A small chin (medically called inferior micrognathia, or microgenia) is an incredibly common problem.
However, most people who can be confidently diagnosed with this have not only not heard such words, but also do not suspect that there is anything wrong with them. They are healthy, everything is in place. But no matter how hard they try to achieve an ideal appearance, it doesn’t work!
Neither losing weight, nor taking care of your face, nor changing your hairstyle helps. It's not clear what's going on! As a result, people either come to terms with the fact that everyone is imperfect, or they suffer all their lives because the ideal is unattainable for them personally.
Description of the pathology
The normal shape of a row of permanent teeth resembles an elongated horseshoe. The lower jaw is naturally slightly narrower than the upper jaw - this is necessary for better closure of teeth and chewing food.
Narrowing of the jaw is called its reduction in diameter - the appearance of a “dent”. This happens more often with the top than with the bottom. It is formed by more porous bone and is more closely connected in the patterns of its development with the upper palate and other elements of the skull. But in fact, the process can affect both jaws, only the right or left side of one of them, or even both.
Another weak but obvious pattern is the increased frequency of curvature in the premolar area (4-5 teeth on each side), while “concave” anterior teeth are less common.
Using the example of orthognathic operations, you can see that often two people fight for the patient’s correct bite, his good health and harmonious facial features - the orthodontist and the maxillofacial surgeon.
And to carry out a successful orthognathic operation, it is necessary that the rows of the patient’s teeth are straight - this is what the orthodontist does during almost six months of preoperative preparation. But what to do if the rows of teeth cannot be aligned using conservative methods, for example, due to a pathological anomaly such as micrognathia?
Micrognathia is a congenital or acquired underdevelopment of the jaw bone. There are upper and/or lower micrognathia, as well as unilateral and bilateral.
A too narrow jaw will not allow the formation of a healthy dentition. And if patients in childhood and adolescence can still be helped without resorting to surgery - using special expanders, then for adults whose growth of the facial bones has already completed, surgery may be the only chance to correct the bite. The method is based on stretching a blood clot formed between osteotomized fragments of the jaw, which gradually undergoes mineralization and ossification - turns into bone tissue.
Depending on the type of anomaly, the patient may be indicated for surgical expansion of the upper dentition, much less often - the lower one, and combined surgery on both jaws is often required. The operation to expand the upper jaw is quite simple: the patient is given endotracheal anesthesia, after which the surgeon gains access through the oral cavity, making a small incision under the upper lip, and, exposing the body of the jaw, performs an osteotomy - a cut along the Lefort I line and along the median palatal suture. As a result, you get two movable fragments, which will be moved away from each other by the intraoral distractor. It is installed at the last stage. When performing surgery on the lower jaw, the distractor is fixed in the area of the dentition. Correction of an accidentally displaced distractor or its replacement does not require general anesthesia and is performed under local anesthesia.
A distractor, a distraction device, is a mechanical device made of medical titanium, designed to gradually, measurably and controllably stretch the facial bones of the skull.
The first 5-7 days after the operation there is a rehabilitation period - during this time a blood clot and a primary callus are formed along the midline of the osteotomy area. The distractor is then activated by the doctor - typically expanding by 1 millimeter per day, and the patient can perform this painless procedure themselves. This speed is necessary to ensure that bone tissue, and not connective tissue, is formed at the cut site. At this time, it is necessary to carefully observe the regime of unwinding the device, as well as personal hygiene - titanium should be cleaned with a soft toothbrush.
A sign of a correctly performed operation is the appearance of a diastema - a gap between the front teeth. After activation is completed, the device remains in the oral cavity for at least another three months - the time required for the patient’s expanded jaw to fully form. Once the distraction device is removed, you can begin to straighten your teeth using braces or orthodontic trays. And subsequently, if required, to carry out orthognathic surgery.
Varieties
This disease has several variants.
- Narrowing of the dentition along the entire length. Its typical sign is the appearance of a “horse” smile due to the fan-shaped incisors.
