Treatment of the upper chewing teeth is associated with the risk of damage to the maxillary sinuses due to their close anatomical proximity. When treating root canals, filling material may end up in the sinus cavity, which entails the development of serious purulent processes. Our Center has been specializing for many years in providing assistance to patients who have become victims of unsuccessful therapy. Such situations are corrected by experienced maxillofacial surgeons with ENT training using modern gentle surgical techniques
Causes and consequences of filling material in the maxillary sinus
In the maxillary region there are the maxillary sinuses, which occupy most of the internal space. Sometimes they are separated from the upper chewing teeth only by a thin bone septum (bottom of the sinus). During endodontic treatment, especially if the roots of the tooth have grown into the sinus cavity, the dentist may not calculate the effort, damage the apex of the root and the bottom of the sinus, as a result, the filling material falls into the sinus, “taking” purulent masses with it.
It is good if the problem is identified immediately and the patient is referred to a maxillofacial surgeon for immediate removal of the material. Otherwise, inflammation occurs in the sinus and the person comes for help himself, but with consequences.
Long-term presence of filling material in the maxillary sinus is dangerous due to the development of complications:
- chronic odontogenic sinusitis and sinusitis;
- mycetoma (fungal infection of the nasal sinuses);
- inflammatory processes on the roots of adjacent teeth;
- encephalitis and meningitis;
- osteomyelitis of the jaw.
Consequences and prevention of injury
This complication, if left untreated, can lead to:
- inflammation of the maxillary sinus;
- infection of surrounding bone tissues with transition to other sinuses of the skull;
- formation of foci of osteomyelitis in the upper jaw;
- suppuration of foci of infection;
- loss of healthy teeth in the affected area.
If the perforation was not identified and treated in time, this can lead to the development of sinusitis or acute sinusitis, which is characterized by acute pain, swelling of the nasal mucosa - with difficulty breathing and purulent discharge.
To avoid such unpleasant consequences of dental treatment for the patient, specialists at the Implantmaster clinic conduct a comprehensive study of the patient’s anatomical features using X-ray and computed tomography images and strictly observe the accuracy of medical manipulations.
Symptoms of complications
A person feels the presence of a foreign body in the sinus 2-3 days after treatment due to the characteristic symptoms of sinusitis. In some cases, it may not manifest itself for months or even years with a strong immune system, but makes itself felt when the body’s defenses are weakened. Also, the rate of development of the pathological process depends on the composition of the filling material that ends up in the sinus, the presence of components in it that can provoke inflammation, and the growth of fungal flora.
Characteristic symptoms:
- chronic nasal congestion;
- aching headaches;
- pain in the upper jaw, worsening with chewing;
- pain when lightly tapping the facial bone under the eye closer to the nose;
- thick purulent nasal discharge with an unpleasant odor;
- increase in body temperature in advanced conditions.
The difference between sinus inflammation due to the presence of filling material in it and sinusitis-sinusitis that accompanies influenza and colds is a one-sided manifestation of symptoms. Signs of odontogenic sinusitis are usually only on the side on which the tooth was treated.
results
All 124 patients with foreign bodies in the maxillary sinus underwent endoscopic endonasal maxillary sinusotomy to remove the pathological substrate from the sinus cavity. In 100% of cases, surgical treatment was successful and was carried out in one stage. In no case was it necessary to resort to repeated intervention. Foreign bodies in some cases may not be detected or may be removed in fragments. In our series of observations, complete removal was confirmed by the results of a control CT scan of the paranasal sinuses in the postoperative period. None of the 113 patients who received topical antibacterial therapy with Polydex sprays with phenylephrine and Isofra developed an acute inflammatory process in the nasal cavity and paranasal sinuses. Complete relief of reactive phenomena was recorded on days 3–7 of the postoperative period.
