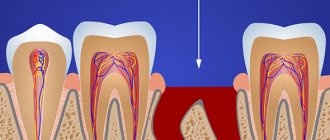
When using an insulating scarf like this on a claustrophobic patient, we can make a hole in an unimportant place: otherwise the patient will be afraid that we will suffocate him
Adults are afraid of us more than other doctors. In second place, perhaps, are surgeons, but they are not feared for long. About a third of patients suffer from dental phobia or dental phobia.
The best fear is rationalized. “Ahh, doctor, I’ll open my mouth now, and you’ll stick a huge long needle in there and do something” - great. “Will you infect me with hepatitis from your dirty tools?” - even better, everything is extremely rationalized. By the way, demanding a demonstration of sterilization is your completely normal right. “And if the drill breaks in my mouth, will the fragments fly out or in?” - in general, the best thing to work with, because the patient has a specific scenario. More precisely, even two!
Fear of a doctor is most often irrational. Somewhere, once upon a time, someone got into a patient’s mouth unsuccessfully in childhood, and now the doctors first became evil old women, and then a complex like “I’d rather die, but I won’t give in to them” simply formed. It is normal to feel fear, and you can work with fear. The question is how. For example, women may cry in the office from emotional stress - this is normal; up to a third of patients do this. But men act differently. They have a wonderful life hack: they don’t come.
In general, come in, I will teach you to be afraid of dentists. Let's talk about the causes of fear, methods of working with it, and a little about real risks. Well, thanks to the Soviet compulsory medical insurance approach, I now have boxing with anesthesia in every clinic.
What is dental phobia or dental phobia?
This is when you are afraid of dental treatment.
You may also be afraid not of the treatment itself, but of the dentist, of medical devices, and of opening your mouth in general in front of strangers who are trying to do you good. Or any other element of the dentist’s office - from smell to sound. Physiological manifestations are completely normal, as for any other fear. For example, if you don't have dental phobia, you can jump with a parachute and remember the sensations on the plane. A mentally healthy person should experience irrational fear of the same nature.
Dental phobia is characterized by the following reactions:
- Increased blood pressure. Very convenient when you need to run away from a doctor or fight with him.
- Increasing muscle tone also increases your chances in a fight with a doctor from an evolutionary point of view.
- Pupil dilation (a side effect of activation of the sympathetic nervous system, the original meaning of the reaction is almost lost).
- Discomfort in the gastrointestinal tract: because you urgently need to take resources for something else, and this system is rushed without control. By the way, if you also start to smell terrible, this will increase your chances in battle. And it will be easier to run, so the effect is also evolutionarily useful.
- Degradation to the level of trained quick decisions, often reflexive - without the participation of complex conscious processes.
Basically, it's the classic prolonged fight-or-flight response that turns into a long flight, flight, flight response.
The only thing is that evolutionary progress has not yet affected adaptation to dentists. There is another reaction - “freeze.” In this case, the patient sits motionless in a chair with a pale appearance. As a rule, in this situation, resources are pulled from the periphery to increase supply to the brain, so there are far fewer problems with the “freeze” reaction. The patient consciously understands that everything is going as it should, he just feels uncomfortable. In this case, it is especially helpful to give the patient back control over what is happening through a very detailed explanation of what is happening and the ability to generally control the intervention. I'll tell you more about this below.
And there is also dental phobia - an even more interesting type of reaction, when fear is caused not by the intervention itself here and now, but by the thought that one will have to undergo it. As a result, the patient systematically avoids dental appointments because he is afraid of treatment. Over time, the need for this treatment begins to grow, but the patient understands that its volume will also increase - and is proportionally more afraid. As a result, this leads to the situation described above, when a masculine man endures to incredible limits, sometimes surprising even experienced surgeons. And in dentistry, you know, it’s quite difficult to bring your condition to a dangerous level. To do this, you need to make real efforts and endure pain for quite a long time, which will bring even the strongest among us to their knees. But the men cope, and then I have to assemble a new jaw for them - or call a surgeon to pump out pus from the cellular spaces of the skull.
What is child phobia - just fear or a disease?
Everyone gets nervous before visiting a dental office.
