What is mandibular nerve injury?
By this concept, dentists mean injury to one of the nerves:
- chin;
- lingual;
- alveolar.
Types of injuries include sprain, compression, crushing and rupture - partial or complete. The cause of the stretching is the long-term retraction of the mucoperiosteal flap, which is created by an implant of greater length than necessary. Crush injuries and compression are caused by needle injuries during the administration of anesthesia. Rupture occurs in two cases: when cutting the mucosa or during preparation of the hole for the implant.
Treatment of a damaged nerve
Treatment for an injured mandibular nerve depends on the extent of the damage, which can be minor, partial, or severe.
- With minor damage, the patient experiences a slight loss of sensitivity, which recovers on its own within a month.
- Partial nerve injury is characterized by more pronounced symptoms, but sensitivity after it also recovers on its own. True, this requires much more time (at least 2 months), and the process is accompanied by painful sensations.
- The most serious degree of damage is a complete disruption of the integrity of the nerve, which is accompanied by degeneration: the tissue supporting the nerve is replaced by scar tissue, which can cause a person to permanently lose sensitivity.
Uncomplicated injuries of degrees I and II usually do not require surgical intervention - the doctor prescribes anti-inflammatory drugs to the patient, and sometimes an additional complex of vitamins B6 and B12. As for serious injuries, their treatment requires the services of a qualified microsurgeon.
In any case, if after implantation a person feels numbness or discomfort in the cheeks, lips or mouth, he should immediately consult a doctor. Any delay can have the most dire consequences - for example, after three months of complete loss of sensitivity, it can only be partially restored, and after a year, the dysfunction of the nerve will be irreversible.
Causes and prevention of mandibular nerve injuries
The only cause of such damage is considered to be medical errors. Since in preparation for implantation, X-rays of the jaw are taken, which the doctor must carefully study so that when choosing an implant and a place for it, he does not injure the nerve, the injuries are caused by his unprofessionalism or negligence.
Damage to the mandibular nerve most often occurs when:
- improper administration of anesthesia - needle injury;
- choosing an implant that is too long;
- damage by an instrument - when preparing the site for the implant.
The only way to avoid such an injury is for a doctor to responsibly approach the stage of preparation for surgery, carefully studying the condition and structure of his patient’s jaw. The only way of prevention for the patient is to choose a trusted clinic and a highly qualified doctor. Specialists at the Implantmaster clinic have been able to reduce the number of injuries of this kind to 2%, since they carefully study three-dimensional photographs of a person’s jaw before implantation, and can correctly assess the condition of the bone tissue, the location of nerves and blood vessels, and select the optimal size of the implant.
Factors influencing neurological response to nerve injury
— Preoperative screening for neuropathic pain is necessary. Preexisting neuropathic dental pain (PDAP type 1), which exists before surgery, can be caused by many different systemic conditions, medications, and other lesions. It is critical that surgeons recognize presurgical neuropathic conditions because neuropathic pain does not respond to surgery and can often lead to worsening pain. In addition, poorly controlled preoperative pain and nerve damage can cause chronic postoperative pain.
— The main indicators for predicting chronic post-surgical pain are psychological factors, including the level of anxiety, neuroticism (a fundamental personality trait in psychology, characterized by anxiety, fear, rapid mood swings, frustration and a feeling of loneliness. It is believed that neurotic people cope worse with stress and are prone to exaggerate the negative side of a particular situation.), catastrophization and introversion. Thus, the doctor has the opportunity not to perform the surgery of choice (implantation) in such patients, but to decide in favor of an alternative treatment plan.
- The concentration of the anesthetic used is up to 2% lidocaine - the accepted standard, because higher concentrations have a greater neurotoxic effect, which may cause permanent neuropathy. Avoid using multiple (repeated) anesthetic blocks in the same area for the same reason.
— Preoperative medical examination should exclude the following diseases : Raynaud's disease, Erythromelalgia (Mitchell's disease), Irritable bowel syndrome (IBS), Migraines, Fibromyalgia.
