faces the oral cavity, the depth exceeds the width |
|
| K03.18 Other specified diseases of dental hard tissues (abfraction) | Angular defect with sharp edges |
|
| K03.0 Increased abrasion (wear) | Horizontal or vertical loss of hard tooth tissues |
|
We should not forget that in the clinic we can observe a combination of various lesions in one patient (Fig. 3-8).
Rice. 3. Patient I., 48 years old, erosion, abfraction, abrasion, bruxism + caries.
Rice. 4. Patient K., 42 years old, erosion (covered by restorations), abfraction, abrasion, bruxism.
Rice. 5. Patient Shch., 53 years old, erosion, abfraction.
Rice. 6. Patient L., 63 years old, crossbite, erosion (covered by restorations), abrasion, bruxism.
Rice. 7. Patient K., 43 years old, tetracycline teeth, abrasion, bruxism.
Rice. 8. Patient S., 44 years old, erosions (covered by restorations), wedge-shaped defects, abrasion, bruxism.
The stress concentration due to bruxism can act synergistically as a cofactor with acids as well as abrasives to produce various manifestations of non-carious lesions. Signs of bruxism in the clinic include increased abrasion, abfraction defects, chipping, tension in the masticatory muscles, and much more.
Mandibular canine
Average age of teething: 9-10 years
Average age of root formation: 13 years
Average length: 25.6 mm
The canine of the lower jaw is more powerful and significantly wider than the incisors in the mesial-distal direction. It rarely causes treatment problems. The atypical form with two roots can be problematic, but is rare.
The access cavity is oval and can be expanded in the incisal direction to facilitate vestibular-lingual access. In the cervical region the canal is oval, in the middle third it is rounded. To completely clean its walls, directed instrumental action is necessary.
If there are two roots, one of them will always be easier to instrument. The other canal must also be opened and funnel-shaped in accordance with the first to prevent dentine filings from entering it and impairing access. Pre-bending the instruments during the initial approach will allow the clinician to walk along the walls of the buccal or lingual root until the tip of the instrument enters the orifice. Once a difficult-to-reach canal has been identified, every effort must be made to shape and create a funnel-shaped orifice to keep access open.
Variety of occlusal surfaces of the tooth
Simon Haug
PhD, dental technician (Wurzburg, Germany)
Modeling natural fissures is one of the most difficult tasks when creating artificial teeth. To obtain a satisfactory result, not only knowledge of the details of the occlusal surface is required, but also many years of professional experience. Achieving a natural form while maintaining full functionality is truly the most important goal of dentistry. Regardless of the material used, wax or ceramic, it is possible to find a starting point and achieve a targeted analysis of predicted success. In this article, functional aspects will be omitted to focus entirely on form design. But at the same time, we must not forget that the principles of aesthetic and natural restoration are invalid without taking into account functionality.
Analysis of outlines and shapes alone cannot show in which direction to reproduce the structures obtained as a result of the analysis. This article reveals different methods for fast and natural fissure sculpting. For this reason, we will not take into account the points of contact and occlusal connection with the opposite jaw, describing only the modeling of the fissures (Fig. 1, 2).
Rice. 1. Fig. 2.
At the heart of the whole scheme are fundamental questions of design of the shape in the front part. They relate to the nature of the tooth and its components. Should the modeling take into account the patient's age and the state of abrasion of the residual dentition? What is the morphology of the patient’s dentition: is it complex and sophisticated or simpler? What is the depth of the morphological surface?
Of course, functionality takes precedence over aesthetics. However, in this case we will not talk about the contact situation, but will try to achieve an effective and efficient production of the occlusal surface.
For modeling, we chose 2 teeth that differed in several respects.
The first model (Fig. 3, 4) represents a first molar with areas of severe abrasion in the mesiopalatal region of the cusp and on the cristatransverse. These abrasive areas resulted from the interaction of lateral joint displacement and retrusion. The occlusal surface of the tooth and adjacent teeth is complex, so fissure modeling will be labor-intensive. Speaking about the modeling on the incisal cusp, we see two convex shapes opposing each other and forming a narrow bottom of the fissure.
Rice. 3. Fig. 4.
I repeat once again that this situation is typical of the surface on cutting cusps. There are several areas of abrasion around the palatine tuberosity. The lateral descent of the fissure, by which we mean the difference in height between the central recess and the peak of the cusp, is quite high on this molar. Also on the adjacent hillocks a pronounced relief is clearly visible. A crown that fits the existing dentition and has a high lateral descent of the fissure is very dangerous and can cause impaired functionality.
In Fig. 5 and 6 show another molar, different from the first in some respects. The areas of abrasion are less pronounced, but the cristatransverse has already undergone some wear. The occlusal surface is simpler in comparison with the first one. The fissures on the cutting cusps are shallow and have a wide bottom. Modeling a tooth with such simple elements is sometimes a more complex process than modeling a tooth with a variety of structural elements. The lateral descent of the fissure on the second molar is less steep (Fig. 7).