Some people simply experience slight nervousness and discomfort, while others are terrified of even the thought of visiting a dentist, and the mention of a drill makes such a person hysterical. It is in the latter case that dental phobia occurs (synonyms for this concept are also the terms odontophobia and dental phobia) or panic fear of visiting the dentist.
This serious pathology should be distinguished from the usual fear of dentists, which almost any person experiences in the dentist's chair. It manifests itself in attacks of uncontrollable fear, hysteria up to loss of consciousness. People suffering from hypertension may experience hypertensive crises or angina attacks. Such patients are usually not contactable, and even the most experienced doctor is unable to find a common language with them.
Most often, people with dental phobia go to the dentist only in advanced cases. For example, when a tooth hurts so much that painkillers do not help, or a decayed tooth prevents you from speaking normally and eating fully.
The Good News: Fear is Normal
Being afraid of something is a normal physiological state.
It is not considered a psychiatric diagnosis as long as you can overcome your fear. If you can’t, then questions already arise (but this is not a diagnosis yet). It is believed this way: if you received treatment, although you were terribly afraid of it, everything is in order, you deserve to be called Sapiens. If not, then you need to do something about it next. For example, pathological fear of the dentist is not a fictitious dental phobia, but a so-called congenital one, which cannot be controlled at all, or, for example, acquired in early childhood, can be corrected by prescribing daytime tranquilizers (benzodiazepine series). They won’t completely remove the fear, but they will at least allow you to get to the clinic and get treatment. True dental phobia is a pathological story and requires treatment. A person cannot cope with it without outside medication or preventive behavioral therapy.
Often patients are afraid of pain, not the doctor. In this case, there is no need to try to overcome fear. This is even more normal, rarely does anyone like pain, although this does happen. The fact is that we can offer different means - from the Viking combat cocktail (nitrogen) and local anesthesia to medicated sleep and anesthesia.
Types of dentophobia
The disease is divided into the following types:
- Imaginary dental phobia.
- Acquired dental phobia.
People with the first type of disease have been terribly afraid of any medical procedures since childhood. The injections cause them to faint. Even such a not very painful procedure as drawing blood from a finger brings them into terrible horror. If such a person is to undergo more serious treatment, then he must be prepared for this in advance.
The second type of disease appears against the background of external causes. Often people begin to fear the dentist after terrible stories from friends. They understand that their mouth needs long and serious treatment. But the negative information they hear makes them afraid of the sound of a drill and a doctor in a white coat. Dentophobes often leave the dental clinic just before entering the office.
An acquired phobia always manifests itself as a result of personal experience. The patient remembers the pain, the unpleasant manipulations of the dentist, the sound of the drill, and anesthesia. He further recalls that the filling he placed fell out very quickly and he again had to go to the dentist’s office. Bottom line: fear is constantly reinforced by new factors and emotions.
The Bad News: Fear Is Mostly Irrational
This means that it can only be “overpowered” or bypassed, but not removed by any rational reasoning or action.
More precisely, there are several components of fear, for example, fear of the unknown, misunderstanding of the duration of the intervention, constant anticipation of pain, and so on - they can be reduced. And there are irrational factors with which nothing can be done. And fear of the dentist is usually a complex of these things. The most common irrational fears arise:
- Due to childhood psychological trauma, for example, successful treatment (suspension) of caries using a Soviet drill of the “bzzzzhrrrrr” model with the smell of burnt tissue (overheated dentin).
- The guilt is that you will be reproached for being in such a state. That is, the patient first brings himself to a serious state by being afraid of the doctor, and then begins to fear that the doctor will scold him for bringing himself to this point. Great combination.
- Constraints. For example, that previously there was no money for a dentist, and this will have to be explained somehow (in reality, of course, not).
- And just some kind of life attitudes, superimposed on the whole complex of the fact that you will have to get to the doctor, tell him something, open your mouth in front of a stranger and allow foreign objects into it, feel pain (if you are unlucky) and feel psychologically and physically helpless throughout the entire procedure.
Oddly enough, dental phobia can be congenital, that is, genetically determined. It's not entirely clear how this works, but here's a quote from a 2016 study:
It is clear that, in addition to environmental factors, genetic influences are important in the etiology of dental fear and anxiety, and should be considered in future studies of fear and anxiety associated with dental treatment and, potentially, interventions aimed at reducing distress that is a barrier to dental treatment utilization. Toward a Genetic Understanding of Dental Fear: Evidence of Heritability (doi: 10.1111/cdoe.12261)
Causes of dental phobia
The exact cause of dental phobia has not been determined to this day. However, there is a clear belief that fear arises against the background of ongoing changes in the central nervous system. And:
- Dentophobia appears against the background of dental trauma in childhood. Fear that was experienced in the past cannot let go of a person in the present.
