- Characteristics of osteoplastic material in dentistry
- Classification of osteoplastic materials
- Necessary procedures before bone augmentation
- Type of osteoplasty
- Surgery with osteoplastic material at A-Medic
The use of bone material in dentistry is widespread. With its help, it is possible to perform osteoplasty - to restore the lost volume of the alveolar ridge. This allows you to avoid further destruction of bone tissue and the appearance of a number of negative consequences that arise against the background of changes in appearance and deterioration of human health. The procedure is often used before installing implants when the patient’s bone tissue is insufficient. Let's take a closer look at the specifics of the materials that make it possible to carry out these events.
Characteristics of osteoplastic material in dentistry
Osteoplastic materials in surgical dentistry must be of high quality and have the following characteristics:
- safety for human health (the use of artificial bone tissue that can harm the body is prohibited);
- high efficiency;
- porosity (ensures the germination of new bone tissue);
- full compatibility with the tissues into which the materials will be implanted;
- ridding the bone tissue of the defect by filling it.
Currently, there are many types of osteoplastic materials on the market. When choosing the most suitable material, all the above characteristics must be taken into account. In addition, it must be ready for immediate use and have high adhesion rates so that the implant can adhere to the bone as closely as possible.
Varieties by purpose
Osteoneutral implants
Osteoneutral implants are mainly used to fill holes. They are a foreign body, which serves as a kind of support for recovery. These implants are:
- absorbable;
- non-absorbable;
- metal.
Osteoconductive
Osteoconductive bone replacement materials are a framework for bone. Divided into:
- alloplastic, which also include: hydroxyapatite, porous and not;
- biological glass;
- calcium.
Osteoinductive
Osteoinductive materials renew the growth of ligaments. Are divided into:
- demineralized and lyophilized alloimplants;
- autografts located: in the mouth (chin, upper jaw, bone mixture);
- outside the mouth (femur, ilium).
Classification of osteoplastic materials
Osteoplastic materials are implants that promote bone formation. At the same time, they provide local osteoconductive, osteoinductive or osteogenic activity. According to their origin, all osteoplastic materials are divided into four main groups:
- autogenous (the patient is the donor);
- allogeneic (the donor is another person);
- xenogeneic (the donor is an animal);
- synthetic (made from calcium salts).
Let's take a closer look at the features of each group separately.
Autogenous
Autogenous bone replacement material is used more often than others in dentistry. Autologous bone is obtained by harvesting from a donor intraoral or extraoral site and then transplanting it into a receiving site. In a number of clinical studies, it has been proven that it promotes accelerated replacement of postoperative and other bone defects with newly formed tissue. It is characterized by plasticity and does not have the properties of immune incompatibility. At the same time, the financial costs associated with its fence are small.
According to their origin, two types are distinguished - endochondral (cartilaginous) and ectomesenchymal (membrane) origin. Disadvantages include the likelihood of infection, the traumatic nature of obtaining autologous material, and the long duration of the surgical intervention itself. Often, autologous bone is used in combination with other materials, for example, allobone or xenobone. This avoids shrinkage of the autologous bone.
Allogeneic
In accordance with the legislation, allogeneic bone material is not used for sinus lifting in the Russian Federation. Allogeneic implants are osteoplastic materials that are obtained from human corpses and subsequently subjected to special processing. This may be cortical and cancellous ilium or a demineralized lyophilized bone allograft. The main advantages of this group in comparison with automaterials include:
- pronounced osteoinductive potential;
- no trauma when obtaining the material;
- good adhesion to the recipient bed;
- short duration of surgical intervention;
- good micro- and macroporous structure (guarantees rapid angiogenesis).
In addition to ethical problems, the disadvantages of using these materials include the likelihood of possible infection of recipients with HIV infection and hepatitis.