Rice. 5. Fig. 6. Fig. 7.
Modeling
At this stage of the comparative analysis of molars, we will give a more detailed description of them (Fig. 8, 9).
Rice. 8. Fig. 9.
The modeling of the outer side of the tooth is done in detail. The fish mouth technique allows us to best predict the outcome of the simulation. The outer side is modeled with a transition to the surface of the tooth. Thus, the palatal cusps are modeled a little wider. It is also important to mark a clear line of the cutting edge of the tooth. This is especially clearly reflected in the external outline of the tooth, which has a twisting effect (Fig. 9). In index 1, the distal buccal cusp is more inclined on the occlusal surface than the mesiobuccal cusp. In index 2, the medial palatal tubercle is more inclined towards the center than the distal buccal tubercle. Thus, the outer surface takes on the shape of a rhombus. In Fig. 10 The first molar visible from the buccal side. In the area of the index, the distal buccal cusp is “screwed” deeper into the surface of the tooth, but the peak, however, is located quite far from the surface of the tooth (Fig. 11–13).
Rice. 10. Fig. 11. Fig. 12. Fig. 13.
The medial palatal tubercle is the highest and widest.
Peripheral abrasive areas are expressed on the slope of the cusp. The central slope of the cusp is surrounded in the medial and distal regions by a structural element (Fig. 14). The cristatransverse is clearly defined at the distal border, as is the medial structural element.
Rice. 14.
The surface looks more interesting due to the sunken shape of the medial structural element. This area was formed due to the pressing of the wax as it hardened. Thus, an arbitrary structure arises that imitates a natural structure. The bottom of the distal fissure is wider than the bottom of the medial one. In Fig. 14 medial structure, which was modeled according to this factor and slightly redesigned. The distal fissure was modeled from liquid wax. It can only be formed when cooled using lecron. It should be noted that when modeling a fissure, movements with the lecron are not made along the fissure, but from its bottom to the top towards the central slope. This means that the lecron moves from pointer 3 to the red dot area. This allows you to create a natural fissure with a wide bottom (Fig. 15).
Rice. 16.
The second molar is quite simple. In Fig. 16 it can be seen that several wavy outlines have been added to the surface of the medial palatal tubercle. And yet, the contour of the distal region of the cristatransverse is defined quite clearly. This may have been done to hide the features of simpler occlusal surfaces (Fig. 17).
Rice. 17.
The distal buccal cusp is smaller than the mesiopalatal cusp, yet larger than the mesiobuccal cusp. The modeling of the three elements of the distal buccal cusp begins with a central slope that forms the cristatransverse. Thus, modeling is carried out to the line of the front teeth, and then continues parallel to the line of the incisal edge of the teeth. As a result, a furrow is formed that emphasizes this line; it can also often be found on typical incisal cusps (Fig. 18).
Rice. 18.
The medial structural element almost reaches the central recess and takes on a slight s-shape. The bottom of the fissure descent towards the central slope is much smaller, and, as a consequence, the depth of the fissure is greater compared to the distal structural element.
These grooves are called orthogonal, which allows for greater surface action on the anterior line of the teeth. Using a pin can connect these grooves to the wax surface, but at this stage, as mentioned earlier, this is the last small touch in our modeling. Especially when using pressed ceramics, when the crown or bridge is completely given an anatomical shape, the connection of the surface structure in the wax becomes more important (Fig. 19).
Rice. 19.
The distal structural element consists mainly of a line of the incisal edge of the tooth, which passes through the rather slight slope of the central fissure (Fig. 20). We completely repeated this fissure using lecron, with a clear outline of the front line of the teeth. For functional reasons, an impression of the central slope of the roller is made to prevent unnecessary interfering contacts (Fig. 21).
Rice. 20. Fig. 21.
In the second molar, the above structures are created in a simplified version (Fig. 22).
Before modeling the medial buccal cusp, an element is created between the medial palatal and medial buccal cusps (Fig. 23). The fissures to this element surround a central recess and usually have a narrow bottom. They consist of convex slopes, which are modeled according to a standard pattern, which can be clearly seen under numbers 1 and 2 (Fig. 24).
Rice. 22. Fig. 23. Fig. 24.
A fine curved tip should be used to model this and all other areas of the fissure with raised features. Thanks to fig. 25–27 (Yeti Dental GmbH, Engen you) the shape of the fissures can be accurately determined. The final element has an inherent deviation and is distributed onto the lateral surface of the teeth to give it a natural appearance (Fig. 28).
The medial buccal cusp is the smallest cusp.
Rice. 25. Fig. 26. Fig. 27. Fig. 28.