- The disease seems to be inherited. Usually, if parents suffer from dental phobia, children in most cases inherit this fear from them. Emotional fear of the dentist becomes a family phobia.
- Dentophobia affects people who have always experienced attention deficit. They are usually withdrawn or, on the contrary, have increased hyperactivity.
- The disease causes stress experienced, which has acquired a chronic form or neurosis.
- Dentophobia becomes a consequence of the resurfacing of past painful manipulations in the memory.
- Stories from relatives, friends, and acquaintances about improper and unqualified treatment from dentists lead to illness.
- Fear arises against the background of a very high sensitivity threshold.
- A state of increased anxiety leads to fear of the dentist's action.
- Dentophobes suffer from frequent panic attacks.
- A person’s consciousness is influenced by the negative impact of social networks and the Internet in general, where terrible videos about dental treatment are often posted.
- A person is unable to tolerate the sight and smell of blood.
- Consequences of improper upbringing (in some families it is customary to scare children with the dentist).
- Dentophobes often suffer from a fear of any doctors, not just dentists.
- A person with bad teeth understands that he has already delayed treatment and will have to treat his entire mouth. Therefore, he is terribly afraid of this long and painful procedure.
- A dental phobe may experience a fear of contracting a foreign disease (HIV, hepatitis) through tools.
- He often experiences an absolute feeling of helplessness.
- A dentophobic person has no control over his emotional states.
- Any medical intervention causes fear.
- The presence of a disease such as vegetative-vascular dystonia.
- Fear of dental instruments, leading to gag reflex and choking anxiety.
What can you do to relieve fear?
In my experience, it is often easier for adults to overcome fear by increasing awareness.
A person is afraid not of the intervention itself, but of the unknown. The patient somehow scares himself, describes what is happening in his imagination, and relies on unreal things. True, there is also a point here: it may turn out that the real intervention is in fact more terrible than what the patient imagines. Therefore, in preventive conversations I do not show huge needles during a tour of the office, and in general, before such conversations, it is better to understand what exactly the patient is afraid of, so as not to frighten him even more with a demonstration of the arsenal of the Inquisition. From experience, no one is afraid of a spatula; I show it first.
In general, the psyche works like this: if some terrible thing happened to you and you are afraid, then the doctor can say:
- Well, patient, my tongue has turned green. Happens.
And then the doctor names some Latin word.
Hop - and you calm down, because in this short phrase there is information that you have something known, understandable, it has a term, and this happens not only to you, but to many in general. And if there is a term, it means that the phenomenon becomes not an unknown dangerous thing, but an understandable dangerous thing. It’s the same with fear: this is a unique event for the patient, but for the doctor he has hundreds of episodes a month. People are afraid that they are not like everyone else, and knowing that a doctor sees fear every day is also reassuring.
There is a lot of fear of losing control. The doctor gains power over you - and this is terrible. Therefore, you need to agree on the process and give the opportunity to manage it.
- When you say “ahh” or “stop” or blink twice, I will stop.
When I was a student, while studying pediatric dentistry at the department, children with moderate fear (without panic) were given a toy remote control on a wire before an intervention, and the wire stretched somewhere beyond their field of vision. The doctor turned on the drill and asked to press the red button on the remote control. The child pressed, the doctor saw that he was pressing and released the pedal. At this point, anxiety was greatly reduced. Then the duration of iterations was longer: drilled, washed, drilled again - these are far from modern devices. The main thing is to really stop when the patient asks, and not “now, just a second.”
Patients are also often afraid of the whistling sound of the turbine tip - this is the same dangerous bzzzz, turning into an inhuman whistle, which you may have heard in childhood. In our country, nozzles with such a rotation speed are rarely used; in the expensive segment, it is possible to afford other materials that allow us not to choose a turbine design. As a result, probably once every hundred patients I take out turbine tips (they are now used to saw massive structures).