- Trapezoidal deformity. With it, the patient's jaw takes on the shape of a trapezoid with clearly visible visually defined angles in the area of growth of the 3rd incisor or 1st premolar.
- Narrowing in the anterior region. Here the incisors converge like a wedge and “climb” onto each other.
- Saddle defect. With it, the row is “dented” inward at the level of the premolars (4 and 5 units on each side) with 6 and/or 7 molars. And the incisors and “eights” are usually positioned correctly, or they may be moderately crowded and rotated.
- Asymmetry. This depression is observed only on one side, but, as a rule, affects both jaws. Often combined with normal occlusion in other areas.
All of them can be I, II or III degrees of severity. The pathology first appears in childhood, as temporary teeth are replaced with permanent ones. In adolescence and adulthood, consolidation of malocclusion leads to a change in the load on the mandibular joint, spreading secondary deformations to healthy areas.
The narrowing of the upper jaw is also accompanied by a deepening of the palatine vault and makes nasal breathing difficult. Plus, these processes provoke uneven wear of crowns and can lead to underdevelopment of units that do not have enough space.
Micrognathia - symptoms and treatment
Almost every type of dysgnathia and micrognathia is accompanied by very specific and noticeable functional and aesthetic disorders. These include all cases of malocclusion: from mesial, when the lower teeth protrude forward relative to the upper ones, to any variants of distal occlusion, in which the lower row of teeth is much behind the upper row. Such malocclusions are always accompanied by certain negative manifestations:
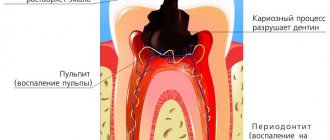
- from the teeth: abrasion, carious lesions, periodontal diseases;
- from the dentition: crowding and compensatory disorders (narrowing of the dentition and its curvature);
- from the temporomandibular joints: pain, clicking, crepitus (crunching sound), limitation of movements.
With skeletal disorders associated with a decrease in the upper respiratory spaces due to the small size of the supporting structures of the upper and lower jaws, a frequent manifestation of the pathology is breathing obstruction syndromes during sleep, for example sleep apnea.
Obstructive sleep apnea is a potentially life-threatening condition. It is characterized by snoring and repeated cycles of cessation of breathing during sleep. Most often, the pathology is associated with a narrowing of the respiratory space caused by improper bite and position of the jaw bones. In addition to snoring with pauses in breathing and night pain in the chest area, sleep apnea is accompanied by a decrease in oxygen levels in the blood, severely fragmented sleep, excessive daytime sleepiness, migraines and irritability.
Despite the listed functional disorders, the most significant clinical manifestation of dysgnathia and micrognathia is the aesthetic component . It is dissatisfaction with the smile and face that forces patients to seek medical help. While the intervention of an orthodontist and/or orthopedic dentist is often sufficient to correct a smile, the help of an oral and maxillofacial surgeon is necessary to restore the aesthetic balance of the face [11].
The main signs of severe underdevelopment of the jaw can usually be seen with the naked eye. These include:
- disproportionate features, distortion of facial contours;
- malocclusion;
- retraction of the upper or lower lip;
- a slanted (“bird-like”) or protruding chin;
- wrinkled skin of the chin, etc.
Severe micrognathia is clearly visible from the outside, but in the early stages only a doctor can diagnose underdevelopment of the jaw bones.
Causes
The most difficult reason in terms of prevention and treatment for a narrowing of the upper or lower jaw by 2 teeth or more (II degree and higher) is unfavorable heredity, since most of the structural features of the skull are determined at the genetic level. But other factors related to childhood also make a significant contribution:
- delay in introducing complementary foods;
- habit of thumb or pacifier sucking;
- early loss of baby teeth, especially molars or several units in a row on one side (the lack of chewing load in this area interferes with bone development);
- lack of solid food in the diet;
- metabolic disorders - rickets, type I diabetes mellitus, etc.;
- parafunction (unjustified increased activity of a nervous nature) of masticatory or facial muscles, including bruxism, involuntary movements of the tongue, etc.;
- rhinitis, sinusitis, tonsillitis, polyps and other diseases that force the child to breathe more often through the mouth than through the nose;
- injuries.