When modeling the medial buccal cusp, start with the central slope (Fig. 29). There is no cushion on it, and it has a slight height. The distal structural element is slightly shorter than the medial element of the distobuccal tuberosity. But even a small element can significantly influence the fact that the resulting fissures become similar to natural ones (Fig. 30).
Rice. 29. Fig. thirty.
On the cutting cusps you can clearly see how different types of fissures smoothly transform into one another. Thus, in the range from 1 to 2°, a significantly expanded fissure bottom (colorless structure) is determined, which turns into a deep fissure.
In the second molar, which is simpler compared to the molar described above, the convexity of the structural elements on this cutting cusp is less pronounced (Fig. 31). While each is important in its own way, they all transition to a convex central slope in a flatter structure (Figure 32).
Rice. 31. Fig. 32.
conclusions
Even if identical areas were modeled differently in both molars, there are still several basic features in fissure design. As at the beginning of the article, in its final part I would like to emphasize that the truly important aspects were studied without taking into account their functionality, in order to fully focus on the issue of modeling natural chewing surfaces.
First lower premolar
Average age of teething: 10-12 years
Average age of root formation: 12-13 years
Average length: 21.6 mm
Often considered a mystery to endodontists, the mandibular first premolar, with its two canals separating at different levels of the root, can be very difficult to machine.
The crown consists of a well-developed buccal cusp and a small or almost non-existent lingual enamel protrusion. The approach is performed buccally from the central sulcus and directed along the long axis of the root to the central cervical region. The oval-shaped pulp chamber is opened using fissure burs with a cutting apex and elongated spherical burs No. 4 or 6. In teeth with one canal, the pulp cavity in the neck area has an almost circular cross-section, and in teeth with two canals it is oval.
One study reported that “at least 23% of first mandibular premolars have a second or third canal”[17]. The canals can split almost anywhere in the root. Due to the lack of direct access, cleaning, shaping and filling these teeth can be extremely difficult.
In a recent study, Vertucci [13] showed that the first lower premolar has one canal at the apex in 74.0% of cases, two canals in 25.5% and three canals in the remaining 0.5% of cases.
Classification and frequency (%) of canal types in first and second lower premolars
By Vertucci, F. J. Am. Dent. Assoc. 97:47, 1978.
Aesthetic restoration of teeth with a combination of carious lesions and increased abrasion
Modern advances in the development of dental materials significantly expand the capabilities of dentists. Recognition of aesthetic dentistry as a separate area with its own theoretical, scientific and practical developments has ensured the rapid implementation of advanced treatment methods. Routine “filling” is being replaced by restoration, which guarantees high quality restoration of teeth with defects of carious and non-carious origin.
Moreover, it has become possible to treat combined lesions using methods that require minimal excision of hard tooth tissue and ensure preservation of pulp vitality.
Such work is based on the principles of aesthetic dentistry (I.K. Lutskaya, 2011) [2].
The main principle, or starting point, of aesthetic dentistry should be the achievement of treatment results that are as close as possible to the natural parameters of the dentition.
Thus, therapeutic restorations and orthopedic structures are subject to the requirement of maximum similarity with the optimal characteristics of teeth in color, shape, and relief.
Surgical crown lengthening or gingivectomy should not visually increase the original size of the teeth, cause gum recession or “gaping” of interdental spaces [4].
Achievement of the basic principle is ensured through optimal therapeutic effects, which involves the selection of means and methods that do not violate or minimally damage intact structures. First of all, the methods of bleaching, then minimal preparation (microabrasion), and grinding of the non-prismatic enamel layer are considered as therapeutic methods. Preparation, and especially depulpation, is carried out strictly according to indications. Any manipulations must ensure high aesthetics, mechanical strength, and reliable adhesion of restorations to tooth tissues [4].
The principle of conscious cooperation implies that the patient conscientiously and regularly performs the procedures prescribed by the dentist.
Thus, home whitening is prescribed by a doctor and performed by the patient independently, strictly following the instructions. The choice of shades of color, size and shape of the structure is carried out jointly by the dentist and the patient to reach consensus. The scope of surgical intervention is also carried out after obtaining the informed consent of the patient.
Working with photocomposites and modern ceramics has its own fundamental requirements, approaches, and principles that provide scientific validity to the manipulations performed.
The principle of color imitation ensures the modeling of a restoration (structure) with high aesthetic parameters, implying the selection of shades of material that correspond in optical properties to dentin and enamel, followed by imitation of the color of lost tooth tissues [5].
The principle of reproducing natural volumetric parameters implies preliminary planning of the dimensions, shapes, and surface relief of the restoration (structure), followed by the reconstruction of macro- and microstructures [1].
When modeling a restoration, its morphological features must repeat the parameters of an intact tooth, therefore it is necessary to maintain the geometric shape, signs of belonging to the side, and mamelons.