Clinical example
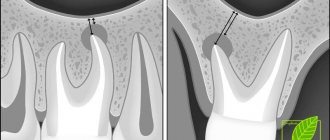
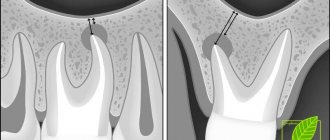
Patient K. applied to the otorhinolaryngology clinic of our university on the referral of a dentist; he had no active complaints. During endodontic treatment of the 16th tooth, the dentist diagnosed the removal of the filling material beyond the apex of the palatal root and the entry of the sealer into the cavity of the maxillary sinus. The patient was recommended to see an otolaryngologist. According to the results of the CBCT, the foreign body was located in the area of the natural anastomosis, slightly anterior to the uncinate process (Fig. 1, 2) . The mucous membrane of the upper jaw without signs of hypertrophy or edema indicates good function of the ciliated epithelium.
Rice. 1. Coronal section of computed tomography. There is a foreign body in the area of the natural anastomosis of the right maxillary sinus.
Rice. 2. Sagittal section of computed tomography. There is a foreign body in the area of the natural anastomosis of the right maxillary sinus.
The patient underwent surgical treatment under the control of navigation equipment under local anesthesia. Under topical anesthesia Sol. Lidocaini 10% + adrenaline 0.01% and infiltration anesthesia Sol. Ultracaini 1.7 ml using a 0° endoscope under the control of an electromagnetic navigation station, the location of access to the maxillary sinus was determined in the middle nasal passage, anterior to the area of the natural anastomosis, directly in the projection of the foreign body. The maxillary sinus is opened, the foreign body is removed (Fig. 3) with antral forceps in one movement. The sinus cavity was visualized with 30 and 70° endoscopes. Irrigation of the sinus cavity with saline solution. Stable hemostasis has been achieved. No postoperative tamponade was required. The surgical intervention time was <10 minutes.
Rice. 3. The foreign body is removed from the maxillary sinus.
In the postoperative period, the patient was prescribed irrigation of the nasal cavity with saline solutions, local antibacterial therapy with Isofra, 1 dose in each nostril 4 times a day for 5 days. The patient was transferred to outpatient treatment on the 1st postoperative day. In the postoperative period, the patient did not complain of difficulty in nasal breathing, discharge from the nose, or pain. Scanty reactive changes in the mucous membrane were completely stopped by the 3rd day of the postoperative period. The development of acute rhinitis/sinusitis was also not noted.
On control CBCT 1 month after surgery, the cavity of the right maxillary sinus is airy, without signs of foreign bodies, the mucous membrane is not thickened. The root canals of the 16th tooth are obturated evenly, up to the apex.
How to warn
Most often, underexamined patients encounter perforation of the maxillary sinus during dental treatment, when the doctor, without a clear understanding of the location of the roots, carries out treatment according to the standard protocol.
Rest assured that in our Center you will not encounter such risks.
The following allows us to prevent the penetration of filling material into the maxillary sinus: CT diagnostics before the start of tooth treatment.
Based on high-precision data, the doctor’s actions are planned and a safe endodontic protocol is selected.
Unfortunately, x-rays, which most clinics resort to due to the lack of expensive equipment, do not provide a complete picture. In our Center, the examination is carried out using a modern CT scanner Sirona Gallileos (Germany) with advanced settings in ENT mode. Such 3D images allow you to study in detail the location of the maxillary sinuses and dental roots, calculate the thickness of the bone septum, and determine the presence of dental cysts. Qualified endodontists
Treatment of teeth bordering the maxillary sinuses should be extremely careful, careful and meticulous. A doctor without experience, sufficient theoretical knowledge and practical skills to work in emergency situations is likely to make mistakes. In our Center, endodontic dental treatment is carried out by specialists with at least 10 years of experience; we do not hire students “off the street” or students immediately after graduation. Minimally invasive techniques for canal treatment under a microscope and 3D filling eliminate the risk of damage to the root canals and sinuses.
CT monitoring after treatment is also required . Before sending the patient home, the doctor must make sure that there is no perforation of the maxillary sinus, no dental material has entered it, and also evaluate the quality of canal filling. If pathological aspects are detected, the patient will have the opportunity to receive immediate help and avoid complications.
In case of unforeseen situations, when the bottom of the maxillary sinus is damaged and filling material gets into it, the patient should be immediately referred to a maxillofacial surgeon to remove the foreign body. Failure to provide timely assistance is fraught with the development of an acute inflammatory process with all the ensuing consequences .
