What does dental pulp consist of?
Anatomical structure of the dental pulp
From an anatomical point of view, the tissue is divided into two zones. The coronal dental pulp has a loose structure and is involved in dentinogenesis; all layers of the dental pulp in this part are penetrated by an extensive network of capillaries and nerve cells. The root pulp of a tooth is denser because it does not contain a large number of cellular elements, but is saturated with collagen fibers. Through the apical foramen, the canals communicate with the periodontal tissues and allow minerals and nutrients to reach the tooth walls.
The pulp and dentin of the tooth form a strong complex - the hard tissue protects the tooth pulp from external irritants, and it, in turn, helps the formation of dentin.
The pulp of the front tooth smoothly passes from the crown to the root part, the dental pulp of the molars has clear boundaries - the mouths of the dental canals.
Histological structure of dental pulp
The pulp contains a large number of different elements:
- Elastin and collagen fibers supply the organ with hyaluronic acid, reducing susceptibility to toxins and bacteria.
- Odontoblasts and stellate cells are responsible for the regeneration of dental pulp.
- Leukocytes, lymphocytes and fibroblasts support the vital activity of the epithelium and organize communication between cells.
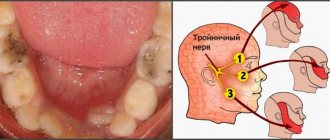
- A branched network of nerve processes forms Rashkov's plexus and provokes the occurrence of pain sensitivity when exposed to stimuli - the innervation of the dental pulp occurs due to the trigeminal nerve.
- Vessels and capillaries provide the blood supply to the dental pulp, which is necessary to nourish the tissues.
Composition of dental pulp
The fabric is 74% water, the remainder being organic and inorganic layers. Pulp cells include protein compounds, acids, lipids, glucose and various enzymes, which allows the epithelium to actively consume and process oxygen.
Many people mistakenly believe that the pulp is a nerve. The opinion is incorrect, since in addition to nerve plexuses, the tissue contains blood vessels and collagen fibers. |
Odontoblasts
Odontoblasts are tall prismatic cells that line the crown cavity (CC) like an epithelial layer. The nucleus with a prominent nucleolus is located basally. The cytoplasm includes numerous filamentous mitochondria, a well-developed granular endoplasmic reticulum and a very large Golgi complex, from which vacuoles with layered contents are separated, accumulating towards the apical pole of the cell, where they are finally transformed into granules with osmiophilic contents. The contents of the vacuoles, released by exocytosis, are precollagen and predentin proteoglycans. Some granules are released into predentin and are transformed into dentin matrix vesicles (DVs), which begin the mineralization of dentin. Well-developed occlusive zones (33), zonulae occludentes, provide strong connections between odontoblasts.
A very long and often branched process, called Toms' fiber (Tf) , arises from the apical pole of each odontoblast.
In predentin, Thoms fibers are surrounded by a plexus of collagen microfibrils (see arrows), and in dentin they continue in the dentinal tubules (DT) to the dentinocemental and dentinoenamel junctions. Immediately after leaving the apical poles, Toms' fibers give off thin lateral branches (B), which are poorly visible in a light microscope. The fibers and their branches are surrounded by mineralized peritubular dentin called Neumann's membrane (NE). Thoms fibers and dentinal tubules provide transport of nutrients into dentin.
Although odontoblasts form a complex of closely related cells, they do not form an epithelial layer, since they do not have a basement membrane and are abundantly supplied with numerous blood capillaries (Caps), surrounded by their own basement membranes (BMs). Nerve fibers (NF) pass between the odontoblasts and accompany some of the Thoms fibers in the dentinal tubules. This partly explains the sensitivity of dentin.
The function of odontoblasts is to produce dentin throughout a person’s life, causing a progressive reduction in the tooth cavity.
Age-related changes in dental pulp
The pulp of temporary and permanent teeth has a similar structure and only becomes thinner over time. Before the roots are formed, the pulp of a baby tooth is concentrated in the coronal part. Later, the tissue begins to spread into the dental canals through the apical foramen and grow into a wide network. The dental pulp in a child has a massive and dense structure, as well as a large fiber size.
