Removable structures
Very easy to use, they can be removed independently during meals, hygiene procedures, and if therapeutic dental treatment is necessary. Also easy to install back. There are several types:
- Polymer transparent retainers-aligners, reinforced with a metal arch. They fix the position of the teeth along the length of the jaw and are invisible to others. Used constantly, excluding food intake and care procedures.
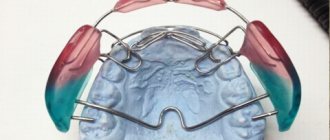
- Orthodontic plates consist of a plastic base and fixing metal elements. Basically, the designs are worn at home and put on before bed.
- Positioners keep the teeth in the correct position and restore the tone and density of the gum tissue. Made from elastic polyurethane, they are easy to use and do not cause allergic reactions. Show high effectiveness for minor occlusion disorders.
Removable orthodontic appliances are made within 3-7 days using individual impressions.
Reorganization of periodontal tissues
During orthodontic treatment, the space of the periodontal ligament expands and collagen fibers break, making it possible for the orthodontist to move the teeth.
Even if dental movement is stopped before the orthodontic appliance is removed, restoration of normal periodontal structure will not occur as long as the tooth remains in a rigid ligament with neighboring teeth, and also if it is connected to a rigid orthodontic arch. Since the teeth cannot respond to the chewing load individually, reorganization of the periodontal ligament (PDL) occurs within 3-4 months, and the slight mobility present gradually disappears when the hardware is removed.
The gingival fiber system is also destroyed during orthodontic tooth movement and must be reconstructed according to the new position of the teeth. Collagen and elastic fibers are reconstructed in the gums more slowly than in the PDS itself. The formation of a network of collagen fibers inside the gum is usually completed within 4-6 months, and the reconstruction of elastic fibers above the alveolar process is even slower, so that even a year after the removal of orthodontic equipment, forces capable of dislodging the tooth may remain.
Fixed retainers
They are represented by a thin metal arch, which is point-fixed with composite material to the inner surface of each tooth. They are installed immediately after the braces are removed, the adjustment time does not exceed a week. It must be remembered that the results of corrective treatment can only be maintained by constantly wearing retention splints! Neglecting the orthodontist's recommendations leads to deformations of the dentition and bite.
Installation Features
Retainers are installed on the day the braces are removed. Fixation is carried out after polishing the enamel and/or professional hygiene. For better adhesion, a special composition is applied to the surface of the teeth. The installation of removable devices is preceded by taking impressions and making mouth guards, positioners or orthodontic plates in the laboratory.
Why is retention needed at all?
- Reasons why orthodontic treatment requires consolidation of the result:
- treatment with braces affects the periodontal tissues (bone and mucosa), and it takes time for their reorganization after removal of the device;
- because after treatment, the teeth are in an unstable position, pressure from the soft tissue creates a constant danger of relapse;
- Growth-related changes may affect the outcome of orthodontic treatment.
Even if the teeth are in a stable position and if no further growth is expected, retention is still essential until the reorganization of the gingival and periodontal tissues is complete.
General care recommendations
The retention period is the most important and integral part of the technology for correcting occlusion. The success of treatment largely depends on the patient’s conscientious adherence to the doctor’s recommendations.
- Before fixing them on the teeth, removable retainers are rinsed with a soapy solution; in the morning and before bed, it is recommended to clean them with a special brush with a low-abrasive paste. Once or twice a week, removable structures are soaked in an antibacterial solution. To protect against damage and deformation, tires should be stored in a lockable case.
- Oral care with permanently installed retainers is carried out using traditional methods. For thorough cleaning of mineralized plaque and food debris, threads, brushes, and irrigators are used.
- An indispensable condition for oral health is visiting the orthodontist at least twice a year. An emergency visit to the dentist is necessary in case of discomfort and pain, as well as in case of damage to the aligners, plates or breakage of the metal arch.
Types of retention devices
As we mentioned above, a retainer can be:
- in the form of a wire fixed on the linval surface of the front teeth;
- in the form of a mouthguard - a kind of cover for teeth made of polymer that follows the shape of the teeth. Today, silicone retainers are in great demand; they are practically invisible on the teeth and do not cause any particular inconvenience during use.
While wearing a retainer, it is important to maintain careful oral hygiene and use specialized devices and products recommended by your doctor.
