2193
The most common method of attaching bridges is to secure them with full crowns placed over the abutment teeth.
To do this, the latter are sanded off on all sides, which leads to a deterioration in their condition and an irreversible loss of aesthetics.
There are, however, other, more gentle ways to attach the MP. One of them is fixation of half-crowns.
General overview
A partial crown is a small, non-removable orthopedic structure that covers four surfaces of the tooth - oral (lingual), two proximal (lateral) and chewing (incisal).
The vestibular (buccal, labial) surface remains uncovered. Typically, partial crowns are placed on premolars and front teeth. They are sometimes called “three-quarter teeth,” although they actually cover 4/5 of the tooth surface.
Most often, half-crowns are used as supporting elements of bridge or clasp prostheses. Unlike full crowns, they do not impair the aesthetics of the supporting tooth, the vestibular part of which remains intact.
Sometimes half-crowns are used as fastening elements for splinting structures.
In general, there are quite a few types of partial crowns. There are ceramic structures similar to veneers. They cover the tooth from the vestibular side and are applied solely to improve the aesthetics of the defective tooth. Therefore, it is more correct to call this type of crown “veneering.”
There are “seven-octagonal” designs that leave only the mesiobuccal cusp open. Due to the relative rarity of such designs, this article will discuss only the traditional types of partial crowns – “three-quarter” crowns.
Half-crowns are made using casting from stainless steel, KHS, gold and silver-containing alloys (silver-palladium, gold-platinum).
To secure the cast product on the tooth, the latter is prepared (ground) on 4 sides to form U-shaped grooves on the occlusal, distal and medial surfaces.
They play the same role as the labial side of a full crown. The grinding thickness should be no less than the thickness of the metal - about 0.3-0.5 mm.
The design of the half-crown structure in each specific case is determined by the doctor, taking into account the clinical picture and the general principles that apply to this type of orthopedic products.
The “three-quarter” structure is attached to the prepared tooth using cement. To ensure more reliable fixation, parapulp pins can be used - thin rods installed vertically in the space between the pulp chamber and the tooth wall.
The first signs of an allergy to crowns and ways to eliminate the problem.
Read here about the features of glass-ceramic crowns.
At this address https://www.vash-dentist.ru/protezirovanie/nesemnyie-p/koronki-np/metallokeramiki-shofu-halo.html you will find all the most important things about Shofu Halo metal ceramics.
Prosthetics with half crowns
A half-crown is a permanent metal prosthesis that covers the lingual, palatal (incisal edge), chewing surface and two contact surfaces. Unlike inlays, a half-crown is used only as a support for a bridge or splinting prosthesis. Due to the fact that it leaves the cheek and lip surfaces free, a good cosmetic effect is obtained. The basis for tooth preparation and the technique for making a half-crown is based on the same principles as for prosthetics with inlays.
Half-crowns are used on all front teeth and premolars. In the latter case, they are called three-quarter. Contraindications to their use are deep bite, low tooth crown and destruction of its contact surfaces.
The half-crown is strengthened in special grooves, the preparation of which is the most critical stage of tooth preparation. It is most convenient to describe the methods of half-crown prosthetics, keeping in mind a specific tooth, in particular the upper canine or incisor. Its preparation consists of the following stages.
First, the contact surfaces are separated. They are made parallel and slightly beveled towards the oral surface. Then, in order to prevent an increase in the height of the bite, the palatal surface of the tooth is ground down to the thickness of the metal (0.3-0.4 mm). When preparing the lower incisors, the lingual surface is ground very little or not at all. When the cutting edge and palatal surface are prepared, grooves are made on the contact surfaces with a fissure bur. They must be strictly parallel and located in the middle of the contact surfaces. On the palatal surface they are connected by a third (transverse) groove. The longitudinal grooves should extend onto the palatal surface at some distance from the cutting edge, otherwise, when a transverse groove is formed, it can be easily broken. The grooves created in this way take the form of the letter P (Fig. 73). In some cases, the edge of the crown near the gum may be adjacent to the tooth tissue, in others, a gingival ledge is created and the edge of the crown comes into butt contact with it.
If a half-crown is placed on a tooth that has no pulp, no grooves are made. Instead, a hole is drilled in the crown of the tooth on the palatal side that goes into the root canal, and the half-crown is strengthened with a pin.
