Where does red throat come from?
A red throat is hyperemia of the pharyngeal mucosa - a symptom that accompanies various diseases of the pharynx in adults and children. Hyperemia can only be in the area of the arches, tonsils or posterior wall of the pharynx; all areas can also be involved at once, including the soft palate. The process can also be one-sided or two-sided.
But it is worth noting that the assessment of this symptom is sometimes not objective, since it is influenced by the color perception of both the patient and the doctor, and external lighting. Therefore, the patient should consult a doctor in order to carefully collect the entire history of the disease and identify the cause of the red throat.
Types of palpation of the larynx and neck
Superficial palpation
This type of study is focused on obtaining objective data on the consistency and turgor of the skin in the neck area, which can be changed as a result of the development of a pathological process, for example, a malignant tumor. The patient is in an upright position.
The area is palpated in two positions - with the head in the normal position and slightly tilted back. The results make it possible to assess the nature of the relief of the skin covering the larynx and neighboring areas.
- hyoid bone;
- thyroid cartilage;
- cricoid cartilage;
- breastbone;
- prominence of the hyoid bone;
- the depression between the hyoid bone and the thyroid cartilage;
- Adam's apple;
- the cavity between the cricoid and thyroid cartilages;
- arch of cricoid cartilage;
- laryngeal prominence;
- depression above the breastbone.
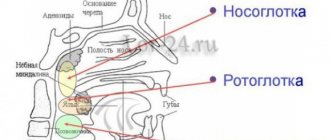
Anatomy of the pharynx
The pharynx is located behind the nasal and oral cavities; begins at the base of the skull and reaches the lower edge of the 6th cervical vertebra, where it narrows in a funnel-shaped manner and passes into the esophagus.
There are three sections of the pharynx:
- upper – nasopharynx
- middle – oropharynx
- lower – laryngopharynx
Nasopharynx
In the nasopharynx there is an accumulation of lymphoid tissue, which forms the pharyngeal tonsil - adenoids. Also in the nasopharynx are the tubal tonsils, which are located around the pharyngeal openings of the auditory tube.
This part of the pharynx is visualized only with the help of instruments or video endoscopic examination.
Oropharynx
The oropharynx is precisely that part of the pharynx that attracts attention when examined by an otolaryngologist and is accessible for examination by the patient himself.
It is located behind the oral cavity and is delimited by the pharynx. The pharynx is an opening formed above by the soft palate and uvula, on the sides by the anterior and posterior arches, and below by the root of the tongue. Between the anterior and posterior palatine arches there are another lymphoid accumulations - the palatine tonsils.
The palatine tonsils, arches, and uvula are subject to friction at the time of swallowing, due to which their mucous membrane may appear redder (hyperemic), in contrast to the entire oral cavity, gums, etc. But this is just a physiological factor.
The mucous membrane of the posterior pharyngeal wall contains elements of lymphoid tissue that visually resemble granules. The mucous membrane of the oropharynx has a dense network of vascular and lymphatic capillaries with rich sensory innervation, and therefore pathological processes are accompanied by symptoms - pain and discomfort in the throat, sensations of dryness, etc.1
hypopharynx
The laryngopharynx begins at the level of the upper edge of the epiglottis and passes into the initial part of the esophagus.
This part is also visualized only using instrumental and video endoscopic methods. This area is visually inaccessible to the patient.
Diseases of the oral mucosa are accompanied by various pathomorphological changes. Inflammation is one of the most common pathological processes of the mucous membrane of the mouth and pharynx and is a manifestation of the body’s protective reaction to the influence of a pathogenic factor. The course and outcome of the inflammatory process depends on the reactivity of the body, localization, activity and duration of action of the pathogenic factor.2
Pharynx cancer/larynx cancer - characterized by the occurrence of a malignant formation that consists of epithelial cells. It is more common in men aged 40-60 years and accounts for up to 3% of all human oncology.
The throat (medically: pharynx) is divided into three parts:
- Upper part: The upper part, the so-called nasopharynx or epipharynx, begins behind the nasal cavity and ends above the soft palate.
- Middle part: The mesopharynx or oropharynx, that is, the part associated with the mouth, includes not only the posterior wall of the pharynx, but also the base of the tongue, pharyngeal tonsils and the anterior surface of the soft palate. It ends at the transition to the larynx.
- Inferior: The lowest part of the pharynx, the hypopharynx, begins where the air and food tracts separate and lies behind and away from the entrance to the larynx.
In more than 90% of cases, pharyngeal carcinoma is squamous cell carcinoma arising from mucosal cells. Cancer of the hypo- or oropharynx usually affects men over 60 years of age. The most common are malignant diseases in the oropharynx. Other malignant tumors, such as malignant melanomas, lymphomas, tumors of the minor salivary glands, or extramedullary plasmacytomas, are much less common.