Some are afraid of a rubber dam (cofferdam) - a latex scarf for isolating the oral cavity, which is generally needed for any more or less invasive interventions, including working with caries. If the patient is prone to claustrophobia, then he will be afraid of isolation - because the main fear there is the fear of suffocation, and the curtain of the oral cavity causes the same fear. You can make a hole in an unimportant place in the rubber dam - it will be easier for the patient.
Patients also like it when they are told in advance how long they need to endure. They are often afraid or embarrassed to ask questions. You tell a person that the worst thing lasts 15 seconds on this tooth and 25 seconds here, he understands the time distribution and does not panic ahead of time.
A very important point in fear is that a person has to face the inevitability of losing the illusion of immortality. We don't see atherosclerotic plaques, we don't see ulcers, we don't see how joints age and wear out. And here you cannot miss the evidence of mortality in dentistry, it is obvious and is in an area that is emotionally charged. And this is one of the hardest experiences in life. This fear is on a level with loss of reason and existential fear of loneliness and is one of the honorable three most terrible things for a person. But usually it is tested before going to the doctor. Often - instead of going to the doctor, alas.
How to overcome fear as an adult
People often don’t understand how to stop being afraid of the dentist. First of all, an adult needs to understand that, despite his own fear, it is necessary to treat his teeth and no matter how long a dentist puts off going to the dentist, he will still have to visit him. And the more timely this trip is, the easier and cheaper the treatment will be.
Below are recommendations on how not to be afraid of the dentist as adults.
If the fear is caused by the possible incompetence of the dentist or the fear that the doctor will ridicule and scold the patient for the condition of the teeth, then you should be more selective in choosing your doctor. Today, the dental services market is replete with all kinds of offers, promotions, and discounts. Therefore, you can choose a dentist who is suitable both in terms of experience and budget.
It is also recommended to try to establish interaction with the doctor yourself, asking him to stop the procedure if the procedure suddenly becomes painful. Understanding that the procedure will stop instantly at the slightest pain will give the patient confidence and peace of mind.
When choosing a dental clinic, it is better to give preference to one that is more reminiscent of a rest home than a hospital, depressing with its snow-white walls and evoking terrible thoughts.
If you have a deep fear of pain, it is recommended to insist on anesthesia before the procedure. The mere fact of administering an anesthetic will give confidence to the patient.
It is often possible to overcome fear through sedation - putting the patient into half-asleep (superficial sleep) with the help of dinitrogen oxide. You should find out in advance about the availability of such a service at the dental clinic.
In addition to the listed activities, people who are interested and say, I’m afraid of the dentist - what to do, the support of loved ones helps to cope with situational fear of dentists. It is much easier for a human individual to endure various unpleasant manipulations if a loved one is nearby.
Fear and cowardice
Fear has nothing to do with cowardice.
Fear is the body's response to circumstances. Cowardice is the result of decision making. A fearless person is not one who is not afraid, but one who knows how to work with his fear. Every mentally healthy person is afraid in principle. Physiologically, fear is the mobilization of the body for an optimal reaction.
The good news is that the ability to work with your fears can be trained.
For example, in the case of dental phobia, you can start with small amounts of treatment, and then gradually get used to it. If you have diagnoses typical for 40-45 years old that require treatment, but do not require it right here and now, then you can start by stopping caries, hygiene, then do something else, and then move on to serious interventions - if the indications allow . This plan usually suits male patients. For our part, we do everything so that you spend as little time as possible in the clinic and get the finished result in a minimum of visits. Dentistry has become much more humane over the past ten years.
When should you cancel your visit?
If circumstances arise that prevent you from visiting the dentist at the scheduled time, you can cancel the visit and reschedule it for a later date. It is better to inform the doctor or administrator about this as soon as possible so that it is easier for them to adjust the patient’s appointment schedule.
Cancel your visit if:
- you become ill with ARVI, influenza, or any other infectious or viral disease that may be contagious or interfere with treatment;
- your herpes has worsened;
- the nose is very stuffy (for example, due to allergies), and the stuffiness is not relieved with medication;
- with any increase in body temperature;
- when you feel unwell associated with an increase or decrease in blood pressure.