Half-crowns for premolars are made very rarely and mainly for the upper ones, which are visible when smiling. The tooth preparation technique is somewhat different from that just described. After separation of the contact surfaces, the oral surface of the tooth is ground to the thickness of the metal (0.3-0.4 mm). At the same time, the palatal cusps are ground down to the same thickness. Grooves are formed on the contact and chewing surfaces. Only on the last one, the groove should not run along the fissure, but somewhat anterior to it, so that the tooth does not split.
A wax model for casting a half-crown can be obtained by direct and indirect methods. However, preference should be given to the latter, because the direct method in this case is very labor-intensive. The remaining procedures are no different from those used in the manufacture of the inlay.
Indications and contraindications
Half-crowns are a relative rarity in the arsenal of dentists. They are usually used in the following cases:
- As a supporting element for a bridge or clasp structure, if the goal is to preserve the front part of an intact tooth intact, and also to avoid unnecessary and unaesthetic exposure of a full metal crown.
- As a fastening element for splinting systems.
- As supporting devices when installing inlays in clinical situations when strong fastening of the latter is impossible without additional strengthening of the tooth. Half-crowns perform the function of such reinforcing structures.
Contraindications
The main obstacle to installing half-crowns are some design features and the insufficiently good condition of the supporting teeth:
- Caries.
- Small area or destruction of chewing surfaces.
- Severe defects of the approximal surfaces.
- Low tooth height, when it is difficult to ensure reliable fixation, and in addition, there is a risk of opening the pulpous chamber.
- There is a danger of weakening the buccal cusp during its preparation.
- The walls of the pulp chamber are too thin.
- Mobility of support units.
- Deep bite. Due to the need to grind down too thick a layer of enamel and dentin on the palatal side, there is a danger of opening the pulpous chamber.
It is not recommended to use half-crowns even with a long bridge.
Indications and clinical and laboratory stages of manufacturing a half-crown (three-quarter crown).
⇐ PreviousPage 2 of 3Next ⇒
Half-crowns are a permanent prosthesis covering the contact and palatal (lingual) surfaces of the tooth. The use of metal half-crowns for fixation of bridges has an aesthetic purpose. They leave the buccal and labial surfaces of the tooth free.
Half-crowns of this design, used on premolars, are called three-quarter crowns. They cover the contact, chewing and palatal (lingual) surfaces of the tooth. Half-crowns combined together are used as a splinting prosthesis for traumatic occlusion.
To use half-crowns, certain conditions are required, namely;
1) high clinical crowns with a well-defined dental cusp:
2) sufficient area of contact surfaces of supporting teeth;
3) resistance of teeth to caries.
Half-crowns made of ceramics that cover the defective vestibular surface of the front teeth are also called veneers.
The preparation of teeth for half-crowns begins with the separation of contact surfaces, which must be parallel. The palatal, or lingual surface, from the dental tubercle to the gingival margin should be vertical. Therefore, the equator of the tooth is removed in this zone using a cylindrical head. The occlusal surface is ground to the thickness of the metal (0.2-0.4 mm). The dental cusps should retain their shape. The cutting edge is ground beveled towards the oral side. Parallel grooves are created on the contact surfaces using a fissure bur. On canines, these grooves are connected on the palatal (lingual) surface by a transverse groove. If the dental tubercle is well defined, a channel 0.3 mm deep can be drilled on it to improve fixation of the half-crown.
After preparing the tooth, a double impression is taken, and the half-crown is cast on a fire-resistant model along with the frame of the bridge.
Clinic and preparation of the oral cavity for prosthetics with partial absence of teeth.
After tooth extraction, the dentition changes significantly. The clinical picture is very diverse and depends on the number of lost teeth, their location in the dentition, the function of these teeth, the type of occlusion, the condition of the periodontium and hard tissues of the remaining teeth, and the general condition of the patient.
Clinic. Patients present various complaints. In the absence of incisors and canines, complaints about aesthetic defects, speech impairment, splashing of saliva when speaking, and the inability to bite off food predominate. Patients who lack chewing teeth complain of impaired chewing (however, this complaint becomes dominant only in the absence of a significant number of teeth), more often of inconvenience when chewing, injury and soreness of the mucous membrane of the gingival margin. There are frequent complaints about aesthetic defects in the absence of premolars in the upper jaw. When collecting anamnestic data, it is necessary to establish the reason for tooth extraction, as well as find out whether orthopedic treatment was previously carried out and with the help of which denture designs.
