The use of veneers to enhance the aesthetics of a smile is becoming an increasingly popular dental service. Various materials are used as materials for the manufacture of artificial onlays - composites, porcelain, zirconium dioxide. A special place in this list is occupied by dental ceramics, which makes it possible to create veneers for a metal base and solid products, including feldspathic veneers.
A distinctive feature of ceramics used in dentistry is the absence of kaolin, which is vulnerable to coloring pigments. The chemical structure of the material includes two-thirds feldspar and one-third quartz, the combination of which with additional trace elements ensures high strength of the finished products.
Feldspathic ceramic veneers are made from a powder mass obtained by firing and instantly cooling a workpiece that is subjected to grinding. The flexural stability index is 30-40 mPa, which, combined with high aesthetic properties, allows the composition to be used for dental prosthetics in both the chewing and anterior areas.
Indications
Ceramics are used to make aesthetic dentures with or without a metal frame. With its help you can make:
- thin veneers less than 0.6 mm thick and regular veneers (only made of glass ceramics);
- occlusal veneers;
- inlays and crowns;
- endocrowns;
- root posts (made of oxide ceramics);
- stump pin inlays (with a pin made of oxide ceramics);
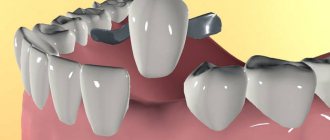
- bridges supported on inlays (with a frame made of oxide ceramics);
- three-unit bridge-like dentures, as well as long-length bridges;
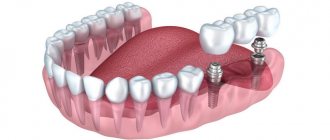
- dental implants (made of oxide ceramics);
- abutments;
- artificial teeth of removable dentures (made of glass ceramics);
- gingival part of conditionally removable and fixed dentures (glass ceramics).
Classification by purpose
Dental ceramics are used for various purposes. Depending on this, it is divided into frame, monolithic and facing. Frame – used for the manufacture of crowns and bridges. Facing – metal (cermet) or ceramic (metal-free ceramics) frames are veneered. Monolithic – designed for making complete dentures.
The requirements for these varieties are different. The framework ceramics must be very durable, the veneering metal-free ceramic crown must have good aesthetic characteristics and reliable adhesion. Monolithic ceramics are generally the strongest of all, so require less invasive preparation and provide longer prosthetic life. Only lithium oxide and disilicate glass ceramics are suitable for its manufacture, while aluminum oxide requires additional lining due to its high abrasiveness.
Contraindications to the use of ceramics
- Low-strength ceramics cannot be used under increased occlusal loads, including in patients with bruxism.
- It is prohibited to manufacture ceramic dental bridges if their bending strength is less than 350 MPa.
- Lithium disilicate ceramics are not suitable for the manufacture of bridges longer than three units.
- The material is also not used for deep subgingival preparations if adhesive fixation is required.
- It is contraindicated if the preparation depth is insufficient.
- It is not used if there is a need for subsequent non-destructive removal of the structure, with the exception of screw ones.
Indications and contraindications
Installation of veneers on the dentition is recommended if the following factors are present:
- Aesthetic defects of the frontal units, characterized by the presence of irregularities, cracks and chips, as well as abrasions on the enamel surface;
- Detection of hypoplasia – a pathology that negatively affects the development of dental tissue;
- The problem of a “gummy” smile, which requires not only tooth restoration, but also correction of the gum line in the contact area;
- Increased susceptibility to temperature or mechanical irritants;
- The need to eliminate diastemas, as well as mask other problems associated with the shape or appearance of the units.
The most common reason for prosthetics is the patient’s desire to improve the aesthetics of his smile, accompanied by the impossibility of using other enamel whitening techniques. At the same time, it is important to take into account the influence of negative factors considered as limiting contraindications:
- The presence of non-retinated units in the row;
- Diagnosed bruxism;
- Insufficient thickness of the enamel coating;
- Advanced caries requiring additional treatment;
- Damage to more than 60% of the tooth surface;
- Periodontal pathologies;
- Previously installed extensive fillings.
The decision on the possibility of restoration using feldspathic veneers is made based on the results of a comprehensive examination conducted in a clinical setting.
Advantages and disadvantages of ceramics in dentistry
Ceramics make it possible to produce dentures that are almost impossible to distinguish from real teeth. In this indicator, it outperforms amalgams and metal alloys, unlike which it also has low thermal conductivity. It can be used to make dentures for vital teeth. Such designs do not have the disadvantages of metal dentures, however, prices for metal-free crowns are always higher. In addition, ceramics are more fragile than metal, and therefore require careful handling during preparation and do not tolerate sharp transitions.