Certain tumor diseases in the nasopharynx differ from those in the lower two parts of the pharynx. They are common (endemic) in southern China, northern Africa and Alaska and are often associated with Epstein-Barr virus (EBV) infection. For other, nonendemic forms of nasopharyngeal carcinoma, other risk factors may be present and significant, the same as for tumors in the lower regions of the pharynx.
ENT examination and speculum examination
An examination by an ear, nose and throat specialist (otolaryngologist) includes a thorough examination of:
- oral cavity,
- nose and throat,
- larynx and ears.
Using a small mirror that the doctor holds in the mouth area, he can also see parts of the nasopharynx and larynx. This is why we talk about examining with a mirror. Many tumors in the pharynx can already be identified thanks to this examination alone.
Hearing testing and measurement of tympanic membrane mobility may indicate tubal dysfunction in nasopharyngeal carcinoma.
Endoscopy
If a patient has trouble opening their mouth—which most often happens with advanced tumors in the ear, nose, or throat—the doctor may use an endoscope.
An endoscope is a medical device that allows you to see the internal cavities of the body from the inside. For this purpose, the light source is connected to either a flexible hose or a rigid tube. Optics allows for examination with ocular magnification of a magnifying glass. Through special channels, instruments can be introduced, thanks to which, for example, samples can be taken.
The doctor also often uses an endoscope to accurately examine the nasopharynx. The so-called panendoscopy, that is, an endoscopic examination of the entire upper respiratory tract and digestive tract (mouth, throat, larynx, esophagus, bronchi) under general anesthesia, serves, on the one hand, to determine the extent of the tumor, and on the other, to identify a possible second carcinoma . During panendoscopy, tissue samples are taken from suspicious areas. Through histological examination of these tissue samples, the diagnosis is ultimately assured.
Blood analysis
If the patient has been infected with Epstein-Barr virus, antibodies to this virus may be detected in the blood (EBV serology). The presence of EBV antibodies reinforces the suspicion of nasopharyngeal cancer. This is especially true for patients from endemic areas (Asia, North Africa or Alaska).
Tumor staging
To stage a tumor—the so-called search for signs of cancer spread—further examinations are carried out in addition to the panendoscopy described above. To detect signs of tumors (metastases), an ultrasound examination of the soft tissues of the neck and abdominal cavity (especially the liver) and an x-ray of the lungs are performed. Other imaging modalities in the search for metastases include computed tomography, magnetic resonance imaging, and, especially for large tumors, bone scintigraphy.
How is oropharyngeal and hypopharyngeal carcinoma treated?
If possible, these tumors should be removed surgically. Radiation therapy is often performed along with surgery. Depending on the location and extent of the tumor, access to surgery may be through the mouth, under the chin (behind the lower jawbone), through the lower jaw, or through the neck.
At the same time, tumor removal using transoral laser surgery is possible in many cases. With this method, the operation is performed through an open mouth, using an endoscope and under microscopic magnification. The cutting tool is a CO2 laser. With this method, very targeted removal of even large tumors is possible. Adjacent structures and therefore throat functions (eg swallowing) are usually better preserved than with conventional surgical techniques.
First of all, small tumors (T1 and T2) are usually easily removed. In the case of large tumors, it may be necessary to plastically cover larger missing parts of tissue with a perfused so-called tissue flap.
Primarily at the time of diagnosis, pituitary tumors often spread to adjacent structures such as the larynx, esophagus, or thyroid gland, which then need to be removed during surgery. In many cases, however, these tumors can no longer be completely removed by surgery.
In most cases, the lymph nodes in the neck are also removed. In this case, they speak of a “neck cut.” This is also recommended if enlarged lymph nodes are not detected, because the rate of spread of metastases in lymph nodes that are not yet visible when swollen is relatively high. Depending on the type and extent of the tumor, lymph nodes should be removed only on the side on which the tumor is located or on the opposite side.
Doctors often treat advanced carcinomas with a combination of chemotherapy and radiation therapy. The targeted drug cetuximab also plays an important role. This is an antibody against a specific protein that is often found in tumor cells. This drug is also used to treat other types of cancer. The prognosis of the disease depends on the type and extent of the tumor. Studies in recent years have shown that patients with oropharyngeal carcinoma caused by HPV have a significantly better prognosis. One reason is that these carcinomas respond better to radiation and chemotherapy. Also, small tumors (T1, T2) of the oropharynx have a good prognosis.
How is nasopharyngeal carcinoma treated?
- Radiation therapy: Nasopharyngeal carcinoma is usually irradiated because the affected area is not easily accessible to surgery. In most cases, the lymph nodes in the neck also receive radiation therapy because nasopharyngeal carcinoma has often already spread to them.
- Surgical removal (“neck dissection”) is recommended for recurrent or residual tumors remaining after radiation therapy.