Importance of complication
The maxillary cavities are located above the upper jaw, they are designed to warm the air entering through the nose and clean it from dust and debris. When treating teeth and insufficient thickness of bone tissue, filling material often penetrates into these cavities through damaged tissue.
The possibility of removing a foreign object over time is completely excluded, and patients are also unable to carry out therapy on their own. The therapy involves self-penetration into the sinuses and removal of the filling material stuck there.
This is technically impossible for the patient to do on his own; often the pieces are sharpened at the border of the gum and tooth, and only a professional doctor can handle them.
Therefore, it is important to detect it in time, make a reliable diagnosis and provide quality treatment. Such an operation is not particularly difficult for a doctor. Depending on the specific medical institution, the patient may be discharged either on the same day or the next. The operation is performed using local anesthesia.
Why is it better to contact the ENT department of dentistry?
If you still find yourself in a difficult situation after unsuccessful dental treatment, you can only eliminate the consequences with a guarantee from an oral and maxillofacial surgeon with ENT training.
Otolaryngologists and ordinary dentists have a fundamentally different approach to the issue of diagnosis and treatment of diseases of the paranasal sinuses of odontogenic (“dental” origin). Each of them solves the problem only in its own part, while it requires an integrated approach.
The complexity of interaction between these two specialists in city clinics, the reluctance of each to delve into the problems of related specialties, and the lack of joint consultations lead to errors in diagnosis and choice of treatment tactics. As a result, the patient goes in a vicious circle from one doctor to another to no avail.
ENT dentistry has a number of undeniable advantages in this regard.:
- an integrated approach to solving the problem;
- accurate diagnosis using CT in ENT mode;
- treatment is carried out by a specialist equally knowledgeable in dentistry and otolaryngology;
- Carrying out gentle dental operations without mandatory hospitalization.
In our Center, operations to eliminate combined dental and ENT pathologies are performed by experienced surgeons with ENT training, candidates of medical sciences.
KolchinSergey Alexandrovich
Maxillofacial surgeon, 7 years of experience
Surgeon with ENT training. He specializes in ENT dentistry, including performing endoscopic operations and carefully removing tumors in the sinuses.
More about the doctor
Diagnosis of complications in the maxillary sinus
Diagnostic measures are aimed at determining the size and localization of dental material, the degree and prevalence of inflammation of the mucous and bone tissues of the sinus.
- Visual inspection Performed using a nasal speculum, it allows you to determine the presence of a foreign body in the nasal sinus.
- Computed tomography in a special ENT mode is the most accurate type of diagnosis of combined dental and ENT pathologies today. The advanced settings of our tomograph allow us to evaluate the maxillary sinuses in full. This allows the maxillofacial surgeon not only to determine the presence/absence of a foreign body, but also to assess the condition of the mucous membrane, determine the amount of purulent masses, and the extent of inflammation.
A 3D tomogram gives a complete picture of the condition of the maxillary sinuses, the location of the filling material, and the degree of inflammation
Material and methods
At the Otorhinolaryngology Clinic of the First Medical University named after. acad. I.P. Pavlova surgical treatment of 124 patients with foreign bodies of the maxillary sinuses was performed in 2022. This pathology was found almost equally among both males (56 patients) and females (68). 77 patients were referred for consultation to an otorhinolaryngologist by a dentist. In 15 patients, the foreign body turned out to be an incidental finding during an X-ray examination of the skull for other pathological conditions. All patients underwent endoscopic endonasal maxillary sinusotomy under the control of rigid endoscopes with different visualization angles (0, 30 and 70°). Typically, this operation is performed under local anesthesia with preliminary premedication. In 7 patients, surgical treatment required general anesthesia. This was associated with pronounced psycho-emotional arousal and increased anxiety in patients. In 27 cases, the removal of the pathological substrate required the use of navigation equipment, since in these cases the foreign body was localized submucosally and/or in parts of the maxillary sinus that were difficult to visualize. Since 2013, patients with complex localization of foreign bodies in the upper jaw have undergone surgical treatment under the control of a navigation station. In 106 people, transnasal maxillary sinusotomy was performed through the lower nasal passage. Of these, in 95 cases the temporary anastomosis was plastically reconstructed. In 11 patients, a persistent antrostomy was formed, as there was a pronounced inflammatory reaction of the mucous membrane of the maxillary sinus. The same group of patients was prescribed systemic antibacterial therapy in the postoperative period. The presence of an adequate anastomosis in the lower nasal passage made it possible to perform lavage of the maxillary sinus in the postoperative period by analogy with the puncture method of treatment. Many years of experience at our clinic shows that odontogenic foreign bodies in a large percentage of cases can be removed by access through the lower nasal passage, without the formation of a persistent anastomosis, so as not to disrupt the complex anatomical structure of a healthy natural anastomosis [9]. Also, due to the minimally invasive nature of this treatment method, patients do not require systemic antibiotic therapy. We prescribed topical antibiotic therapy to 113 patients in the postoperative period. 72 patients were prescribed topical Polydex spray with phenylephrine, 41 were prescribed monocomponent antibacterial spray Isofra. The choice of the prescribed drug was associated with the presence or absence of swelling of the mucous membrane and complaints of nasal congestion.