Composite materials are in no way inferior to ceramics, but they have an undeniable advantage. It is more durable and has increased biocompatibility, since it does not contain organic components. Ceramic materials have record color and wear resistance, as well as bending strength, but they are more fragile than composites. Therefore, some authors recommend choosing composite materials for implant-supported prostheses.
Among the obvious disadvantages of ceramics is low repairability, especially in the oral cavity.
The evolution of prosthetics. Triumph of ceramics. Part two
Daria Bendarskaya journalist Dental Magazine
The idea of using porcelain in the manufacture of dentures later received active development, not only in the Old World, but also in the New World: there are no geographical boundaries for ingenious solutions.
Personal motivation as the engine of progress
In Europe, Pierre Fauchard's main followers in working with porcelain were his two compatriots - the pharmacist Alexi Duchateau and the dentist-surgeon Nicolas Dubois de Cheman.
Duchateau himself wore dentures made of ivory and learned from his own experience that it was impractical, unhygienic and unaesthetic: the porous bone absorbed saliva and the remains of liquid food, acquired a dirty color over time and caused a strong bad breath. So the pharmacist was looking for a replacement denture and, after a series of experiments, with the help of specialists from a porcelain factory in Saint-Germain, he made his first porcelain denture.
As for Dubois de Cheman, he managed to solve the problem of porcelain shrinkage during firing. In 1789, he received a patent in England for porcelain teeth, the material for which was supplied to him by the English company Wedgewood. The dentures were made by sintering feldspar, silica and kaolin. True, at first the dentist himself called his products not porcelain, but mineral. The fact is that porcelain was treated as a very fragile material, and such a reputation for porcelain would only harm Dubois de Cheman in popularizing his invention. For comparison, if in 1797 3 thousand sets of complete removable dentures were sold, then by 1804 - already 12 thousand.
Portrait of Dubois de Chemans. Source: wikimedia.org
Complete removable dentures made of gold and porcelain. Source: flintsauctions.com
At the beginning of the 19th century, dentist Giuseppe Fonzi developed a technology for making porcelain dentures with metal pins. This technology was a breakthrough in prosthetics. The design made it possible to make complete removable dentures for the upper and lower jaws. Each porcelain tooth, which was secured in a gold prosthesis using a platinum pin, had its own independent “suspension.” The pins themselves enabled the dentist to fine-tune the dentures individually for each client. And, importantly, the palette of shades of porcelain teeth made it possible to choose the most suitable option so that the prosthesis looked completely natural. By the way, Giuseppe Fonzi, during his cruise through Europe in 1824-1825, designed and installed prosthetics for Alexander I. They were incredibly expensive for the Tsar’s treasury. And the autocrat became the first Russian emperor to acquire dentures.
At the end of the 19th century, among private practitioners abroad and in Russia, the practice of cutting out deposits from porcelain pieces and cementing them into previously prepared carious cavities was popular. In the 1870s, the above-mentioned dentist Land developed a special mass for inlays, but its disadvantage was that it had a high melting point and exhibited significant shrinkage during firing. A few years later, in Germany, in Dresden, Porcelain Enamel was created, which was used for a long time all over the world.
On the other side of the ocean
The mid to late 19th century was a period in the history of dentistry when experiments with ceramics progressed with varying degrees of success. New inventions were required for this direction to receive further active development. Dentists tried to combine the best qualities of two materials - ceramics and metal, to find the optimal technology and solve the problem associated with the strength and aesthetics of ceramic dentures on a metal frame.
Prosthetics was actively developing not only in Europe, but also in the USA. Industrial production of artificial porcelain teeth in the country began in 1825. In 1884, dentist Broke developed a porcelain bridge design in which a platinum-iridium alloy was covered with a ceramic shell. Although the technology itself was not widely used due to the fact that prosthetics were quite difficult to manufacture and were not durable, this technology was used in Russia until the beginning of the 20th century.
In 1885, a method for custom-making a pin artificial tooth was patented, in which a porcelain veneer was sintered directly onto a platinum post. The prerequisite for the manufacture of a porcelain shoulder crown, called the "jacket crown" or "jacket crown", was the use of platinum foil by dentist Land when modeling ceramic crowns in 1887. Later, he also described a method for making porcelain crowns using foil directly using a kiln. With some modifications, this technology is still used today. Land had many opponents who believed that such a fragile material as ceramics could not be used to create artificial teeth. But his students proved the promise of the innovative methodology.
By the end of the 19th century, two main directions for the use of ceramics in prosthetics had been identified: cladding of metal frames (metal-ceramics) and metal-free ceramic structures.