The development of dental pulp continues throughout life, but with age, regeneration processes slow down: the number of active cells decreases, which leads to vascular fragility, insufficient tissue nutrition, the tooth suffers from odontoblast atrophy, that is, the impossibility of dentin formation. The described changes apply to older people.
Tooth structure
If you look at a tooth in cross-section, it is represented by the following tissues (from the periphery to the center): enamel, dentin, cementum and pulp. It is supported in the socket by alveolar bone, gums and periodontal ligament.
The part of the tooth visible in the mouth is called the dental crown, and the parts below it, located in the gum and bone, are called the neck and root. The neck is the slightly narrowed part of the tooth surrounded by gum. The root is immersed in the dental alveolus. On top of it there is an apex radicis or apex, where the hole is located: through it the neurovascular passes into the tooth.
Functions of the dental pulp
The main role of the pulp is to perform several tasks to support the vital functions of the tooth.
- Plastic function.
Formation of basic dentin, as well as the formation of hard tissue in case of damage. - Protective function.
Preventing infections from entering the periodontium through canals, removing dead cells, maintaining regeneration processes. - Sensory function.
A signal about the presence of an external or internal irritant to preserve tooth health. - Trophic function.
Supply of nutrients to dentin and tooth enamel.
Functions
The main tasks performed by the pulp are:
- protective;
- sensory;
- plastic;
- trophic.
It is the pulp that is responsible for the proper development and growth of the future tooth germ and further formation. With the help of this organ, mass and thickness increase throughout the entire period of life. Without pulp, normal tissue nutrition does not occur; the release of antioxidants and other substances is responsible for hardness and protection. One of the most important functions is also sensory, that is, the transmission of signals about the state of tissues, pain at the onset of the development of inflammatory processes.
What can cause pulpitis?
Burn of tooth pulp
As a rule, a pulp burn during tooth grinding occurs as a result of medical error or carelessness. Before prosthetics, the crown part is treated at high temperatures. Insufficient cooling during the preparation process can lead to a burn, which will provoke subsequent inflammation of the dental pulp.
Dental pulp hematoma
After a tooth injury, there is a possibility of getting a hematoma, that is, bleeding into the dentin. The crown acquires a reddish tint and painful sensations occur when pressure is applied. However, a bruise that has not turned into pulpitis or necrosis does not need treatment and goes away on its own over time.
Caries
Through the smallest cracks in the tooth cavity, infection and pathogenic bacteria penetrate into the pulp. Advanced caries is one of the most common causes of pulpitis.
Any damage or complications of diseases can lead to disastrous consequences if left untreated. Dental pulp necrosis is the process of tissue death due to the spread of infected cells. The anomaly can be recognized by the grayish color of the tooth and incessant aching pain. During treatment, the doctor will perform depulpation, clean and seal the canals. |
Pulp diseases
There are three stages of pulpitis: reversible, irreversible and tissue necrosis. Let's take a closer look at these pulp diseases.
- There are cases when inflammation of soft tissues is caused by the presence of a constant irritant. For example, the disease can be caused by mechanical trauma, pulp hyperemia, incorrectly installed filling, or chemical burn. If the pain immediately goes away after removing the irritant, such pulpitis can be considered reversible.
- A constant inflammatory process, the pain in which does not stop and only becomes stronger over time, means the presence of acute irreversible pulpitis. This kind of pulp disease is most often caused by the presence of an infectious focus and it can only be treated by depulping the tooth.
- Pulp necrosis, or pulp death, is most often caused by severe trauma, chemical exposure, or increased bacterial growth in the affected area. Often there are no painful manifestations during necrosis, but the tooth itself gradually darkens, changes color and loses its shine. Such a tooth can only be cured by removing necrotic tissue, cleaning and filling the canals, and then installing a crown on the damaged tooth.
To avoid all the problems described above, do not forget to regularly visit your doctor for preventive examinations, and also do not develop acute painful conditions into chronic ones.
Therapeutic methods for treating dental pulp
Therapeutic or conservative are methods of treatment that make it possible to do without removing tissue. These methods of preserving dental pulp are not available to all patients; there are certain indications:
- age not older than 40 years;
- deep caries;
- acute serous-purulent or fibrous pulpitis;
- opening of the dental pulp due to trauma;
- lack of medical intervention in the inflammation process to date.