Nitrogen
The simplest thing we can suggest to you is to breathe nitrogen. The same thing that makes a person fearless and joyfully laughing at pulled out teeth. It doesn’t remove pain in any way, but it perfectly turns off its emotional coloring, and this is a large part of the perception of pain. Children often play “fighter pilots” with these nitrogen masks and think that going to the doctor is fun and cool (if the nurse works properly, of course, she should know child psychology). Nitrogen is worth trying at least once as part of general development if you have any doubts: it is quite safe and can make your life very much easier during complex interventions.
Tranquilizers
Next, you can use tranquilizers, but they should not be prescribed by a dentist, unless we are talking about a serious surgical intervention.
If you take your pills “to go to the tax office,” then keep in mind that they are needed only to get to the clinic (and not inside during the intervention) - and you definitely need to tell the doctor about them, otherwise a lot of interesting things await you at diagnostics and cross-reactions with other drugs. Our patients come on benzodiazepine medications - they help overcome dental phobia and generally get to the doctor. It is better not to drink before visiting the dentist. Alcohol will greatly interfere with the doctor’s proper work. And it also enhances the effect of some drugs, changes some, and reduces others. On top of everything else, you probably don't want the local anesthesia to turn off at a random moment, just when you have a foreign object in the doctor's hands in sensitive tissue.
Of course, there are situations when we work with “date” patients. There are a number of diseases in which the pain becomes more active in the evening, and the patient is already in a state close to calling his ex. If emergency intervention is required, it will be provided. But if the situation is planned, for example, the patient comes in an altered state of consciousness for hygiene, we will most likely refuse him.
Situations often arise when a patient drinks a mild painkiller available at home, it is not enough, and he washes it down with alcohol just to have enough strength to get to the clinic. When the patient accurately reports the dosage of alcohol and lists the medications taken without unnecessary questions, in general we are ready to understand him and meet him halfway. But just remember that this may prolong the diagnosis by half an hour and greatly worsen the sensations during treatment.
But after dental intervention, you can already wave a stack, if the doctor allows it.
Local anesthesia
We choose the articaine series as the safest in terms of duration/quality of action, possible side effects, and potential allergic reactions.
If you are afraid of injections, don't be afraid. They are not felt. Some doctors first use gel anesthesia, and then insert a syringe needle with an anesthetic into this place. In our clinic we have needles of 27-30 gauge (this is the outer diameter from 0.5 millimeters to 0.3 millimeters), this is another advantage of expensive paid medicine. By the way, the insulin needle starts with 26 G, that is, with 0.46 millimeters of outer diameter with a lumen of 0.26 mm. Injections with such needles can be done without application of anesthesia; you still won’t feel anything. Well, we also have a device that greatly speeds up and simplifies this process. If you don't tell what's going on, patients don't notice. This is where we really
to be afraid of practicing dentists: they are able to give an injection to any person without him even feeling or recognizing it.
Local anesthesia perfectly cuts down the necessary bundles of nerves nearby. If the intervention is serious, you will have a lisp until the next morning. If not, you simply won’t feel a couple of teeth and part of the gums for a while. Nerve problems are extremely rare as side effects. Extremely rare - if a doctor comes across something like this in 20 years of practice, then he won the lottery. More precisely, he lost. There are also cases of “Doctor, you gave me anesthesia a week ago, today my legs are paralyzed” - this is not for us, but the dentist can seriously write out a referral to a psychiatrist in such a situation.
Needles thinner than 30 gauge are used extremely rarely, as they lose mechanical strength. For some types of deep local anesthesia, a thicker needle is needed to push the tissue apart: it requires elasticity, that is, a larger diameter. In this case, the gel will still be used.
We have a rule: we spend as much time as possible on pain relief. You may not know, but therapists really don’t like symptoms with pain with limited appointment time. In our country, it’s hard to find the source of pain: in some cases it takes up to an hour just to find the cause and relieve the pain. Therefore, when we have a patient with a telephone history of acute pain, we do not limit the time for the appointment. If this is a regular client of the clinic, then it is normal for the doctor to go out just for him. If this is an emergency primary patient, then we leave a long pause between appointments. If this is one of the last appointments (and our doctors work for half a day), then we transfer the patients further to another doctor, and this one deals only with the patient with pain - as long as necessary to solve the problem. It is important to note here that a clinic patient with acute pain is actually a signal that treatment or preventive observation is not going well, because this is not the case in the plan. On the other hand, primary patients with acute pain have the unpleasant property of disappearing after we remove the primary symptom and still offer treatment. The worst thing is if the primary patient with acute pain made an appointment, but did not show up and did not tell anyone. If he warns you and doesn’t come, that’s normal. But if we prepared resources, cleared the doctor’s schedule, but he didn’t arrive, that’s bad.