—Location of surgery is another factor associated with neurological response. Trauma in the distal jaw is more significant (eg, angle and ramus) than in the mental foramen, because the closer the proximal nerve injury is, the greater the risk of damaging trigeminal ganglion cells and initiating retrograde effects of differentiation into the central nervous system. .
Thus, a thorough interview and examination of the patient, detailed pre-implantation planning based on CBCT data, appropriate visualization of the implantation plan and the use of surgical guides, selection of optimal implant sizes with extended safety zones, use of drill limiters and, of course, an experienced team of doctors who will carry out the implantation followed by early postoperative care, all of which will contribute to safer practice and optimized patient outcomes.
Our team of doctors
Maxillofacial surgeon, Implantologist
Bocharov Maxim Viktorovich
Experience: 11 years
Dental surgeon, Implantologist
Chernov Dmitry Anatolievich
Experience: 29 years
Orthopedist, Neuromuscular dentist
Stepanov Andrey Vasilievich
Experience: 22 years
Endodontist, Therapist
Skalet Yana Alexandrovna
Experience: 22 years
Orthopedic dentist
Tsoi Sergey Konstantinovich
Experience: 19 years
Dentist-orthodontist
Enikeeva Anna Stanislavovna
Experience: 3 years
Symptoms and stages of damage
The symptoms by which this complication can be recognized are as follows:
- numbness of parts of the head - tongue, lips, chin, cheeks, etc.;
- biting lips and tongue;
- choking while eating or drinking;
- profuse salivation.
All this creates a number of inconveniences for the patient: it makes it difficult to eat and talk, disrupts facial expressions, and also prevents men from shaving and women from applying makeup. The severity of this injury is determined by its degree: a minor one goes away on its own or with the help of drug treatment, a severe one leads to irreversible processes of nerve degeneration and is not curable. Damage to the mandibular nerve, the symptoms of which the patient observes, requires immediate consultation with a doctor - only a specialist will be able to determine its extent and provide timely assistance.
Dentists distinguish the following stages of this implantation complication:
- minor - neuropraxia;
- more severe, but partial damage - axonotmesis;
- a serious injury that leads to complete loss of sensitivity - neurotmesis.
Inflammation of the trigeminal nerve after removal of a diseased tooth
It happens quite rarely that after getting rid of a bad tooth, people begin to feel acute pain in the nasal, eye areas, as well as in the temporal mandibular joint. Sometimes such pain can be caused by everyday habits. For example, brushing your teeth, applying makeup, etc. Even a light touch of your hands to your face can cause spontaneous pain.
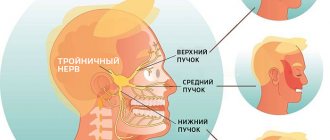
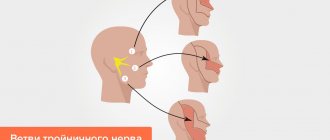
Such pain is harmful to human health, since any unexpected painful blow can immobilize a person for 2-3 minutes. All this is a manifestation of neuralgia, otherwise it can be called inflammation of the trigeminal nerve. The trigeminal nerve is the largest of the 12 cranial nerves, this nerve consists of 3 main branches: the orbital, mandibular and maxillary nerves, which are responsible for the sensitivity of the facial tissues, nasal mucosa, mouth, and for the proper functioning of the facial muscles.
The most famous pathology is inflammation of the trigeminal nerve. Inflammation of the trigeminal nerve is a chronic disease that affects parts of this area and is accompanied by pain in one part of the face. According to statistics, women aged 50-70 years most often suffer from such pain. Inflammation can occur due to hypothermia, infectious diseases, such as caries. Neuralgia also appears when there is a tumor in the brain. There is no need to be afraid, as in childhood, of having a tooth removed at the dentist. It is extremely rare that dental treatments lead to nerve inflammation; these are only exceptions. But on the Internet you can find a lot of dissatisfaction from people who were advised to treat inflammation of the trigeminal nerve when the cause of the pain was dental problems. Sometimes doctors mistakenly mistake pain symptoms for neuralgia, not realizing that the pain may be associated with diseases of the dental tissues. But remember that most often the pain “echoes” precisely in the neighboring teeth, so neuralgia is often confused with toothache.