As a rule, the dentist treats the surgical field with antiseptic solutions, removes the affected tissue and places the drug into the cavity. There are two methods for performing this procedure.
- Indirect covering of the dental pulp.
An antibacterial agent is placed at the bottom of the cavity to stimulate the production of bone substance. Regeneration occurs naturally. - Direct covering of the dental pulp.
The medication is applied directly to the soft tissue to preserve the viability of healthy cells, then isolated with a pad.
Next, the tooth is restored with temporary materials, and after a secondary examination, it is finally restored.
Histological analysis of the pulp in correlation with the carious process of varying depth
Determination of the inflammatory process in the pulp of primary teeth, caused by the development of caries, eludes clinical and radiological examination. Establishing an accurate diagnosis and identifying the inflammatory status of the pulp tissues in primary teeth allows us to select the correct treatment and ensure the success of restorative and endodontic therapy. This is especially important when working with young patients, since the limited ability to cooperate with them greatly complicates re-treatment.
Pulp inflammation in carious primary teeth is classified according to clinical signs and symptoms. However, in young children this inflammation cannot be absolutely reliable. Thus, we must rely largely on radiographic data. And the only unambiguous way to determine the status of pulp inflammation is histopathological examination.
Treatment of caries in children is not very simple due to unclear objective data that are necessary to make a correct diagnosis. And all manipulations on baby teeth must be justified and justified. All possible techniques such as indirect pulp capping, pulpotomy, pulpectomy and extraction must be justified by the presence of certain inflammatory changes in the pulp. Currently, there is insufficient literature on the correlation of signs, symptoms and histopathological status of the pulp in caries of primary teeth, which raises the problem of choosing the right treatment method.
Therefore, the present study aims to evaluate data on the histopathological status of the pulp obtained from the study of the second primary molar involved in the caries process. Histological parameters correlate with clinical and radiological data.
Materials and methods
A simple pilot study was conducted on 44 children aged 6 years and younger without serious general health problems. The study was conducted at the University Dental Hospital Sharjah (UDHS). The selected teeth were suitable for restoration and had less than 1/3 root resorption with no radiographic evidence of calcification, internal or external resorption. Upper and lower second primary molars with caries on the occlusal (22 teeth) and contact (22 teeth) surfaces. The study was conducted after obtaining approval from all necessary committees in accordance with the Declaration of Helsinki. The children's parents were informed about the study and gave written consent.
Children found themselves at the pulpit 2 weeks after the first signs of pain. Nine children reported 2-3 days after the onset of pain, and the remaining participants reported persistent pain for more than 10 days. Clinical examination of the selected teeth showed relatively strong hard tissue and healthy surrounding gingiva. Intraoral targeted radiography was performed to determine the percentage of caries involvement, total hard tissue thickness, residual dentin density (RDT), and periapical pathology. All indicated indicators were determined on a scale and then verified by an independent researcher, so all data can be considered accurate and reliable. The depth of caries was assessed as a percentage of the total dentin thickness.
Clinical procedures included local anesthesia, rubber dam isolation, removal of carious tissue, opening of the pulp chamber, and amputation of the coronal pulp with a spoon elevator. The bleeding was stopped by pressing a cotton swab soaked in saline solution for 5 minutes. After which the root pulp was removed using pulp extractors. After the pulpectomy procedure, tooth restoration was performed in one visit. The removed pulp tissue was placed in a 10% buffered formalin solution and sent for histopathological examination.