What is dentophobia?
Dentophobia (dental phobia) is the fear of contact with a dentist and the fear of visiting a doctor’s office. A person is sick with dental phobia if he not only says: “I’m afraid to go to the dentist!”, but experiences panic fear. With dental phobia, arguments about excellent anesthesia and the professionalism of the doctor do not work. The patient is simply physically unable to cross the threshold of the dental office, even despite the unbearable toothache.
Difference between fear and phobia
Few of us will find the news about the need to visit the dentist good. The fear of dentists lives inside everyone. Even despite the achievements of modern dentistry, the feeling of fear of the dentist overcomes everyone, regardless of age, gender and profession. However, fear and phobia should not be confused.
Fear is a natural state of our body that overcomes a person under potential danger or uncomfortable conditions. A phobia is a pathology that occurs against the background of vegetative disorders and the inability to realistically assess the situation.
A phobia is not just a very strong fear, it is a much more complex phenomenon. This is a symptom of a neuropsychic disorder. This means that if not treated in a timely manner, the development of the disease can cause mental disturbances.
What exactly is the patient afraid of? TOP 10 fears.
According to the results of a statistical survey conducted in the UK, the largest number of people who suffer from dental phobia are afraid of not having their teeth treated; most of them answered: “I’m afraid to remove a tooth!” Among other frightening factors (as their prevalence decreases) were:
- fear of pain from teeth drilling;
- fear of giving an injection;
- fear of feeling a sharp pain syndrome (since the patient does not see what is happening in his mouth);
- fear of the sound of a drill;
- fear of dental office attributes and instruments;
- fear of a white coat, the sight of a doctor;
- fear of postoperative recovery;
- fear of side effects during treatment;
- fear of showing the doctor bad teeth, his reactions and comments.
Above are the most common fears of a person with dental phobia. However, in practice, unexpected, seemingly absurd fears of patients are also described, for example, the fear of suddenly dying in the dentist’s chair.
Types of dentophobia
The main classification of the disease reflects the congenital and acquired forms of the disease. In practice, cases of hereditary dental phobia are described, from which all family members suffer.
- Congenital dental phobia. The rarest type of dental phobia, which is not associated with any unpleasant experience. A person experiences an inexplicable fear of visiting the dentist and any manipulations in the mouth. After the first visit to the dentist, the patient may overcome his fear and forget about it, or the situation may worsen due to the formed negative attitude towards doctors in general.
- Acquired dental phobia. A common form of the disease, which affects every third patient. Very often a person experiences fear of the doctor and everything connected with him, due to previously received negative experiences. This form of dental phobia is based on a healthy property of the psyche - to protect us from everything that previously posed a threat and caused unpleasant emotions. Once receiving an alarm signal, the human brain responds not only to the same stimulus, but also to similar circumstances.
- Imaginary dental phobia. This disease affects those who have never visited a dentist. The reason for the development of imaginary dental phobia is an inadequate assessment of the treatment process, supported by a wild imagination. Usually a person only has to overcome his fear once, and after a successful visit to the doctor, the symptoms of the disease completely disappear.
Pathological fear of dentists is also distinguished by its severity:
- light. A person experiences slight anxiety at a doctor's appointment. There is no need to reassure the patient; he copes with emotions on his own.
- average. The patient experiences anxiety not only during the procedure, but also after the end of therapy. Helping the patient - correcting the emotional state. The doctor can tell you in more detail about the features of the manipulation, increase the degree of self-confidence through a friendly conversation;
- heavy. An adult visits the dentist only in the most extreme cases, interferes with medical procedures in every possible way, and does not adhere to the dentist’s recommendations. In this case, you cannot do without taking special medications and psychotherapeutic treatment.