Such large structural elements are modeled with opaque materials.
Individual characteristics, such as surface relief, cutting edge shape, and transparency, are formed using enamel shades in compliance with the rule of preserving the volume of natural tissue.
The principle of adhesive preparation (English: prepare) means increasing the area of contact between the filling and the tooth in order to ensure high-quality bonding of the composite with the dental tissues. The objectives are achieved by excision of hard tissue to intact structures, creating a bevel of the enamel or giving the cavity a certain shape, as well as acid etching and the use of an adhesive system.
The principle of minimizing the effects of polymerization shrinkage is based on the property of the material to decrease in volume during the curing process.
At the stage of tooth preparation, reducing the effects of shrinkage is achieved by excision of thinned protrusions and rounding of the internal corners of the cavity. The absence of a complex design reduces tension in the tooth tissues. The risk of detachment of the filling, the formation of a gap at the border with the tooth, and the appearance of hyperesthesia is reduced when using gaskets made of chemically cured materials: during polymerization, they are “attracted” towards the heat source - the pulp.
During the curing process of a composite, one of the methods for reducing shrinkage is the “soft start” method: reducing the exposure time of the first stage of photopolymerization.
Knowledge of the principles of aesthetic dentistry allows you to choose the most correct methods of influence, ensuring maximum efficiency.
Clinical case
The patient, 35 years old, complained of aesthetic defects of the upper central incisors. Carious cavities are localized on the mesial surfaces of the 11th and 21st teeth. There is a significant decrease in the height of the crowns of the upper central incisors due to increased uneven abrasion of hard tissues (Fig. 1).
Rice. 1. Carious cavities on the mesial surface of teeth 1.1 and 2.1, uneven wear of hard tissues.
The use of composite material for dental restoration involves the following sequence of stages: mechanical cleaning of the tooth surface; choice of photopolymer shades; planning the size and shape of restorations; tooth preparation; use of an adhesive system; filling the defect with a composite; polymerization; coating of teeth with fluoride varnish.
Taking into account the complexity of the work and aesthetic requirements, a nanohybrid composite is used for dental restoration, representing a new class of filling materials characterized by high aesthetic properties: Grandio SO (VOCO). It combines the qualities of photopolymer with the innovation of nanotechnology. For its production, polymer resins with high molecular weight and microfillers with an average particle size of 20-30 microns were used.
Combining nanomers (zirconium silicate particles less than 100 nm in size) with glass-ceramic composite particles made it possible to increase the share of filler in the material to 87%, which reduced the content of organic resins in the matrix and, accordingly, reduced polymerization shrinkage to 1.57%. Filling the material with nanoparticles ensures high marginal stability, easy polishability and good color fastness of the restoration. Thanks to good adaptation to enamel and dentin shades, the so-called chameleon property, the stage of selecting composite shades is greatly simplified. In some cases, one shade of material from one color group (for example, red-brown, group A) of varying degrees of transparency (opaque, enamel, transparent) can be used. In more complex clinical situations, 2-3 syringes with different color characteristics will be required.
Nanocomposites are indicated for filling cavities of classes I-V according to Black, restoring teeth with traumatic injuries and hard tissue defects of non-carious origin. A large selection of shades and color stability of the nanomaterial allow it to be used for aesthetic filling of anterior teeth with correction of shape and color; restore teeth with class II cavities of significant size; used for splinting, making inlays, onlays, adhesive prostheses, restoring the tooth stump for a crown.
The first stage is the mechanical treatment of teeth with fluoride-free paste (Fig. 2). Cleaned surfaces are washed with a stream of water.
Rice. 2. Cleaning teeth from plaque.
The shades of the photopolymer are selected in natural light (the patient is in a sitting position) using the colors supplied with the material (Fig. 3).
Rice. 3. Selection of shades of tooth color.
The surfaces of the teeth are kept moist, which preserves their natural appearance. The opaque composite OA 2 is selected to match the color of the central area, this will avoid the transparency of the filling. To create a natural look, shine and transparency, enamel shades of the restoration are used, which are selected separately for the central (A 2) and proximal sections (A 2 and I), and the incisal edge (A 1 and I). Using opaque alone can create the appearance of a flat or lifeless tooth. The absence of opaque will make the restoration “transparent”. Enamel and clear shades are required to cover the main area of the restoration, the incisal edge and proximal surfaces. A transparent cutting edge with a width of more than 1 mm is assumed.
When choosing tooth shades, the phenomenon of irradiation is taken into account - a change in the size of the surface depending on color and lightness, when warm light colors (yellowish) create the illusion of convexity, and cool colors (blue) create depressions. As a result, the cutting edge of light yellow shades will be perceived as voluminous, while the bluish edge will be perceived as flat and displaced orally. In this case, it is planned to use 4 syringes of composite material: opaque OA 2, enamel A2 and A1, transparent I.