Pulp tissue samples were embedded in paraffin and then cut. Preparation for painting was carried out in two stages. The cut ran parallel to the longitudinal axis to a thickness of 5 mm. Hematoxylin-eosin was used for staining, which helps determine the type of inflammatory cells, vascular proliferation and fibrosis. To confirm the hematoxylin-eosin staining data, Masson trichrome staining (for fibrosis) and immunohistochemistry for CD (cluster differentiation) 45 leukocyte antigen and CD 34 endothelial marker (DAKO, Denmark) were performed. The degree of pulp inflammation for CD45 was defined as follows: 0=normal, + (mild) 1-50 cells/20 HPF, ++ (moderate) 51-100 cells/20 HPF, +++ (severe) >100 cells/20 HPF . CD34 was defined as + up to 50 blood vessels with inflammatory infiltrate/20 HPF, ++ 51–100 blood vessels with inflammatory infiltrate/20 HPF, and +++ > 100 blood vessels with inflammatory infiltrate/20 HPF. Lymphocyte counting was performed using an Olympus BX51 microscope (Hamburg, Germany). The extent of fibrosis is respectively labeled as mild, moderate, and extensive based on collagen density in Masson trichrome-stained sections. The number of cells/20 HPF was counted by an assistant, and accuracy was checked by repeat counting after a period of time. The obtained data were analyzed by Student's t-test to compare histological types of inflammation with clinical parameters. P<0.05 was accepted as significant.
results
The children were 6 years old or younger. An assessment was made of 22 teeth with occlusal and contact caries. The extracted pulp from the upper and lower primary second molars of 44 children was prepared and sent for histological analysis. A correlation was made between histological data and clinical parameters.
The results showed different histological conditions of the pulp depending on the degree of carious lesions of the occlusal or contact surfaces. All samples were grouped depending on the nature of the inflammatory process. Group A was a focal or diffuse inflammatory infiltrate consisting primarily of neutrophils interspersed with varying numbers of lymphocytes, plasma cells, and occasional eosinophils (Figure 1). The remaining groups (B1, B2 and C) showed mild to severe chronic inflammation represented by lymphocytes, macrophages, plasma cells along with blood vessel proliferation and varying degrees of fibrosis (Figure 2). Groups B1, B2 and C were divided based on the extent of fibrosis and angiogenesis. Histological parameters of the coronal and root pulp were the same in all cases except group A. In group A, severe acute inflammation was detected in the coronal and relatively moderate in the root.
Photo 1: Histological sections from group A showing signs of acute inflammation in the form of infiltration of neutrophils, varying numbers of macrophages, lymphocytes and plasma cells scattered around dilated blood vessels (a: hematoxylin-eosin staining/20 HPF Olympus BX51) and the same section stained CD45 antigen staining (b)
Figure 2: Histological sections from group B with chronic inflammation represented by moderate infiltration of lymphocytes and plasma cells, angiogenesis and fibrosis (a: hematoxylin-eosin/20 HPF Olympus BX51 stain) and the same section stained with leukocyte antigen CD45 (b) stain CD34 of blood vessel endothelium (c) and fibrosis stained with Masson trichrome (d).
In nine cases, when patients were examined 2-3 days after the onset of pain, signs of acute inflammatory changes were found, while in the remaining cases, except one, the pulp passed into the stage of chronic inflammation.
All children who sought help complained of pain, while healthy gum tissue was clinically determined, and tooth mobility in all cases was within physiological limits. Spot radiography revealed minimal changes in the periapical tissues. Carious lesions >80% and residual dentin thickness <1 mm were associated with varying degrees of pulp inflammation. We did not find any significant difference (p>0.05) between the histological type of inflammation and the clinical parameters assessed in this study.
Discussion
Histopathological examination was performed on pulp collected from primary second molars of children less than 6 years of age. The age criterion was chosen in order to completely exclude the influence of physiological resorption on the development of the inflammatory process.
Teeth in which pain was characterized as spontaneous were selected for the study. While the criterion for selection during examination in the oral cavity was healthy gums and dense hard tissues, which could indicate the vitality of the tooth. X-ray examination helped to exclude such pathologies as internal and external resorption, as well as calcification of the pulp chamber.
The pulp of the selected teeth was then sent for histopathological examination. Next, the samples were divided into groups according to the type of inflammation: acute and chronic. We observed histological signs of pulpitis in all cases. In 10 cases it was acute pulpitis, in the rest - varying degrees of chronic inflammation. The nature and severity of inflammation was similar in the coronal and root pulps in 40 cases, however, in 4 cases, acute severe inflammation was recorded in the coronal pulp and only moderate inflammation in the root pulp. For the first time in this study, we report that the histological type of inflammation (acute or chronic) influences the development of certain symptoms and clinical presentation.