So why can neuralgia appear after tooth extraction? If the diagnosis was incorrect, dental treatment could be performed instead of treating nerve inflammation. At the time when it was necessary to treat the nerve, the tooth was removed. Consequently, after which, the patient’s pain did not stop. And the person associated these painful symptoms with incorrect tooth extraction and poor quality work of the dentist. Either without removing the tooth, but undergoing long-term treatment, already with an inflamed nerve, the tooth can be severely injured, which is why neuralgia occurs. At first, such inflammation was related to dental treatment, but later it began to refer to neuralgia. No one can still say for sure the cause of inflammation. But many doctors believe that this is due to the pressure of an artery or vein on the nerve, which is why the change occurs.
How is trigeminal nerve treated? If you feel any pain in the facial part of your face, it is better to consult a neurologist. If a neurologist examines you and definitely says that the pain is not related to the nerve, but that the pain is caused by a bad tooth, only then go to the dentist. Treatment for inflammation is varied and varied. Your doctor may prescribe pain-preventing and pain-relieving medications. Acupuncture is also widely used (the essence of this treatment is the impact of thin needles on certain points on the human body). But the main method of treating neuralgia is surgery. Since pain is the main complaint of patients. And after the operation, the pain goes away forever or for a very long period. Today, there are many treatment methods, both surgical and traditional. To avoid pain in various parts of the body, if you feel the slightest discomfort, it is better to immediately consult a doctor so that he can identify your problem and prevent the development of the disease.
Recovery and treatment
In the first case, self-recovery takes approximately 1 month; the help of doctors is not needed, since there is no anatomical damage. Symptoms of the second appear after a while - usually 6-8 weeks, so recovery can be painful and incomplete: it will take more than 2 months. In the third stage of damage to the mandibular nerve, treatment gives results only at the beginning and is performed surgically, since we are talking about degeneration with a violation of integrity. Loss of sensitivity, which is observed in a patient for more than 3 months, indicates a high probability of losing it forever. Damage to the mandibular nerve, the consequences of which is the lack of sensitivity of the nerve for a year, leads to irreversible changes. Only the professionalism and responsibility of the doctor, which is guaranteed by the specialists of our Implantmaster clinic, can protect the patient from such unpleasant injuries.
Author:
On the issue of treatment of injury to the inferior alveolar nerve during dental implantation
Introduction
Currently, one of the most pressing and significant problems of modern dentistry is the treatment and prevention of injuries to the inferior alveolar nerve that occur during the installation of dental implants in the lower jaw. Damage to the inferior alveolar neurovascular bundle, which includes the inferior alveolar nerve, is possible if the protocol for performing dental implantation surgery is violated. This complication is observed in cases where the anatomical and topographical features of the structure of the lower jaw are not taken into account, namely, with an inadequate assessment of the existing reserve of bone tissue bordering the mandibular canal, as well as with the wrong choice of the size and shape of the implant.
If surgical intervention is performed without taking into account the age and individual characteristics of the structure of the mandibular canal, the risk of injury to the lower alveolar neurovascular bundle increases.
If the walls of the mandibular canal are damaged by an implant, clinical manifestations of neuritis of the inferior alveolar nerve are detected immediately. They manifest themselves in the form of bleeding and severe pain. If this complication occurs, the following measures must be taken: urgent removal of the implant, stopping bleeding, surgery to lateralize the inferior alveolar nerve. Anti-inflammatory therapy is prescribed.
When installing dental implants, an operation is performed to lateralize the inferior alveolar nerve. After anesthesia, a trapezoidal incision is made. The mucoperiosteal flap is detached. Using a physiodispenser, an osteotomy is performed in the middle third of the lower jaw in the form of an elongated window. The mandibular canal is opened. After which the inferior alveolar nerve is ligated and retracted to the side. A dental implant is installed. The bioresorbable material “Bio-oss” is placed, and the nerve is returned to its place. The autograft obtained during the operation closes the bone wound. The wound is closed with a resorbable membrane. The mucoperiosteal flap is placed in place and interrupted sutures are applied.