Planning the size, shape and relief is a strictly defined sequence of actions describing the specific anatomical formation of the tooth.
Teeth are measured with a micrometer. The height of the clinical crown of the central incisors is defined as the distance from the marginal level of the gums along the vertical midline to the conventional line of the cutting edge, overlapping the occlusal surface of the lower incisors by 1.5 mm.
Mesiodistal dimensions in the neck area are measured by the distance between two points at the level of the apexes of the interdental papillae, in the equator area - at the level of the middle third of the crown height, in the incisal edge area they are assessed by the distance between the protruding points of the mesial and distal edges of the crown. In this case, odontometry indicates that the width of the tooth in the equatorial region is equal to the height of the tooth and is 8.9 mm in the 11th tooth, 9.0 mm in the 21st tooth.
In the area of the cutting edge, it is not possible to measure the horizontal size of the tooth, since it is erased. The map indicates signs of belonging to a party. The sign of crown curvature is weakly expressed. Due to chipping and increased wear of teeth, the dimensions of the mesial angle are not determined. Based on visual assessment and measurement results, it is planned to change the square geometric shape of the crowns to rectangular by increasing the vertical size by lengthening the cutting edge. The planned vertical dimensions of the incisors are 9.7 mm for the right incisor and 9.8 mm for the left (the height of the teeth differs due to the higher dome of the gingival margin in tooth 21) (Fig. 4).
Rice. 4. Odontometry: tooth width in the equatorial region in 1.1 teeth is 8.9 mm, in 2.1 teeth 9.0 mm. The planned tooth height is 9.7 mm for the right incisor and 9.8 mm for the left.
It is planned to recreate the predominance of the distal angle of the crown over the mesial angle, which is a sign that the tooth belongs to a certain side. The sign of crown curvature is not pronounced: the mesial surfaces have a slight oral location compared to the distal ones, they have a penumbra, and are visually perceived as darker. It is intended to create a slight convexity of the vestibular surface closer to the mesial edge. The individual characteristics of teeth are smooth vestibular surfaces. The length of the contact points between the teeth is planned in such a way that there is enough space for the interdental papilla (from the top of the gingival papilla to the incisal edge). The cutting edge of the teeth is smooth.
To prevent chipping of the filling material, occlusal contacts and the incisal path are aligned using carbon paper.
Teeth preparation is carried out with diamond burs and begins with a thorough necrotomy of the walls and bottom of the carious cavity. In this case, diamond burs (NTI company) are used to process the enamel, first with medium (100 microns), then with fine grain (40-50 microns). The water jet is applied continuously to the drill to avoid irritation of the pulp. Dentin is prepared with carbide burs. The vestibular wall of the carious cavity is partially excised, since it is represented by a thin layer of enamel that does not have underlying dentin. As a result, class IV cavities are formed (Fig. 5).
Rice. 5. Teeth after necrectomy.
All corners are rounded with a spherical bur. On the vestibular surface of each incisor, an enamel bevel approximately 3.5-4.0 mm wide is made in order to recreate the sign of crown curvature and move the convexity of the vestibular surface closer to the mesial edge. The surface is smoothed with a fine-grained diamond bur (40-50 microns). Bevels will ensure an increase in the contact area between the tooth and the composite, as well as the aesthetics of restorations due to a smooth transition of the material at the filling-tooth interface. On the palatal surface, the enamel is ground at an angle of 45°.
The prepared surfaces are thoroughly washed with a stream of water and dried with an air stream. The dentin is covered with glass ionomer cement. Then the enamel is covered with etching gel (30 sec.) (Fig. 6).
Rice. 6. Acid etching of enamel.
After time, the gel is thoroughly washed off, and the enamel surface is dried with a stream of air (Fig. 7). The adhesive is evenly applied to the prepared surfaces, rubbed in with a brush, left for 30 seconds to soak, distributed with a gentle stream of air and polymerized for 20 seconds.
Rice. 7. Central incisors after the acid etching stage.
Filling begins with filling the cavity. The opaque composite (OA 2) is introduced into the cavity in a layer of no more than 2.0 mm in thickness, carefully pressed against the bottom and walls, and photopolymerized for 30 seconds.
The adaptation of the material in the area of the missing vestibular wall of the cavity requires special attention: the level of the opaque layer is located 1.0-1.5 mm below the level of the tooth surface (the difference will allow the formation of the enamel layer) (Fig. 8).
Rice. 8. Adaptation of the opaque layer of the Grandio SO (VOCO) material.