- Patients often receive concomitant chemotherapy (chemoradiotherapy) for advanced tumors. In advanced tumors, there is evidence that both prior (neoadjuvant) and subsequent (adjuvant) chemotherapy in addition to radiation chemotherapy may reduce the risk of relapse. However, it also increases the side effects of such treatment. Therefore, the decision in individual cases must be made individually.
- For tumors with distant metastases, palliative chemotherapy may be appropriate in combination with radiation therapy.
The chances of effective treatment are much better the earlier the cancer was detected.
The Clinic of Otorhinolaryngology, Head and Neck Surgery at the City Clinical Hospital of Solingen, Germany, specializes in complex cases of pharyngeal cancer.
How to contact us
Consultation, diagnosis, treatment or a second opinion on your diagnosis can be obtained by contacting our specialists from the international department, write to us or leave a request for a call back. Email: [email protected] Tel.: +49 212 5476913 Viber | WatsApp: +49 173-2034066 | +49 177-5404270 For your convenience, please enter the phone number in your phone book and call or write to us for free on WhatsApp, Viber or Telegram. Applications made on weekends or holidays will be processed on the first business day. In urgent cases, request processing is carried out on weekends and holidays.
Causes of a red throat
| CAUSES | A COMMENT | ||
| causes: | Infectious causes | a comment: |
|
| causes: | Non-infectious causes | a comment: |
|
In 70% of cases, inflammation of the pharyngeal mucosa is caused by ARVI viruses (rhinoviruses, adenoviruses, coronaviruses, influenza and parainfluenza viruses), as well as other viruses (enterovirus, herpes virus, Epstein-Barr virus for infectious mononucleosis, and others).
The cause of inflammation can be bacteria:
- group A beta-hemolytic streptococcus (GABHS)
- Staphylococcus aureus
- Streptococcus pneumoniae
- Haemophilus influenza
It should be remembered that a red throat can be a manifestation of infectious diseases such as measles, scarlet fever, and rubella. In some cases, differential diagnosis with other infectious diseases is required.
Benefits of treatment at GMS Hospital
Removal of benign tumors of the pharynx and larynx at the surgery center of the GMS clinic is carried out on an outpatient basis, using endoscopic technologies. Endoscopically-assisted operations have the following advantages:
- minimal surgical trauma - healthy tissues are not injured;
- targeted accuracy - all modified tissues are removed along with the growth zone;
- minimal blood loss - simultaneous coagulation of blood vessels ensures the absence of bleeding both during and after the intervention;
- short recovery - the patient returns to normal life after 4-7 days;
- the ability to remove all tumors in one operation;
- high clinical result.
Since the operations are performed through the oropharyngeal approach, pain is minimal or completely absent. You can make an appointment with an otorhinolaryngologist at GMS Hospital by leaving a request on the website or by phone.
Diagnosis of red throat
To identify the cause of a red throat, the patient must consult an otorhinolaryngologist (ENT) or therapist.
If a child has a red throat, a pediatrician’s consultation is necessary.
To identify lesions of the oropharynx, certain rules must be followed. First of all, the inspection requires sufficient lighting (fluorescent lamp, frontal reflector, etc.). The doctor carefully collects anamnesis to make the correct diagnosis.
An otorhinolaryngologist may prescribe a consultation with other specialists: a gastroenterologist, a dentist, and others.
Various laboratory tests are performed: bacteriological examination (culture from the back of the throat and tonsils and PCR), blood tests (complete blood count, ESR, C-reactive protein).
Indications
Indications for palpation of the larynx and neck:
- injuries (fractures, bruises) and stenosis of the larynx;
- malignant tumors;
- laryngeal tonsillitis (enlarged regional lymph nodes can be felt);
- laryngitis, including phlegmonous (severe pain is observed when pressing on the affected area);
- foreign bodies of the pharynx and esophagus;
- retropharyngeal abscess;
- pathologies of the thyroid gland (hypothyroidism, etc.).
At the same time, palpation as an independent and only diagnostic method is used relatively rarely; it is supplemented by laryngoscopy, pharyngoscopy and other studies.
Features of the rehabilitation period
Endoscopic removal of tumors of the pharynx and larynx is a minimally invasive operation with a short rehabilitation period. After the intervention, the patient is transferred to a day hospital ward, where he will remain under medical supervision for several hours. For two weeks, you need to limit physical activity and exclude thermal procedures (bath, hot bath, sauna).
You also need to adhere to a certain diet:
- exclude coarse, hard, spicy, sour and any other foods that irritate the mucous membrane;
- Avoid hot and cold drinks and food.
Most often, medications are not required after endoscopic surgery. But under some circumstances, an otolaryngologist may prescribe a course of antibiotic therapy, immunomodulatory and antiviral therapy. You can get more detailed information about the removal of benign tumors of the hypopharynx by making an appointment with an otolaryngologist, by phone or online.