Don't be alarmed if you don't see visible results from wearing your retainer. His work, although not visible, is very important. Over time, the teeth will take a stable position, and the moment will come when your doctor will inform you that the device can be removed and you will finally become the owner of straight and strong teeth.
The Smile Studio specialists instruct their patients that neglecting retention devices is unacceptable. This can ruin the entire result of long-term treatment. So listen to the professionals, and your gorgeous, charming smile will stay with you forever.
Advantages of the Alfa-Vid clinic
The Alfa-Vid Dental Center invites patients in need of bite correction to a free consultation. At the initial appointment, the doctor will carefully examine the oral cavity and, depending on the clinical case, will offer the best option for retention treatment. We guarantee:
- compliance with international quality and safety standards;
- individual approach;
- comprehensive problem solving.
If necessary, the patient has access to emergency assistance from doctors of related dental specialties (therapist, surgeon, etc.). The clinic is equipped with advanced European-level equipment, and dentists use high-quality materials in their work.
Removable retainers
Pros and cons of a removable retainer
The advantages of removable retention products are:
- the use of the device is not permanent—the patient himself chooses the time to use the device. The main condition is that this time is no less than 10 -12 hours;
- ease of use - the ability to remove the retainer yourself before eating or having an important meeting;
- Hygiene procedures are not difficult - brush your teeth and removable retainer twice a day with a toothbrush and toothpaste, after eating you need to rinse your mouth with warm water and install a retainer.
The disadvantages of using removable retainers are the following:
- Possible difficulties with articulation;
- the presence of a foreign object in the mouth often causes increased activity of the salivary glands;
- the need for frequent visits to the dental office;
- metal structural elements can provoke an allergic reaction.
Duration of use of a removable retainer
The time required to consolidate the result is individual for each patient. The duration of retention is affected by:
- complexity of the corrected defect;
- patient's age;
- duration of therapeutic treatment.
As a rule, the retention period lasts twice as long as the active period.
What is the procedure for removing retainers?
Removal, as well as fixation, of a non-removable retainer occurs only in the dental office.
There are certain arguments in favor of removing the retention device by an orthodontist:
- The metal arch is attached using a composite material and it is not possible to remove it without damaging the tooth enamel.
- Only the attending orthodontist can determine the end of the period of occlusion stabilization. Premature removal of the structure will eventually make all the efforts and time spent on correcting defects in the dentition (not to mention the money) in vain.
The procedure for removing the retainer is as follows:
- The retainer is removed using a dental bur, which removes the composite material that secures the metal arch to the lingual side of the teeth.
- The surface of the tooth at the site where the retainer is attached must be polished to eliminate possible roughness and minor residues of the composite material.
- The treated areas of tooth enamel are remineralized to eliminate their increased sensitivity.
The procedure for professional hygienic cleaning after removing retainers can be carried out only if the sensitivity of the tooth enamel is not impaired.
Abrupt abandonment of retention products is undesirable. Therefore, after removing non-removable retainers, the orthodontist will prescribe the use of a removable orthodontic structure - mouthguards, plates. Gradually reducing the time you wear the device will help avoid relapse.
Orthodontic screws
In practice, orthodontists more often use orthodontic screws to change the shape and size of dental arches, correct the position of individual and groups of teeth and bite.
An orthodontic screw is a factory-made mechanically acting element that is an integral part of the orthodontic apparatus.
The advantages of using screws are as follows:
1. The screws can be easily activated by both the patient and his parents.
2. The screws act with precisely measured force.
3. Screws can act in one or several planes simultaneously.
4. The two parts of the cut plate appliance with screw are more stable than the expansion spring orthodontic appliance.
5. The screws have different shapes and sizes, which facilitate their fixation in the base of the orthodontic apparatus.
6. Thanks to their design features, screws can move individual teeth, groups of teeth, dentitions and normalize the bite.
Depending on the purpose of use and design features, orthodontic screws are divided into 3 groups:
Group 1 – screws for moving individual or groups of teeth.
Group 2 – screws for normalizing the shape of the dentition:
a) for symmetrical bilateral expansion or contraction,
b) uniform symmetrical elongation,
c) uneven expansion - radial action (expansion of the frontal section is symmetrical and asymmetrical),
d) simultaneous expansion and elongation (uniform and uneven; symmetrical and asymmetrical).
Group 3 – to normalize the bite.
The force that is necessary to move teeth or change the shape and size of the dentition and normalize the bite develops when the screw is activated (unscrewed).