The most difficult thing to talk about is congenital dental phobia, because a person is not born with the understanding that the dentist is dangerous. The baby is only capable of primitive and large-scale reactions, and it doesn’t matter what caused the discomfort. Congenital is usually called increased anxiety and fearfulness, which is caused by the child’s developmental characteristics and the functioning of the nervous system. Excessive emotions in a newborn can also be caused by a high level of hormone-transmitters in the blood.
Why is dental phobia dangerous?
In itself, fear of the dentist does not pose a significant threat to the patient. A patient who does not visit a doctor out of fear is able to live a full life. However, if there are problems with teeth or gums, the patient has a serious reason for concern, and at the same time a real threat “looms.”
A sore tooth or gums are sources of infection. Pathogenic bacteria from the oral cavity enter the gastrointestinal tract and other organs. If caries is not eliminated in time, it becomes complicated and develops into periodontitis, which is accompanied by the accumulation of pus that can cause blood poisoning.
Another point is aesthetics. Diseased teeth become dark and decay; a person ceases to look attractive. He begins to be ashamed of his teeth, stops smiling, talking, and loses self-confidence. The patient's quality of life decreases sharply.
And finally, the financial aspect. If a person puts off visiting a doctor for too long, there is a high probability that solving the problem in the future will require serious financial investments.
Practice shows that previously the fear of dentists was so pronounced that it was impossible to carry out full dental treatment. Patients were afraid of any procedures in the oral cavity and even refused to install dentures.
Sedation and drug-induced sleep
This is propofol, a hypnotic that causes a feeling of deep moral satisfaction and helps you sleep.
True, it is better not to use it without the supervision of an anesthesiologist; it can end sadly, as the experience of some musicians proves. You may have experience receiving supervised propofol if you have had an EGD (“bowel swallow”) or colonoscopy under sedation. Propofol does not anesthetize you in any way, it simply erases your memory. That is, it will still hurt, but you won’t remember it. Propofol in small doses is conveniently combined with local anesthesia: the patient can fall into a shallow sleep, enough to lose the will and follow simple commands like “open your mouth.” At this point, you should seriously think about the use of propofol by various intelligence agencies and begin to really be afraid of dentists for the second time. Alas, it cannot be used as a “truth serum” - the patient is not able to think enough in his sleep to answer coherently. As a plus, you will get an incredibly good mood that will last a long time after the intervention. In small doses, propofol works as a sedative (you won’t care about anything), in medium doses it puts you into a shallow sleep, then the sleep becomes deeper, but does not turn off the nervous system. Anesthesia shuts down the nervous system. This is the best way to do something serious surgically, because the patient will be unconscious and will not twitch in response to even thoughtful sawing off of the arm. You can turn off either the lower part of the body or the entire body at once, because, alas, there is a large nerve node on top. Anesthesia very much depends on the active substance. We use sevoran, here is more about it - as well as about other ways to turn off consciousness in dentistry. Briefly: safe, children allowed, no “helicopters”. We use sevoran with children using natural breathing through a mask (shallow anesthesia); for adults, the optimal choice is propofol and local anesthesia.
Just know that we have it all. It is because of those who fear the “drill” more than anesthesia that operating rooms with oxygen are built in expensive clinics.
Or we can give you a referral to a psychotherapist (don't be alarmed) so that he can give you antidepressants for dental treatment. This also happens, but usually rarely, because a Russian person is not only afraid of a psychotherapist (psychiatrist), but consciously avoids them. By the way, you really should be wary of psychotherapists at the end of March, June, September and December, whose quarterly plan for hospitalizations is on fire. Kidding.
Both in the case of anesthesia and in the case of sleeping under propofol, there is a slight chance that the drug will not act as it should. When the body is immobilized, and you feel everything - the cases are described. There was a case when one foreign patient showed an atypical reaction to propofol - it did not cause the characteristic retrograde amnesia. Her son arrived with a machine gun and said that he would now take the surgeon to teach him manners. The conversation was very unpleasant, we managed to defend the doctor. The anesthesiologist's surgeon also failed.
Let's do it again
- It’s normal to ask for anesthesia for any fear.
- It is normal to request anesthesia for discomfort that interferes with treatment (for example, an instrument rubbing against your teeth or tickling during hygiene).
- It’s normal to ask to see how instruments are sterilized.
- Asking for an explanation of how each device works in a doctor’s office is normal (just don’t abuse this opportunity or warn in advance that you need a tour, there are patients further away).