Xenogeneic
In extremely rare cases, specialists resort to the use of xenogeneic bone material for implantation. It has osteoconductive properties and preserves the original mineral structure of the bone. Xenobone (natural hydroxyapatite) is obtained from mammalian bone tissue. The structure of animal bones is identical to human bones, which allows them to be used in dental practice. Xenobone is preliminarily subjected to special treatment and deantigenization. This allows you to eliminate from its composition all factors that provoke the development of an immunological and allergic reaction.
Depending on the type of processing, a distinction is made between xenomaterials with low-temperature processing, xenomaterials with high-temperature processing and xenomaterials based on enzyme technologies. There are two main methods of deantigenization. The most effective and popular is heat treatment at elevated temperatures (about 700-1000 C°), after which all organic substances evaporate. Xenobone does not shrink. Due to the synchronicity of the processes of bone destruction and restoration, physiological replacement of artificial bone granules with natural bone occurs, without loss of volume.
Synthetic
Synthetic bone material is made on the basis of calcium salts. In particularly complex clinical cases, when it is necessary to build up large volumes of bone in the horizontal or vertical direction, xenogeneic bone tissue is combined with autogenous bone in equal proportions. Synthetics are a worthy alternative to auto-, allo- and xenomaterials. In some respects, they are superior to osteoplastic materials of natural origin (for example, there is no need to harvest bone tissue, and the possibility of infection with infectious pathologies is excluded).
The main disadvantage of most synthetic materials in comparison with auto-, allo- and xenomaterials is the lack of osteoinductive properties (the ability to cause ectopic bone tissue formation). If components are added to their composition that will stimulate bone tissue regeneration (for example, collagen), they can acquire osteoinductive properties.
Algorithm for performing osteoplasty
Bone grafting consists of several stages, including preparation, surgery, rehabilitation, and osteosynthesis. Osteoplasty algorithm:
- preparation begins with a comprehensive examination of the patient. During this stage, the doctor collects anamnesis, identifies indications and contraindications, and visual and hardware diagnostics. All this allows the surgeon to make a diagnosis, determine the degree of atrophy and the characteristics of the clinical case. Based on the conclusions made, the doctor plans the type and course of surgical treatment;
- Sanitation of the oral cavity is a prerequisite for the operation. This complex includes dental and periodontal treatment (if necessary), professional dental cleaning;
- surgical stage – performed according to a developed protocol depending on the type of plastic surgery. General scheme: local anesthesia, gum incision to gain access to the operated area, preparation of a bed for laying the graft, fixation of bone material and growth stimulator, suturing of the surgical wound;
- the process of osteosynthesis (formation of new bone tissue). Lasts up to 6 months. The duration depends on the type of plastic surgery and the transplant materials used.
General recommendations for the rehabilitation period:
- do not eat or drink for 3 hours after surgery;
- do not brush the surgical area with a toothbrush for at least 10 days;
- food should not be hot or cold, it should be finely chopped during the entire time until the surgical suture heals;
- Do not drink through a straw or blow your nose (especially after a sinus lift);
- you should refrain from physical activity (including fitness) for at least 2 weeks after surgery;
- be sure to take medications prescribed by the doctor;
- it is necessary to monitor your well-being and the site of surgery. If inflammation, swelling, or temperature occur, immediately consult your doctor.
Expert advice: 2 hours before surgery you should refrain from eating. After surgery, it is necessary to meticulously adhere to the surgeon’s recommendations on nutrition, hygiene, and physical activity. stress, as well as taking prescribed antibiotics and other medications. Otherwise, postoperative complications are possible.
The dental network offers osteoplasty services. Our surgeons are highly qualified and improve their skills in famous clinics in Russia and Europe. The quality of surgical operations meets international standards. We have a system of family and cumulative discounts. We provide the necessary documents for filing a tax deduction. Convenient appointment schedule with specialists: daily without a break from 9 to 21 hours (Sunday from 10 to 16).
Branches of our orthodontic center are located in Moscow within walking distance from the metro:
- Art. Alekseevskaya (VDNKh district, etc. Mira), address: st. 3rd Mytishchiskaya house 3, building 2;
- Art. Shelepikha, address: Shelepikhinskaya embankment, address: building 34, building 1.