On external examination, as a rule, there are no facial symptoms. If there are no incisors and canines on the upper jaw, then some retraction of the upper lip may be observed. In the absence of a significant number of teeth, retraction of the soft tissues of the cheeks and lips is often observed. In cases where part of the teeth on both jaws is missing without maintaining antagonists, that is, with an unfixed bite, the development of angular cheilitis (jamming) is possible; during the swallowing movement, a large amplitude of vertical movement of the lower jaw is observed.
When examining tissues and organs of the oral cavity, it is necessary to determine the type of defect and its extent, the presence of antagonizing pairs of teeth, the condition of hard tissues, mucous membrane and periodontal tissue, and evaluate the occlusal surface of dentures. In addition to the examination, palpation, probing are carried out, the stability of the teeth is determined, etc. An X-ray examination of the periodontium of the proposed supporting teeth is required.
The leading symptoms in the clinic for dental defects are:
1. Violation of the continuity of the dentition.
2. The disintegration of the dentition into independently functioning groups of teeth of two types - functioning and non-functioning.
3. Functional overload of the periodontium of the remaining teeth.
4. Deformations of the occlusal surface of the dentition.
5. Violation of chewing and speech functions.
6. Changes in the temporomandibular joint due to tooth loss.
7. Dysfunction of the masticatory muscles.
8. Violation of aesthetic standards.
Treatment plan:
ü complete sanitation of the oral cavity must be carried out (pay attention to teeth with increased sensitivity);
ü the feasibility of preserving teeth affected by caries and other diseases (x-ray and electroodontometric control), including filled ones, teeth with periodontal lesions, etc., should be checked when planning them as supporting ones;
ü pulpless teeth must have roots sealed to the apex (x-ray control);
ü the necessary treatment must be carried out for diseases of the periodontium and oral mucosa;
ü if pathological processes in the teeth and jaw bones are suspected, it is necessary to conduct an x-ray examination;
ü teeth and roots that cannot be preserved must be removed.
⇐ Previous2Next ⇒
Recommended pages:
Use the site search:
Pros and cons of products
The main advantage of half-crowns is the increased aesthetics of the abutment teeth covered with them due to the preservation of the integrity of the frontal surface.
The safety of the tooth and gums also increases compared to technology that uses a full crown.
Minuses:
- significant labor intensity of preparation of the supporting unit;
- high requirements for the doctor’s qualifications due to the complex configuration of the treatment area.
Manufacturing technology
The production of half-crowns involves a series of sequential clinical and laboratory procedures.
The choice of design is made based on diagnostics.
Preparation
A layer of enamel and dentin 0.6-1 mm thick is sanded off from the lingual, two lateral and chewing (cutting) surfaces.
The parallelism of the side surfaces must be checked. A slight inclination is allowed - convergence of 3-5° in the oral direction, so that the instructions can be easily put on and taken off when fitting.
It is advisable to provide an inclination in the chewing area. A U-shaped notch with a depth of no more than 1.5 mm is made on the occlusal and proximal surfaces.
The grooves on the side surfaces are made parallel to each other and shifted closer to the outer (vestibular) surface.
Grinding of the cutting edge of the tooth is carried out in such a way that the edge of the metal model is not visible from the front side.
Preparation methods may vary depending on the technique used - Vect or Elander. It is convenient to control the grinding depth by using a fissure bur of the appropriate size.
Techniques for tooth crown repair and how justified the procedure is.
In this article we will tell you why teeth hurt after crown removal.
Follow the link https://www.vash-dentist.ru/protezirovanie/nesemnyie-p/koronki-np/metallokeramicheskih-vita.html if you are interested in the characteristics of the Vita metal-ceramic crown.
Taking impressions
An impression is taken of the prepared tooth and the antagonist row. To obtain an impression, masses are used that give the most accurate impression.
The next stage is the production of plaster models from the impression and their processing.
Wax modeling
Before applying wax, the plaster tooth is coated (isolated) with varnish, oil or petroleum jelly. This is necessary to ensure that the wax cap can be easily removed.
Various modeling techniques are used. All of the wax can be applied by hand, or the capping technique is used, which involves first dipping a model of the tooth into molten wax to form a cap, which is then finished by hand.
First, wax is applied to the grooves. After application, it is pressed onto the model with your fingers until it hardens.