- It’s okay to cry in the office if you feel like it. This is part of the compensation for fear, our body does this. Nothing unusual.
- It’s normal to reschedule your appointment to gather your strength. Sometimes this is necessary due to bowel behavior.
- It’s normal to know the meaning of every doctor’s manipulation.
- Bringing someone with you to hold hands is at the doctor's discretion.
Willpower is trained.
If you can conquer fear in small things, then it will be easier to defeat fear in large things. A patient who was previously embarrassed to go to a urologist or proctologist, and then stopped, will most likely accept the dentist calmly. Fear is normal. Doctors see fearful patients every day. We don’t laugh at this, this is the patient’s usual state. The fact that you came is very good, and it is a sign of respect for us, because you were not afraid to come to us. This is not a legend for patients; doctors really have respect for those who simply sincerely explain what is wrong with them. Without playing detective, as often happens.
Fear is easier to bear in a good physiological state. It’s better to get enough sleep, come in the morning (before you’re tired), and not be very hungry (unless your stomach is “twirling”). If you have something important to do after the doctor, it’s better to reschedule either the appointment or the case.
If you are afraid to tell your doctor something or don’t want to share your fears with him, this is a sign of not the most professional doctor. The doctor must recognize the patient's condition and ask him to tell him what is bothering him. The dentist does not start treatment right away, but tells what will be done and how (if this is appropriate, that is, if it is not dental phobia in certain forms), talks about the equipment, shows sterilization and talks about other safety aspects. In our application, when making an appointment, the protocols of each future intervention are automatically uploaded: you can read in advance what exactly the doctor will do and in what order, so that you can ask questions on the spot.
What to do if a teenager is afraid to go to the dentist
A teenager trusts adults less, it is impossible to distract him and it is difficult to convince him of anything. You need to establish a trusting relationship with him and show respect for his choice.
It is advisable to follow these tips:
- Be sure to condemn all the procedures that have to be done so that he is not frightened by the unknown. Most fears go away after a detailed discussion of the upcoming situation.
- If a guy or girl refuses treatment and the situation is not urgent, do not insist on visiting a specialist. Familiarize them with the consequences of their refusal in detail and allow them to make a choice. After discussion, the teenager shows interest in treatment himself.
- Create positive motivation in your teenager for dental treatment and careful oral care. Explain to him the importance of healthy teeth and a beautiful smile for his future.
- Until the age of fifteen, you can always be in the dentist's office with your son or daughter and support him. If they are older, then the presence of parents is possible only with their consent.
- Choose a doctor who can establish good contact with the teenager. He must take into account the teenager’s opinion and communicate with him as an adult, and not just listen to the parents’ opinions and fulfill their wishes.
If you cannot cope with the situation on your own and the child continues to be afraid of the dentist, you should contact a psychologist. He will provide him with professional help and help him cope with fear.
Really dangerous situations
In fact, the most dangerous thing you can do in a doctor's office is touch an instrument or the hand that holds the instrument, or try to throw the doctor off balance by grabbing his leg.
If at this moment you have a diamond disk in your mouth (like an angle grinder, only small), you can get hurt. We won’t cut through to the brain, of course, but it won’t be much fun, because bleeding in the sublingual space is difficult to stop. Fortunately, in 2021 these discs are probably used only in regional compulsory medical insurance clinics. But if you do this with a drill, you will very quickly end up with a new unplanned hole in your gum or cheek. We really don't like it. In my youth, I had a situation where I damaged a patient’s lip with an old polishing instrument, but visually it seemed that she was walking around with herpes while it was healing. It was extremely embarrassing, and this was my first negative review - it is still hanging out on the Internet. Therefore, believe me, I would not want my doctors to do the same, even by accident. I have the opportunity to purchase a tool for clinics that has protection against going beyond the designed axis: you can configure the drill to automatically turn off when the doctor’s grip changes (for example, if someone is afraid that the doctor will simply drop the drill in his mouth) and if resistance arises along the axis of rotation (this is when soft tissue or hair gets wrapped up and slows down the tool, usually the first millimeters of error). That is, in our case, the gum can only be drilled purposefully at a calculated angle; if the patient gets hurt or the doctor has a heart attack during the drilling iteration, the device will turn off. But not everyone is like that.