You can trust us with your health, come, we will solve any dental problem. Waiting for you!
Necessary procedures before bone augmentation
Once a molar or premolar is removed, the bone is no longer subject to regular stress, which over time causes it to atrophy and lose volume. Along with this, inflammatory processes appear in periodontal tissue. As a result, the more days that pass after the loss of a molar or premolar, the more the bone begins to become deficient. Against this background, it becomes much more difficult to carry out implantation.
The technique used to increase bone tissue volume is selected individually in each clinical case. To do this, the dentist first evaluates the oral cavity and, if necessary, prescribes instrumental diagnostics. It often happens that the need to use another technique arises only during the period of surgical intervention. Due to this, the specialist must be aware of all types of osteoplasty and be able to apply them in practice.
Scope of application of bone chips in dentistry
The roots of the teeth are located in the jaw tissue, and when chewing food, it naturally receives the load it needs. Without it, the normal functioning of the bone is impossible, its cells are destroyed, it atrophies. There is not enough tissue to properly install the implant. Atrophy is a serious problem, especially if several teeth are lost. Difficulties with chewing food appear, the aesthetics of the smile and facial skin suffer greatly (wrinkles deepen), and more serious, medical problems may arise. In most cases, the problem of restoration must be solved surgically. Doctors perform a bone grafting operation and build up the “base” for the implant.
One of the materials used during the intervention is bone chips. This is a graft crushed to granules of 0.5-1 mm, which is taken in the form of a block from the patient himself or the animal (cattle). The starting material is accordingly called an autograft or xenograft. The first option is recognized as the “gold standard” in dental practice. The risk of rejection and complications with it is minimal, but to obtain it, it is necessary to carry out additional intervention - sampling of material. However, the MAZOT Dental Center uses a technique for obtaining bone chips from the patient’s teeth to be removed. In this way, surgical interventions can be avoided.
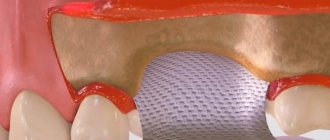
Artificial grafts, alloplasts, are also used in implantology. These are mainly bioceramic and hydroxyapatite materials, as well as membranes that need to be used to cover the bone “replantation” site. Despite its scale and complexity, bone grafting is considered one of the most effective and safe methods of tissue restoration, and in many cases it cannot be avoided.
Type of osteoplasty
Below are the main types of osteoplasty to understand for which surgical interventions a specific type of material is used:
- autotransplantation. This is a procedure that involves moving a tooth from one place to another in order to fill a visually and functionally significant defect. Eighth molars (wisdom teeth) are most often transplanted. As a result of the operation, the bone tissue becomes significantly wider;
- sinus lift. This is a surgical intervention that is performed on the upper jaw in order to increase the length of bone tissue in case of its deficiency.
It is possible to increase the volume of bone tissue through the use of materials of synthetic origin. Barrier membranes are used to fix transplanted bone tissue or to protect a person’s bone tissue after a molar or premolar has been removed. Allografts are used to restore bone tissue. The most common are autografts.
Osteoplasty methods
Adequate width and height of bone tissue is necessary for the implant to be stabilized. Once a tooth is lost, there is no necessary physiological pressure on the bone. Atrophic processes begin. The smaller the volume of the alveolar process, the more difficult it is to carry out successful implantation, since when installing an intraosseous implant there is a risk of perforating the bottom of the maxillary sinus.