The thickness of the wax should be 0.3-0.4 mm. When modeling the chewing and cutting surfaces, the bite is controlled - manually or in an articulator. In this case, the dentition models must be installed in the position of central occlusion.
Casting
This is the most complex and responsible operation, which essentially consists of replacing wax with metal.
The flyer is installed in the zone of transition of the lingual surface to the chewing area - parallel to the longitudinal axis of the tooth.
A mold is made and fired, in which, instead of wax, a cavity is formed, filled with molten metal.
The last stage is fitting to the model with processing and removal of all irregularities and sagging.
Fitting in the mouth
The quality of the fit depends on the accuracy of the casting. Even the smallest burrs can disturb it, so they must be removed.
Before placing the half-crown on cement, it is necessary to remove the smallest gaps between it and the tooth.
Fixation of a half-crown
This is done using cement (cement phosphate). If the product is made of soft metal (silver-palladium alloy, gold).
Before the cement hardens, it is useful to roll (core) its edges for better fixation.
Notes
- The wall of the half-crown should enter the gingival pocket by 0.3 mm.
- When modeling, the wax should not extend onto the labial/buccal surface of the tooth, otherwise there will be problems with its removal and fixation of the finished crown.
- When casting a product, it is necessary to take into account metal shrinkage, which varies depending on the material.
The gold-platinum alloy shrinks slightly, while stainless steel shrinks significantly. When using it during modeling, it is recommended to cover the gypsum abutment tooth with tin foil, the thickness of which is 0.02-0.03 mm. To remove wrinkles, you can use the Parker apparatus. - When making a half-crown for pulpless teeth, a pin can be cast along with it and inserted into the root canal.
In the video, a specialist will talk about the features of restoring teeth with veneers, crowns and half-crowns.
Application of tabs in reconstructive surgery? dentistry
- An inlay is understood as a prosthesis designed to restore the anatomical shape and replace hard tissue defects
Indications for use of tabs
:
- Defects in dental crowns of various origins that cannot be replaced by filling
- Counter inlays on the side teeth prevent increased abrasion, being a means of its prevention
- With small included defects in the dentition, the inlays can play the role of supporting elements of the bridge.
- Splinting teeth for periodontitis using inlay (beam) splints
Contraindications to the use of tabs :
- Very deep and poorly accessible cavities submerged under the gum
- Defects in teeth with low and flattened crowns
Main advantages of tabs :
- The inlay manufacturing technique eliminates the possibility of incorrect cavity formation
- Pre-fitting makes it possible to create an inlay without overhanging edges, maintaining the sphericity of the proximal wall and correct interdental contact
- When making a metal inlay, creating a rebate along the edge of the cavity and covering it with the cast part of the inlay protects the border enamel prisms from breaking off and eliminates the possibility of secondary caries.
- Possibility of polishing all external surfaces, including proximal ones, before cementation
Classification of inlays by position in the tooth :
- Inlay - a box-shaped shape located inside the tooth that accurately follows its anatomical shape and occlusal surface
- Onlay - with fold outwards
- Overlay - one wall of the tooth is saved, the rest is from the tab
- Pinlay - an inlay with additional cavities or pin inclusions for fixation
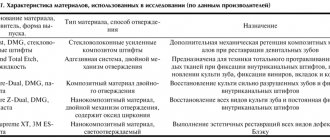
By material
:
- Metal (gold, cobalt-chrome alloy, silver-palladium alloy)
- Plastic
- Ceramic (IPS system = Empress, Cerec, E-max)
- Combined (metal + plastic, metal + ceramics)
- From zirconium oxide
By manufacturing method :
- Direct method
- Indirect method
General principles for forming cavities for inlays
- The cavity is given the most appropriate shape, such that the tab can be removed unhindered
- When forming a cavity to prevent recurrence of caries, expansion
- The bottom and walls of the cavity must be resistant to chewing pressure
- When forming a complex cavity that covers several surfaces, you should create points
- The cavity must have sufficient depth, sink into the dentin and not shift under chewing pressure
- The cavity should be asymmetrical or have additional recesses that serve as a guide when inserting the tab
- Prevention of chipping of thinned enamel edges is carried out by creating a bevel along the edge of the cavity or cast chewing surface
Indications for use of onlay tabs
:
- Carious cavities of class 1 according to Black
- Large defects of dental tissues in premolars and molars
- Restoration of bumps
- Preventive restoration of cusps
Clinical manufacturing steps
- Patient examination
- Anesthesia
- Preparing a cavity for an inlay
- Coating the inner surface with insulating varnish
- Taking a two-layer impression
- Closing the cavity with a temporary bandage
- Fitting the tab in the oral cavity
- Etching the enamel edge of the cavity during 45 sec.