It can also be provoked by a cleft palate, caused by a delay in intrauterine development.
Diagnostics
It is not difficult to determine the narrowing of the jaw in a child or adult during an external examination. Its clear sign is the “pressed-in” dentition in certain areas or along the entire length with partially expanded, crowded units. Another characteristic feature is malocclusion.
At the same time, it is necessary to distinguish pathologies of jaw development from atypical orthodontic and dental situations such as supernumerary units, macrodentia, individual structural features of the skull, etc. They can also be combined. Therefore, a preliminary diagnosis made visually is confirmed with the help of one or more additional studies:
- According to Pon-Linder-Hunt , where the difference between the normal and existing width of the dental arch for a given patient is calculated using a special formula. The method requires taking several measurements directly in the oral cavity and taking into account different indicators for representatives of individual nations. But it gives the attending physician a fairly accurate answer to the question of whether several units will have to be removed to level the entire row.
- According to Howell-Gerber-Gerbst - another relatively complex mathematical scheme that is well suited for measuring the shape, length, width and other individual parameters of a row.
- Teleradiography is a type of X-ray examination that allows you to take a picture of the entire skull. It gives a detailed picture of the deviation itself and reveals its causes, if they are embedded in the structure of other bones.
- Anthropometry is an accurate three-dimensional cast, on which it is easier to take the necessary measurements, especially when the upper or lower jaw of a child is narrowed.
- X-ray - used to assess the condition of the upper palate and its suture, bone structure.
- Orthopantomography - a classic frontal image, is now increasingly being replaced by CT (computed tomography) due to its improved clarity and expanded capabilities - such as obtaining 3D images.
In combination, these methods allow the orthodontist to study the current condition of the bone, the degree and direction of deformation when narrowing the upper and/or lower jaw.
When choosing a correction method, it is also important that they provide an opportunity to evaluate the resource for moving teeth into the correct position and straightening the bite.
Reasons for formation
A child’s jaws are formed under the influence of the chewing muscles, tongue and facial muscles. Failure in their functioning can lead to pathological changes in the shape and dimensions of the arches.
Factors that provoke narrowing of the jaws:
- loss or removal of milk units;
- late introduction of solid foods into the diet;
- osteogenesis disorder;
- sucking of thumbs, tongue, cheeks;
- mouth breathing;
- genetic predisposition;
- general pathologies.
Diagnostic methods
Dental pathology is manifested by a variety of clinical symptoms that make diagnosis difficult. An experienced dentist is able to make the correct diagnosis after a clinical examination. Sometimes additional diagnostic measures are required:
- Radiography. A photograph of the palate allows you to assess the condition of the palatal suture.
- Teleradiography. Lateral shot of the face and jaw.
- Orthopantomography. Panoramic photo of the dentofacial apparatus.
- Anthropometry. Study of a model of jaws made of polymer or gypsum.
- Pon's method. Determination of the individual norm of the width of the dental arches.
- Howley-Herbst diagram. A graphical method that consists in constructing a jaw arch based on the width of the frontal and lateral incisor and canine.
Indications for expansion
The row expansion procedure is advisable in certain clinical situations:
- Narrowing of the HF row with symmetrical crossbite.
- Defects of the face and the relationship of its parts.
- Incorrect position of units or groups.
- Anomalies of occlusion.
- Difficulty breathing through the nose due to the deepening of the palate.
- Injuries to the mucous membranes from incorrectly located elements.
- Inflammatory processes in the periodontium.
- Dysfunction of the dentofacial apparatus.
- Congenital maxillofacial defects.
- Limited row space.
Orthodontic devices
Correction is carried out using removable and non-removable mechanical devices. In children with a mixed occlusion and an alveolar type of narrowing of the upper jaw, removable structures are used to expand up to 4 mm.