After filling the carious cavity, they begin modeling the half-veneer, which is carried out in compliance with a gradual transition from recreating large details (the geometric shape of the vestibular surface) to reproducing medium ones (signs of the angle and curvature of the crown), and then to modeling smaller elements (the area of the cutting edge). Each subsequent layer is applied on top of the previous one and distributed in different directions using a wide trowel or spatula. The boundary of each layer is created in the form of buoyant waves (Fig. 9).
Rice. 9. The enamel shade of the composite is distributed.
The mesial surface is modeled with an opaque composite throughout the middle and lower tier of the tooth crown. The main landmark is the border of the transparent tooth enamel: in this case, there is about 1.0 mm of free space around the entire perimeter of the tooth, except for the cutting edge, where the width of the transparent layer will be 1.5 mm.
To recreate the sign of crown curvature, a portion of opaque photopolymer is applied in the form of a vertical roller at the border of the mesial and median sections, and then smoothed so that the maximum convexity is maintained closer to the mesial surface (Fig. 10).
Rice. 10. Scheme for modeling the sign of crown curvature.
Modeling of the sign of the crown angle is carried out in the lower tier of the tooth, taking into account the degree of its severity: the distal angle is larger in size than the mesial one. In this case, the latter is modeled in the area of the mesial lower third of the tooth crown, with the filling material distributed towards the cutting edge and mesial contour and giving the corner the desired shape (Fig. 11).
Rice. 11. Modeling the crown angle sign.
The vestibular surface is covered with a thin layer of enamel (A 2) and then transparent (I) photopolymer. Modeling of the side surfaces is also completed with enamel (A 1) and transparent composite, which is distributed taking into account the individual degree of transparency of the enamel: evenly along the entire perimeter of the restoration. At the cutting edge, the width of the transparent layer is 1.0 mm (Fig. 12).
Rice. 12. Imitation of a translucent cutting edge.
Immediately after the production of aesthetic structures, they are processed: the surface hybrid layer is removed (with bur No. H390S-018-FG, NTI) (Fig. 13), the relief is contoured, and occlusal contacts with antagonist teeth are verified.
Rice. 13. Contouring of aesthetic restorations.
Polishing is carried out with discs without significant pressure on the surface of the restoration, in the direction from the equator towards the cutting edge. To achieve shine, polishing heads containing fine aluminum oxide powder as an abrasive are used, sponges and polishing pastes are used (Fig. 14).
Rice. 14. Polishing the surface of the restoration.
At the final stage, odontometry is carried out: the vertical size of the teeth after restoration exceeds the horizontal ones and amounts to 9.7 mm and 9.8 mm for the right and left incisors, respectively, the teeth have acquired a rectangular shape (Fig. 15).
Rice. 15. Final odontometry: vertical tooth size 9.7 mm and 9.8 mm for the right and left incisors, respectively.
Finishing of proximal surfaces is carried out with strips - strips on a metal or plastic base with varying degrees of granularity of the abrasive material applied to them. The finished work is shown in Figure 16.
Rice. 16. General view of the finished restoration.
Illumination of teeth with short-wave light demonstrates the same spectral composition and fluorescence intensity of the filling material from which the half-veneers are made and the hard tissues of the tooth (Fig. 17).
Rice. 17. When illuminated with short-wavelength light, the restorations fluoresce in the same way as the hard tissues of the tooth.
The final stage of treatment is the treatment of the enamel surrounding the restoration with fluoride-containing preparations.
Quality assessment is carried out in accordance with the aesthetic quality index (EQI) [3]. The score is given separately for each of the 12 parameters presented in the table: 3 points - the result fully corresponds to the plan; 2 points - the result partially corresponds to the plan; 1 point - the result does not correspond to the planned one. Then all points are summed up. The highest possible number of points is 36.
Quality rating: 33-36 points - excellent; 29-32 points - good; 24-28 points - satisfactory; below 24 points - unsatisfactory.
Calculation of the aesthetic quality index (EQI):
EIC = n/36
where n is the total score; 36 - maximum score;
0.9-1 - excellent result;
0.7-0.8 - good result, minor correction of the restoration is needed;
<0.7 - unsatisfactory result, the structure needs to be replaced.
An assessment of the aesthetic restorations we performed showed: EIC = 1, which is interpreted as an excellent treatment result.