The screw body is usually made of nickel silver (nickel silver), and the drum (working part) of the screw is made of stainless steel.
Screws are classified by size: standard, medium, universal, microscrews and super microscrews.
The direction of activation on domestically produced screws is marked with a red dot, and on foreign ones - with an arrow. In the base of a removable orthodontic appliance, the screw is placed with the activation marking upward, so that activation occurs from bottom to top.
Orthodontic screws consist of a threaded main post and one or two drive pins. The main and driving pins have a common casing. The main pin has left and right hand threads. In the middle part of the screw there is a thickening - a drum - with four holes, which are designed to activate the screw.
The double-guide orthodontic screw (Fig. 28.1) consists of a rectangular body that has two identical halves. Inside the body there are three round longitudinal channels. The outer channels include 2 smooth guide pins, and the middle one has a double-sided thread and contains the screw itself. Either of the two guide pins is rigidly fixed at one end in the opposite halves of the screw body.
The screw with one guide pin is designed in the same way. Its body has 2 channels and 2 pins: one with a double-sided thread (screw), and the second - a guide (Fig. 28.2).
Rice. 28. Orthodontic screws with two guides (1) and one guide (2).
Screws with two guides are used for uniform expansion of the dental arch, and screws with one guide are used for unilateral lengthening of the dental arch, moving one or a group of teeth, etc.
The placement of a screw in the base of an orthodontic appliance made for uniform expansion of the upper jaw depends on the configuration of the palate or alveolar processes and the site of expansion. Most often, the screws are placed so that the first guide is designed between the midpoints of the oral surfaces of the first premolars (first primary molars). Less often - between the middle of the fangs. In this case, the cut of the apparatus passes through the middle of the hard palate (along the palatal suture).
Skeleton screws with one guide are made with a U-shaped straight bracket (Fig. 29.1) (guide) or with a curved one (Fig. 29.2).
Rice. 29. Skeleton U-Bracket Screws.
The latter is more consistent with the shape of the vault of the hard palate and is used on the upper jaw. Such screw designs are used to lengthen the frontal or distal parts of the upper and lower dental arches. The part of the screw with the bracket is located in the stationary part of the device, and the part that moves when it is unscrewed is in a small segment. When the spindle rotates, it slides along the guide along with the plastic sector and moves the tooth or teeth in the mesial, distal or vestibular direction
Radial or fan-shaped screws are used to expand the frontal portion of the upper dental arch. They can be symmetrical (Fig. 30.1) and asymmetrical (Fig. 30.2). When using such screws, the distal border of the base of the orthodontic apparatus ends at the level of the limiter hinge. Domestic and foreign companies produce two types of symmetrical fan-shaped screws. In one design, the drum and limiter are made as a single unit, and in the second design, the limiter is made separately. When inserted into the design of an orthodontic appliance, the stopper arms of such a screw must be moved apart to a width determined by the doctor.
Rice. 30. Fan-shaped (radial) screws.
Screws for simultaneous expansion and lengthening of the upper dentition (three-dimensional) are produced in two types: with two working drums and three. A screw with two working drums ensures uniform expansion and lengthening of the dentition (Fig. 31.1), and when using a screw with three drums, lengthening and uneven expansion of the upper dental arch on the left and right is possible (Fig. 31.2).
Rice. 31. Three-dimensional screws.
The domestic industry produces three-dimensional screws with independent expansion. In such screws, the drum, which lengthens the frontal section of the upper dental arch, is connected to the screw body with a hinge and, if necessary, can be shifted to the left or right side. In this case, there is an expansion of the frontal section of that side of the dental arch under which the screw is displaced (Fig. 31.3).
Push screws are available with a flat working part and a round one. The first are shown for corpus vestibular movement of individual teeth, and the second - with rotation around an axis (Fig. 32).
Rice. 32. Screw pushers.
Intermaxillary screws include the Weise screw, which is used in Wunderer activators for the treatment of mesial occlusion (Fig. 33).
Based on the amount of expansion when the screw is activated a full turn, the following types of screws are distinguished: with an expansion of 0.8 mm, 0.7 mm, 0.4 mm and 0.35 mm and a total expansion of 4 to 10 mm.
Activation of orthodontic screws is carried out by unscrewing the drum. Activation begins after the child has become accustomed (adapted) to the orthodontic apparatus. The activation mode is selected individually - the screw is activated within a period of 14 to 3-4 days.
Activation usually begins on days 7-14, gradually moving to activation on days 3-4.