Stages of removing material from the sinuses
Treatment at the Center is comprehensive; we try to combine all procedures in one visit
- Preparation It is important to create sterile conditions to prevent infection of the surgical wound during the intervention. Hygienic cleaning of the oral cavity and treatment of compromised teeth are carried out.
- The operation is performed according to the selected protocol in the operating room of the ENT department. The patient is in a state of drug-induced sleep. After the operation, a CT scan is repeated to assess the quality of the work performed.
- Prosthetics If it is not possible to preserve the causative tooth, digital impressions are immediately taken and a temporary immediate prosthesis is made to hide the aesthetic defect until permanent prosthetics are installed.
To put you to sleep, we use safe ultra-thin sedatives - Propofol or Diprivan. We do not use general anesthesia, since it has a severe effect on the body and is associated with certain risks. Our full-time anesthesiologist monitors the patient’s well-being during the operation. Upon completion of treatment, a person wakes up rested, full of strength and energy, and within half an hour after drinking tea he can return home.
How we treat
Treatment is carried out only comprehensively and strives to be carried out in one visit , simultaneously:
- Hygienic cleaning and dental treatment We prepare the oral cavity for sterile surgical work. We treat compromised roots. Operations are performed only in a sanitized oral cavity to avoid re-infection.
- The operation is carried out in the surgical department, subject to all conditions of sterile operating rooms. Ultrasound removes inflammatory processes, removes roots that provoked or supported inflammation, eliminates all inflammatory elements, removes cysts, polyps, mucoceles, and foreign bodies.
- Orthopedics Temporary crowns or any other orthopedic elements are fixed to mask the work performed. We do everything to avoid sending the patient home without teeth!
We do not welcome radical and punitive surgery!
Rest assured that after surgery we will never keep you in the hospital unless absolutely necessary.
Levin Dmitry Valerievich Chief physician and founder of the Doctor Levin center
Recovery period
Recovery after surgery is the most unpleasant moment for patients. We made sure that this period was as short and painless as possible
No hospitalization
The use of gentle surgical techniques using an ultrasound protocol and microscopic equipment allows us to carry out treatment with the utmost delicacy and minimal trauma. Coming out of sedation is not accompanied by the consequences of general anesthesia; you will not be haunted by nausea, dizziness and clouding of consciousness. Therefore, hospitalization and hospital stay for 3-4 days will not be required ; 30 minutes after the operation you will go home.
For patients with cardiovascular pathologies who require postoperative observation, the Center operates a day hospital department.
A set of procedures for accelerated rehabilitation
For quick recovery after surgery, our Center offers its own method of accelerated rehabilitation. The procedures are aimed at preventing swelling, hematomas, and eliminating pain. The program includes:
Home care
You will receive at home all the medications you need for recovery and instructions for taking them free of charge. In this way, we prevented the purchase of counterfeit products, and you will not need to run to pharmacies on your own after the operation.
The medication kit, selected by a doctor, includes all the necessary medications to improve your well-being and prevent complications.
Please do not violate the frequency of use and follow the recommendations from the leaflet that you will receive along with the medications.
If you have any questions, please contact the phone number listed in the brochure. The postoperative patient support service operates around the clock 24/7.