Table No. 1. Assessment of the quality of the manufactured structure according to EIK (aesthetic quality index)
Criteria | Intact, symmetrical tooth | Design | Score in points | |
| planned | manufactured | |||
| 1 | 2 | 3 | 4 | 5 |
| 1. Tooth dimensions: height (LCO2), mm | 8.9 mm | 9.7 mm | 9.7 mm | 3 |
| transverse size (MDCO2), mm in the cervical region | 8.9 mm | 8.9 mm | 8.9 mm | 3 |
| in the equator region | 8.9 mm | 8.9 mm | 8.9 mm | |
| in the area of the cutting edge | 8.9 mm | 8.9 mm | 8.9 mm | |
| 2. Geometric tooth shape: rectangular (square) | square | rectangular | rectangular | 3 |
| triangular | ||||
| oval | ||||
| 3. Crown angle sign: expressed not expressed | not expressed | expressed | expressed | 3 |
| 4. Sign of crown curvature (displacement of the point of greatest convexity): | 3 | |||
| mesially | ||||
| closer to the midline | ||||
| displaced distally | distally | mesially | mesially | |
| absent | ||||
| 5. Sign of root deviation: expressed not expressed | expressed | expressed | expressed | 3 |
| 6. Gingival contour: flattened | 3 | |||
| rounded | ||||
| domed | domed | domed | domed | |
| 7. Cutting edge: straight | straight | straight | 3 | |
| convex | ||||
| concave | concave | |||
| serrated | ||||
| 8. Relief of the vestibular surface: expressed | ||||
| not expressed | not expressed | not expressed | not expressed | 3 |
| 9. Degree of gloss of the enamel (presence of distortions): evenly matte | 3 | |||
| “matte” in the cervical area | ||||
| brilliant | shine | shine | shine | |
| 10. Type of tooth transparency: enamel is transparent in all areas of the tooth crown | 3 | |||
| pronounced transparency of the proximal surfaces of the tooth | ||||
| Only the cutting edge is transparent | ||||
| transparent cutting edge and proximal surfaces | + | + | + | |
| 11. Tooth color assessment using the VITA scale: in the cervical region | A 2 | A 2 | A 2 | 3 |
| in the equator region | A 2 | A 2 | A 2 | |
| at the cutting edge | A 1 + I | A 1 + I | A 1 + I | |
| on proximal surfaces | A 2 + I | A 2 + I | A 2 + I | |
| 12. The presence of individual characteristics of the tooth (stains due to hypoplasia, fluorosis, etc.) | — | — | — | |
| 13. Assessment of the quality of the manufactured structure according to EIK (aesthetic quality index) | n/36 | 36/36 = 1 | ||
Conclusion
The use of photocomposites in aesthetic dentistry makes it possible to expand the indications for dental treatment using therapeutic methods. In accordance with the basic requirements for aesthetic restorations, the main stages of treatment are carried out using light-curing materials, including the selection of optimal shades, modeling of restorations, and their processing. Efficiency is assessed in accordance with the aesthetic quality index, which reflects the main parameters of size, shape, surface topography, optical properties of the tooth and restoration.
Literature
- Lomiashvili L. M. On the way to creating the secrets of tooth shapes
/ L. M. Lomiashvili // Klin. dentistry. - 2006. - No. 2. - P. 12-15. - Lutskaya I.K. Fundamentals of aesthetic dentistry.
/ I. K. Lutskaya. - Mn.: Let's lie. school, 2005. - 332 p. - Criteria for assessing aesthetic restorations: instructions for use No. 078-0906:
approved.
Ministry of Health of the Republic of Belarus 06/26/2007 / I.K. Lutskaya, N.V. Novak, T.A. Zapashnik, V.P. Kavetsky // Modern methods of diagnosis, treatment and prevention of diseases
: collection. instruction—method. doc. - Minsk: RNMB, 2007. - T. 5. - Issue. 8. - pp. 75-79. - Nikolaev A.I. Physico-mechanical properties of modern filling materials: significance for practical dentistry.
III. Dry shine and strength of composites / A. I. Nikolaev, L. M. Tsepov, P. G. Adamov // Maestro of Dentistry. - 2003. - No. 3. - P. 28-32 - Pogorovskaya I. Ya. Comparative assessment in vitro of color indicators and color stability of composite and glass ionomer materials for aesthetic restoration of teeth
/ I. Ya. Pogorovskaya, I. M. Makeeva, E. A. Emilenko. - M., 2001. - P. 83-84.
Second lower premolar
Average age of teething: 11-12 years
Average age of root formation: 13-14 years
Average length: 22.3 mm
The second lower premolar, which is very similar in crown shape to the first premolar, has a less complex root.
Its crown has a well-developed buccal cusp and a much better formed lingual cusp than on the first premolar. The access is made slightly oval, wider in the mesial-distal direction. They begin to form access in the central sulcus with a fissure bur with a cutting apex, and then expand and form the contour of the burr hole with spherical burs No. 4 and 6.
Researchers reported that only 12% of mandibular second premolars studied had a second or third canal [17]. Vertucci [13] also showed that second premolars had one apical foramen in 97.5%, while only 2.5% of the teeth examined had two foramina.
An important circumstance that should not be forgotten is the anatomical location of the mental foramen and the vessels and nerves passing through it. Due to the proximity of these structures, an acute inflammatory process in the area of the lower premolars can cause temporary paresthesia. The exacerbation of the pathological process in this area is more severe and resistant to conservative treatment than in other areas.