Mold for making dentures. France, early 20th century. Source: medicalantiques.jalbum.net
Ideas and technologies
In Europe, jacket crowns have become widespread since the 1920s, using gold as a frame material. In the 1920s and 1930s, new ceramic dental masses of American, English and German production appeared, as well as new kilns, supplemented with silit heating elements. In 1925, dentist Albert Le Gros described the main stages of using ceramics in prosthetics.
In 1937, on the basis of the Leningrad Porcelain Factory. M.V. Lomonosov opened a factory of teeth made of porcelain and dental cements. Artificial teeth were produced in 18 different shapes and 9 colors. In 1947, the Leningrad Union Plant of Dental Materials was founded. At the end of the 1950s, the first Soviet porcelain mass FIL-1 was created with a melting and firing temperature of about 900 degrees. This temperature made it possible to use gold foil for firing. The industrial production of artificial teeth from ceramics in the country was in full swing: equipment was modernized, technology was improved, and production volumes grew. At the same time, the industry for the production of artificial teeth from plastic developed.
At the end of the 1940s, significant progress was made in improving the technology for making artificial teeth from ceramics. In the 1960s, research and experimentation began on creating ceramic compounds for single crowns; The technology for working with ceramics was significantly improved; they began to fire it in a vacuum. A technology for strengthening ceramics using aluminum oxide has also been proposed. During these same years, a patent was received in the United States for a gold-based alloy with a low melting point for the manufacture of a metal frame for porcelain crowns and bridges.
Thus, the second half of the 20th century became the era of metal-ceramics in prosthetics.
Students, future dentists, at work in the prosthetics laboratory. University of Otago. New Zealand. 1949 Photo source: Elaine Donaldson
Porcelain teeth. Circa 1925.
Aluminum mannequin for prosthetics. 1930s Photo source: atlasobscura.com
Was, is and will be
Despite the widespread use of metal-ceramic structures and acrylic, the idea of using metal-free ceramic structures has not lost its relevance for dentists. Since the 1980s, ceramics have been used to make veneers, inlays/onlays, crowns and bridges for the anterior teeth. In the 1990s, newer and more precise technologies were developed to create ceramic masses and luting cements. The fact that gold and metal structures began to lose their aesthetic appeal also played a role in the popularization of ceramic dentures: today patients want their dentures to be not only reliable, but also to look like real ones. Thanks to new materials and techniques, modern all-ceramic prostheses meet these requirements. But work to improve ceramics continues: the goal is to reduce the hardness of the material in the surface layer and its abrasive effect on natural teeth.
So ceramics remains one of the most popular materials in dentistry. Statistics confirm this: the need for ceramic prostheses increases every 4 years by approximately 50%.
Moving on to the first part...
Empress metal-free ceramics
Empress ceramic technology is characterized by strength, durability and aesthetics.
Empress ceramics contain a large number of leucite crystals, which has a positive effect on its strength. The material from which it is made has similar properties to the enamel of natural teeth and has good color and light transmittance. This allows the orthodontist to very accurately select a color that matches the color of the teeth surrounding the crown.
As the name suggests, the crown is made by pressing. Using a cast plaster model that is an exact replica of the patient's teeth, the technician models the crown, reproduces it in wax, then places it in the porcelain casting system. A special ceramic mass is heated in a kiln and poured into a mold at high temperature and under pressure, while the wax is burned out. Afterwards, the almost finished crown is painted and covered with additional ceramics (or excess is removed), glazed and fired. The result is a custom-made crown with superior aesthetic and functional characteristics.
Advantages of Empress ceramics:
- Fully biocompatible material. No allergies;
- Naturalness. Complete imitation of the shape and color of teeth.
Empress is an earlier version of E-max technology and is gradually replacing one technology with another in the laboratory. E-max is a further development of Empress technology.
Receiving technology
Powder obtained from ceramic mass using a special technology is used as blanks for creating prostheses .
The mixture is fritted (primary firing). The resulting product is called “frit” and is a fine-crystalline dispersion of quartz with fillers.
Due to the rapid cooling, the frit has many cracks that allow it to be ground into a fine powder. Fritting also promotes uniform distribution of components throughout the material.
Ceramic mass, which serves as the starting material for the manufacture of prostheses in laboratory and factory conditions, exists in the following forms.
- Powder made from frit. It is used by dental technicians in laboratory conditions (mixed with water), as well as in factories for the production of dentures. This form of the original ceramics is called conditioned.
- Tablets compressed from powder. They are used in particular for the manufacture of crowns using the injection molding method.
- Solid machine blocks. The term “machine” means that these blocks are designed for cutting crowns and inlays using special milling equipment using CAD/CAM technology.
- Infiltrated ceramics. It consists of a powder filler and an amorphous lanthanum glass matrix.
This is interesting: Why do you need to reline a removable denture: methods of carrying out the procedure
The video shows the process of casting and pressing ceramics.