Bone grafting allows you to increase the required bone volume and successfully implant an implant. In practice, the following bone grafting methods are most often used:
- Splitting of the alveolar process. The ridge of the process is split with a milling cutter and implants are installed. The space around them is filled with bone replacement material. After osseointegration, abutments are installed and prosthetics are made. With this method, synthetic osteoplastic materials are often used;
- Autogenous bone block grafting. Bone collection is done in the chin area or from the alveolar tuberosities of the “figure eights”. After this, the bone block is implanted into the defective area. The method is suitable for significant bone atrophy. Implantation is done after complete engraftment of the graft;
- Guided bone regeneration. Carry out simultaneously with implantation. For replanting, allogeneic or xenogeneic material is used. The method is suitable for slight loss of natural bone;
- Sinus lift. Subantral augmentation is used to increase the volume of bone tissue in the upper jaw in the area of the maxillary sinuses. Performed using open or closed methods. The choice is influenced by the height of the alveolar process and the type of implants. An open sinus lift is indicated for significant bone loss; a closed sinus lift can be used when the height of the alveolar process is 4-6 mm. In most cases, it is possible to perform bone grafting simultaneously with implantation, but if the bone height is less than 2 mm, sinus lift is performed as an independent operation. The implant is installed only after complete engraftment of the graft. Autogenous osteoplastic material is well suited for sinus lifting. In some cases, it is advisable to use a combination of different grafts.
The surgeon selects the appropriate osteoplasty method based on the clinical picture and study results. He also individually selects the osteoplastic material with which he will work.
Surgery with osteoplastic material at A-Medic
Osteoplastic operations are recognized as one of the most difficult (from a technical point of view) in the field of dental surgery. To avoid a number of negative consequences after surgery, they should be performed only in trusted clinics. Highly qualified dental specialists at A-Medic have been specializing in these operations for many years. The clinic is equipped with modern instruments, modernized equipment and the necessary lighting, which guarantees a positive result of therapy.
Doctors perform high-quality surgical interventions of any complexity using various osteoplastic materials. The cost of the procedure is significantly lower than in other private clinics in Moscow. You can find out more about the price list on the official website. To make an initial appointment with a dentist, just call the clinic at the numbers provided or leave a request online (indicating your name and contact number).
What is bone grafting during dental implantation?
Dental implantation is an operation to insert an implant into the bone tissue of the patient’s jaw.
The success of this surgical intervention depends entirely on the reliability of the osseointegration of the artificial root. The main condition for obtaining a positive result is sufficient bone density and volume. But, for various reasons, quite often patients exhibit a deficiency of these parameters. Modern dentistry has effective methods for eliminating this defect. This is bone grafting, the purpose of which is to compensate for bone deficiency. Causes of loss (resorption) of jaw bone tissue:
- tooth loss;
- injury;
- dental and periodontal diseases.
Bone grafting during implantation (osteoplasty, augmentation) is a surgical operation to replant osteoplastic materials in the area where the implant is installed when bone deficiency is detected there. Such manipulations have been carried out since 1965, so they have been quite well studied and have received recognition from implantologists around the world. Osteoplasty is an extremely popular procedure for implantation. This is due to the fact that atrophy of the bone structure occurs rapidly. For example, after tooth extraction, the width of the alveolar process in this area decreases to 40% per year. Carrying out augmentation requires great skill and precision from the surgeon.
Please note: the network of “Smile” clinics employs highly qualified surgeons, and the branches are equipped with modern diagnostic and dental equipment. Our specialists successfully perform operations of any complexity.