Since the autograft, which is cut out using a physiodispenser, is significantly smaller in size than the resulting bone window, the operation requires the mandatory use of bioresorbable materials to fill and cover the bone defect.
The disadvantage of this operation is that direct contact of the lower alveolar neurovascular bundle with osteoplastic material leads to nerve irritation, loss of protopathic sensitivity, impaired circulation in the inferior alveolar artery, hypoxia, prolonged hypo- and paresthesia of the lower alveolar nerve. There is no provision for isolating the wound from the oral cavity after surgery. Complications in the form of inflammation are possible.
Currently, traditional methods of treating injuries of the inferior alveolar nerve are removing the implant from the mandibular canal and prescribing a number of physiotherapeutic procedures in the postoperative period (ultraphonophoresis with hydrocortisone, Tribexol vitamin complex, etc.).
There is a known operation to remove filling material from the mandibular canal after endodontic treatment - “Method of rapid access to the mandibular canal.” This method eliminates irritation of the lower alveolar neurovascular bundle and reduces postoperative trauma. The procedure for performing the operation is as follows: after anesthesia and an incision, an osteotomy is performed by sawing the bone of the lower jaw with an ultrasonic device “Piezosurgery” with a frequency of three-dimensional vibration of 24-29 kNz at an angle of 45º, the filling material is removed from the mandibular canal, then the bone wound is washed with a 1% solution of dioxidine, processed through a 0.05% solution of miramistin for 5 minutes with a waveguide from an “Optodan” apparatus, with a semiconductor laser diode generating pulsed light with a wavelength from 0.85 to 0.98 microns, pulse power 2–4 W, pulse duration 40 –100 ns, with a pulse frequency of 1.5–2.0 kHz, magnetic field strength of 35 mT. The defect is closed with an autograft, a resorbable Parodonkol membrane, a mucoperiosteal flap, sutured with interrupted sutures and isolated with Diplendent film with metronidazole.
This method has a number of disadvantages: long-term paresthesia of the areas of the face corresponding to the innervation of the inferior alveolar nerve (skin of the chin, cheek, corner of the mouth), the absence in the postoperative period of complex therapy aimed at completely restoring sensitivity in the area of innervation of the inferior alveolar nerve with constant objective monitoring of electrical excitability indicators corresponding areas of the face.
Purpose of the work: to increase the effectiveness of treatment of injuries of the inferior alveolar nerve during dental implantation, including removal of the dental implant, restoration of sensitivity in the area of innervation of the inferior alveolar nerve in the postoperative period with constant monitoring of electrical excitability indicators of the corresponding areas of the face and dental pulp.
Materials and methods. 12 patients with perforation of the mandibular canal were operated on using a dental implant. The surgical technique is as follows: under anesthesia, an osteotomy was performed in the form of a bone window in the area of the body of the lower jaw, which is formed by sawing the bone with an ultrasonic “Piezosurgery” device with a three-dimensional vibration frequency of 24-29 kNz at an angle of 45º. The inferior alveolar nerve was lateralized using ligatures. A dental implant is removed from the mandibular canal. The bone wound is treated with a 0.05% solution of miramistin for 5 minutes using a waveguide device "Optodan" with a semiconductor laser diode generating pulsed light with a wavelength of 0.85–0.98 microns and a pulse power of 2–4 W, a pulse duration of 40– 100 ns, with a pulse frequency of 1.5–2.0 kHz, magnetic field strength of 35 mT. The wound is isolated from the oral cavity with Diplendent film containing metronidazole. Peripheral blood circulation in the area of injury was restored by using phonophoresis with a 0.5% hydrocortisone solution, amplipulse phoresis with 2% nicotinic acid, acupuncture at Balle points - at the points of entry and exit of the lower alveolar nerve from the lower jaw (Fig. 1), with measurement of electrical excitability indicators the corresponding areas of the facial skin and the pulp of adjacent teeth using the PARKELL device (model D624 with an error in measuring the current amplitude of no more than 5%, made by Parkell Elektronics Division, USA), which allows you to monitor the effectiveness of the treatment.