- Fixing the inlay in the tooth cavity using Dual-cement
- Final polishing of the edge of the inlay
Technical stages of production
- Making two working models from supergypsum and regular gypsum and auxiliary models
- Treatment of a working model made of ordinary plaster with a separating liquid
- Modeling a composite inlay
- Polymerization of the inlay on the plaster model in the apparatus
- Polishing the outer surface of the inlay and sandblasting its inner surface
- Processing the inlay on a working model made of super plaster with control of occlusal contacts in the articulator
Application of ceramic inlays
:
- Cerec system
- Empress ceramics
- Fiberglass ceramics
Classification of dental ceramics
:
- Conventional slip ceramics (increased content of crystalline phase)
- Casting ceramics (mica-based glass ceramics)
- Ceramics obtained by mechanical processing using a computer program (ceramics, zirconium oxide CAD/CAM)
- Pressable ceramics (feldspathic ceramics reinforced with leucite)
- Glass-saturated ceramics
Long-term results of orthopedic treatment with ceramic inlays
Efficiency over a 6-year service life:
- Conventional slip ceramics - 92%
- Casting ceramics - 90%
- Ceramics obtained by mechanical processing using a computer program (CAD/CAM) - 91-100%
- Pressed ceramics - 94%
Stages of making ceramic inlays
Clinical stages .
1st stage:
- Determination of shade using shades before tooth preparation
- Anesthesia and cavity preparation for an inlay
- Applying a pulp isolation pad
- Obtaining a two-layer print
2nd stage:
- Fitting in the oral cavity, preparing the cavity for fixation
- Preparing the tab for fixation, fixing the tab
- Final processing, finishing, polishing of the inlay
Technical stages of production
1st stage:
- Production of two models: a working collapsible one made of supergypsum and an auxiliary one made of solid gypsum
- Plastering models into the articulator
- Modeling a hard wax inlay on a working model in an articulator
2nd stage:
- Composing the sprue tree and molding it with fire-resistant investment material
- Ceramics injection molding stage
- Freeing the sprue tree from investment material and removing the sprues
3rd stage:
- Fitting the inlay to the model in the articulator
- Applying an enamel layer and transparency to the outer surfaces of the tab
- Application of dyes and glazing
Natural color concept . Systematization of visual selection .
Visual color detection system:
- Color space is selected according to a natural pattern
- The arrangement of color samples corresponds to the logical construction of the dental color space and is clearly divided into areas: yellow, orange and red
- The effect of metametry between color samples and facing material is excluded, because color samples are made of identical ceramics
- The effect of contrast enhancement is eliminated by using a gingival mask
The perception of color is influenced by :
- Lighting
- Gum color
- Surrounding tissue
- Type and structure of the color indicator
- Test sample placement
- Individual human ability to see color
- Experience in color determination
- How the eye works
Service life and cost
The service life of a half-crown used as an element for fastening a bridge depends on the following indicators:
- service life of the problematic element;
- the material from which the model is made;
- condition of supporting teeth;
- operating conditions of the prosthesis.
In general, with good quality supporting units and proper operation, the service life of a bridge can be from 5 to 15 years.
The price of a half-crown depends mainly on the material from which it is made. The cheapest option - a steel structure will cost from 1000 rubles.
A design made of chromium-cobalt alloy will cost at least 3000-4000 rubles.
Ceramic veneering for the front part of a tooth can cost from 28,000 rubles.
Reviews
Typically, bridges are secured using full crowns. Making them and preparing a tooth for them is a routine operation for dentists and technicians.
Not every doctor would think of suggesting that a patient have a half-crown installed.
If you have such a relative rarity installed in your mouth, please share your impressions and experience of using it. You can do this by leaving a review at the bottom of this page.
If you find an error, please select a piece of text and press Ctrl+Enter.
Tags dental crowns fixed dentures
Did you like the article? stay tuned
Previous article
Sky implants – high-tech systems for patients of all age groups
Next article
Three reasons to stop wearing fake braces