Prevention
To prevent pathology, it is necessary to regularly visit the dentist for preventive examinations at least once every six months. It is also important to promptly replace dental defects. In addition, all experts advise correcting malocclusion pathologies in a timely manner already in childhood or adolescence. Orthodontic therapy will help cope with the abnormal position of the teeth and prevent wear of the crown part.
You won’t have to decide what to do when the hard tissues of your teeth are worn away if you treat all the diseases that lead to it. For example, this includes bruxism, mineral metabolism disorders, thyroid pathologies, and problems with the digestive organs.
If the patient is at risk due to professional activities, it is necessary:
- use personal protective equipment;
- take a responsible approach to regular hygienic oral care;
- take courses of vitamins and minerals prescribed by your doctor.
The most important point remains the qualitative diagnosis of the transitional stage between physiological and pathological erasure. For this purpose, regular examinations and timely treatment of identified disorders are indicated.
First lower molar
Average age of teething: 6 years
Average age of root formation: 9-10 years
Average length: 21.0mm
The mandibular first molar erupts earlier than other permanent teeth and most often requires endodontic treatment. It usually has two roots, but sometimes three roots are found, with two canals in the mesial root and one or two canals in the distal root.
The distal root is easily accessible for endodontic cavity preparation and mechanical treatment.
The doctor can directly see the opening(s) of the canal. The distal root canals are wider than those of the mesial root. Sometimes the mouth is wider in the buccolingual direction. This indicates the presence of two channels or a slit-like channel with a complex network-like configuration that can complicate cleaning and shaping.
The mesial roots are usually curved, with the greatest curve in the mesiobuccal canal. The orifices of the canals at the bottom of the pulp chamber are usually clearly separated from each other and located buccally and lingually relative to the upper tubercles.
The tooth often undergoes extensive filling. It almost always experiences a strong chewing load, so the coronal pulp cavity can be obliterated. It is easiest to identify the mouths of the distal canals.
Then the mouths of the mesial canals are found, which will be located in the above locations in the same horizontal plane.
Since the mouths of the mesial canals lie under the mesial tubercles, they may not be detected during normal cavity preparation. In this case, to determine their location, it is necessary to remove the hard tissue of the tubercle or filling. During access preparation, overhanging molar cusps need to be ground down [15]. Remember that this tooth, like all other lateral teeth, after endodontic treatment requires complete restoration of the entire occlusal surface area. Therefore, to identify anatomical landmarks and orifices, it is better to make a wider access cavity than to skip one or more channels for the sake of “sparing” preparation, which may cause failure.
Skidmore and Bjoradal [11] found that approximately one third of the mandibular first molars examined had four root canals. If there are two canals, “they either remain separate with separate apical foramina, or unite and form a common apical foramen, or communicate with one another by transverse anastomoses partially or completely... If the tooth, instead of the usual triangular shape, had a more rectangular shape, this would allow better vision and explore a possible fourth canal in the distal root.”
In the area of bifurcation of the roots of the lower molars there are several orifices of additional canals [9]. They are usually impossible to clean and shape, and are rarely visible except incidentally on radiographs when they are filled with root cement or heated gutta-percha during treatment. It would be correct to assume that if irrigation solutions tend to clean the canal from protein decomposition products, then the area of root bifurcation in the pulp chamber must be thoroughly cleaned (remove denticles, etc.) so that the solutions can reach the small mouths of the canals.
All infected dentin, leaking fillings, and pulp denticles must be removed before endodontic treatment begins. It is recommended to completely cover the cusps with a restorative structure after endodontic treatment.
Second lower molar
Average age of teething: 11-13 years
Average age of root formation: 14-15 years
Average length: 19.8 mm
The crown is somewhat smaller in size than the first molar, and the more symmetrical second lower molar is characterized by a close arrangement of roots. The roots gradually converge distally and have closely spaced apices.
Exposure is made at the mesial portion of the crown with access extending only slightly distal to the central sulcus. After trephination of the cavity with a fissure bur with a cutting apex, an elongated ball-shaped bur is used to expand it until free access is achieved. The distal root angles often allow for a smaller opening than the lower first molar.
Particular attention should be paid to the shape of the mouth of the distal canal. A narrow oval orifice indicates the presence of a slit-like lumen in the distal canal, which requires more careful treatment.
All carious tissue, leaking fillings and denticles should be removed and replaced with a suitable temporary filling prior to endodontic treatment.
The lower second molar is most susceptible to vertical fractures. After preparing the access, but before starting endodontic treatment, the clinician should examine the floor of the pulp cavity using fiber optics. For mesial-distal crown or root fractures, the prognosis is extremely unfavorable.
To avoid vertical fractures after endodontic treatment, it is necessary to completely cover the cusps with a restorative structure.