All selected teeth exhibited symptoms of pain from irreversible pulpitis, intraoral examination revealed healthy gingiva, and tooth mobility was within physiological parameters. Thus, the children who took part in the study suffered from acute and chronic pulpitis, the form of which depended on the age of onset of the disease. Lack of mobility and swelling of the gums were criteria for excluding non-vital teeth from the study. The presence of periapical changes indicated the transition of infection from the coronal pulp to the furcation zone and the beginning of microscopic root resorption.
X-ray assessment of the extent of the carious process on the occlusal and contact surfaces showed from 80 to 100% of the total dentin thickness, which histologically corresponded to an acute inflammatory process in 10 images and a chronic one in the rest. The data obtained are in agreement with previous studies comparing the response of the pulp to the carious process. RDT was between 0.25 mm and 1 mm in 24 samples; in other cases, the carious process penetrated into the pulp chamber. The RDT score was used as an objective assessment of the likely pulpal response. We noted that the RDT value in this study was associated with inflammatory changes in the pulp tissue.
Correlations of the clinical manifestation of caries in the form of a cavity of 1-5 mm histologically corresponded to acute and chronic changes in the pulp. It should also be noted that caries assessed radiographically in 80% of cases clinically appeared less widespread. Thus, only a clinical assessment of a carious cavity cannot be considered a reliable guide for choosing a treatment method; in addition, it is necessary to evaluate the x-ray picture and clinical manifestations. It is also interesting that a 1 mm defect in the proximal zone in two clinical cases was associated with acute inflammation, which may indicate rapid progression of caries in a very short period of time.
The correlation of histological parameters with clinical manifestations confirmed the validity of the chosen treatment method (pulpectomy in one visit). From the results obtained, we can hypothetically conclude that a temporary molar with a carious cavity of less than 80% of the volume of the entire tooth, with an RDT of more than 1 mm, the absence of periapical changes, pain, dense hard tissues and healthy gums can be effectively treated only by the method of gradual excavation.
Conclusion
Temporary second molars with carious lesions of more than 2/3, with symptoms of pain, histologically show inflammation of the coronal and root pulp in all cases. Considering the clinical and radiological parameters, single-visit pulpectomy is considered the optimal treatment option in this situation.
Authors: Vellore Kannan Gopinath , General and Specialist Dental Practice, College of Dentistry Khurshid Anwar , Basic Medical Sciences, College of Medicine, University of Sharjah, Sharjah, United Arab Emirates
Surgical methods for treating dental pulp
In cases where therapeutic methods are powerless, the only option left is to remove the dental pulp. This option is used in cases where the patient’s immunity is weakened, the disease is at an acute stage, or the tooth will be used in the future as a support for prosthetics. Surgery involves amputation or extirpation of the dental pulp.
- Amputation of the dental pulp
- during the procedure, only the coronal part is removed. Prescribed for acute pulpitis or mechanical damage to the dental pulp. - Extirpation
is the complete removal of the pulp. Used for all forms of pulpitis.
The pulp can be removed vitally, that is, under anesthesia without prior killing. If this method is not possible, the doctor resorts to devitalization of the dental pulp - the toxic substance is left in the cavity for about a day, after which the dead tissue is painlessly removed. Means for devitalizing dental pulp include arsenic or paraformaldehyde paste.
Devitalization
There is no point in reminding how important it is to monitor the health of your teeth, but if, nevertheless, pulpitis begins, it must be treated urgently so as not to cause further complications. Unfortunately, the only treatment is complete removal of the pulp.
In other words, this process is called pulp devitalization . The procedure is carried out either mechanically using a special tool that drills a hole in the pulp tissue, or chemically using drugs that dissolve the damaged area.
The most commonly used pulp devitalization paste contains arsenic. It is applied to single-rooted teeth for a day, and to multi-rooted teeth for two days. Another drug for pulp devitalization is paraform paste; it is used in more severe cases and is applied for a period of five days to two weeks. An anesthetic tampon and a water dentin bandage are placed on top of the paste.
At the next visit, the doctor will carry out amputation, pulp extirpation, as well as instrumental and antiseptic treatment of the tooth canals. In place of the removed soft tissue, a filling with mummifying properties is installed, and on top of it is a regular, light-curing one.