Contraindications
- HIV AIDS
- Oncology
- Diabetes
- Severe pathologies of the heart and blood vessels
- Poor blood clotting
- Osteomyelitis
- Epilepsy
- Allergy to anesthetics
- Diseases of the ENT organs
- Alcoholism and drug addiction
- Pregnancy
- Dental and periodontal diseases
- Infectious diseases
Bone grafts. Part 3
Synthetic bone substitutes - alloplastic materials
There are four main types of synthetic materials available on the market: non-porous hydroxyapatite, porous hydroxyapatite, beta-tricalcium phosphate and HTP polymer (polymer of polymethyl acrylate and hydroxyethyl methacrylate coated with calcium). Porous and nonporous hydroxyapatite and HTP polymer materials have been reported to be nonabsorbable, while tricalcium phosphate is resorbable. Results from controlled clinical studies have shown significant improvement with the use of nonporous and porous grafting materials compared to defects where no bone grafting materials were used. Defect closure ranged from 1.6-3.5 mm when using a synthetic bone substitute to 0.5-0.7 mm in areas where no graft was used. In addition, treatment with osteoplastic materials for class II furcation defects in the mandible was significantly more effective than treatment in a control group of patients treated with or without guided tissue regeneration techniques but without bone substitutes. A five-year follow-up after the use of porous and non-porous hydroxyapatite for the treatment of intraosseous defects showed clinical stabilization. In addition, studies have proven the effectiveness of defect closure using tricalcium phosphate. Significant improvement was also achieved with the use of NTP polymer compared to the control group. Although clinical signs appear promising, histological evidence suggests that the material is encapsulated by connective tissue and is associated with little bone regeneration. Some histological studies have demonstrated limited new bone formation in the immediate vicinity of or on the surface of alloplastic material, as well as within particles. One histological study report suggested that some regeneration could be achieved using porous hydroxyapatite. There is also histological evidence of the possibility of very little regeneration after the use of NTP polymer. Be that as it may, it is currently believed that the function of alloplastic materials is to create an indifferent filler. When compared, bone allografts and hydroxyapatite clinically produce similar results. However, if the goal of the operation is to achieve regeneration, then guided tissue regeneration or bone grafting is preferable.
Conclusion
The use of alloplastic materials as filler can achieve significant clinical improvement. However, from a histological point of view, they act as biological fillers and cause little or no bone regeneration and result in very limited periodontal regeneration.
Areas of additional interest
Root Surface Demineralization/Citric Acid
Demineralization of the root surface, usually with citric acid, is often used as an adjunct to guided tissue regeneration. This technique is used to change the root surface by “detoxifying” it and releasing collagen fibers in the cementum or dentin structure. Animal studies have proven the emergence of new connective tissue attachment after demineralization of the root surface with a solution of citric acid, although the desired result was not always achieved. When citric acid was used to demineralize the root surface, clinical studies provided histological evidence of new connective tissue attachment and some regeneration. Again, the results were not consistent enough. Clinical studies have shown no benefit from the use of citric acid in addition to surgical procedures, regardless of the use of bone materials or guided tissue regeneration. Promising results have been obtained when experimentally combining root surface demineralization with fibronectin to produce a more pronounced response. However, when used in humans, this technique did not lead to significant improvement. In conclusion, it should be noted that demineralization of the root surface does not lead to significant improvement in results when compared with a control group of patients who did not receive this type of therapy. Histological data prove the emergence of new connective tissue attachment and some regeneration as a result of demineralization of the root surface. However, histological improvement did not lead to significant improvement in clinical status compared with the control group.
Matrix proteins/growth factors
Research into matrix proteins and/or growth factors for regeneration efficacy is in the early stages. The first clinical trials were conducted in 1991. This interesting and promising technique is discussed in other review papers of the American Academy of Periodontology.
Conclusion
Autogenous and allogeneic bone grafts result in bone replacement, which has been proven in many studies involving large numbers of patients. Controlled clinical studies have shown more modest results. There is a large amount of clinical and histological evidence of periodontal and bone regeneration, which allows us to recommend their use in the practice of a dentist. Guided tissue regeneration is particularly effective in achieving regeneration in intraosseous defects with three bone walls. These techniques have been preferred, although less effective, in the treatment of class II furcation defects, especially those involving the mandible. The available clinical and histological data regarding bone and periodontal regeneration are sufficient to recommend this technique for use in clinical practice. The use of flap manipulation to provide wound stability during the early healing period results in bone regeneration in class II mandibular furcation defects and limited clinical improvement in mandibular class III furcation defects. No clinical studies have been reported on the use of this technique for the treatment of other defects. Alloplastic materials (synthetic bone substitutes) play the role of biocompatible fillers of the defect. The use of these materials leads to results similar to those of bone grafts or guided tissue regeneration. However, with the use of synthetic bone substitutes, little or even no periodontal regeneration occurs.
Beginning of article: Part 1 Part 2