For mechanical expansion, the screw is turned a quarter turn weekly. The expansion should not exceed 1 mm per month. The expansion of the arch occurs through the alveolar inclination of the masticatory units. There is no rupture of the palatal suture.
If expansion of more than 4 mm is required, the palatal suture must be opened.
In children under 16 years of age, orthodontic treatment using palatal suture rupture is effective in almost 100% of cases. The expansion process can be slow or fast. In the first case, the screw is activated once every three days, in the second - twice a day. It is prohibited to use the quick method in persons with weak periodontal disease.
Derichsweiler apparatus
A compact non-removable orthodontic structure consisting of a metal frame, a screw and bushings attached to the chewing units. The product is designed to correct the entire length of the HF. It is used in children at the end of the mixed dentition or in the permanent dentition. Has a strong effect on bone tissue.
Expansion plates
A gentle treatment option for correcting pathology in temporary or mixed dentition. The design fits tightly to the sky, reproducing its shape. It is connected to supporting units using clasps.
Operation
Surgical treatment is carried out in complex clinical situations and consists of three stages:
- Orthodontic treatment.
- Operation.
- Correction using orthodontic appliances.
Depending on the clinical indications, the surgeon performs tooth extraction or perforation of the jawbone.
Treatment in children
The optimal age for correcting a narrowed jaw in children is from 6 to 15 years. For violations limited to the apical base and alveolar process (the area of root growth and placement of their holes), braces are recommended. They will align their row in conditions when the rest of the chewing apparatus is formed correctly.
If the pathology affects the entire jaw or palate, removable or permanent plates are prescribed. They consist of a plastic or silicone base with expansion screws in the center. They are fixed using a system of arms, brackets and locks to give the correct position to the displaced units. If it is necessary to correct a deep bite, cross bite, etc., two-jaw structures with cheek shields are used.
In each individual case, the elements of the plate are determined and adjusted individually, using casts. Only the rigid frame and screws remain unchanged, which must be expanded by approximately 0.25 mm every 4 days. The advantages of the plates are:
- wide frame color options;
- low visibility to others;
- mild impact on target structures.
Their low cost may also be an important argument. It rarely exceeds 10 thousand rubles, while the price of individual brace systems varies between 50-100,000 (ligatures made of plastic or precious metals, respectively). Plus, removable models are easy to care for and make it easier to maintain oral hygiene after eating. But when prescribing such plates to children, more control is required from parents.
The time of wearing them should be at least 20 hours a day, and the child is unlikely to comply with it himself due to the discomfort that persists even after the appearance of the habit.
Treatment options in adults
For patients over 18 years of age or with complex curvatures, more or less extensive surgical solutions are recommended. The simplest methods of treating narrowing of the upper jaw in adults:
- Installation of the Derichsweiler apparatus - a beam screw design for the upper jaw only. He breaks the palatal suture and sets its bones in a new, wider position. Then the teeth are straightened with braces.
- Normalization of the bite by removing several units in a row (in the vast majority of cases, the first premolars, 1 on each side). The method allows you to correct the bite and aesthetics of the smile without treating the narrowing of the jaw itself, if it is impossible or not necessary. Extracted premolars are not always redundant. But due to them, space is freed up for the remaining ones, and their location is again leveled with the help of braces.
In the case of the lower jaw, the layer of gum tissue is lifted, the bone is drilled in several places and the holes are connected with grooves. An expander is installed in them, with which the patient with a narrowing will need to go through several years, and the mucous membrane is returned to its previous position. This procedure is called jaw perforation.
When is jaw expansion performed in adults and children?
Orthodontics recommends wearing fixed expanders or jaw surgery in cases where this is the only effective and safe option to correct the bite. The main indications for expanding the upper jaw or lower dentition are:
- Micrognathia is insufficient development of the jaw. The disease is often congenital or appears during a period of intense bone tissue growth. The causes of the disease are injuries, genetic predisposition, rickets, defects in bone formation, endocrine pathologies;
- Abnormal narrowing of the dentition, when correction is possible only through orthodontic treatment.