Performing syndrome diagnosis
To properly check for the presence of a disease, it is necessary to perform a full range of various procedures. In particular, diagnosis of stylohyoid syndrome includes a number of actions and manipulations.
First of all, a professional examination of the patient is performed, as a result of which the doctor examines and identifies the compaction of the bone growth in the area of the anterior zone of the cervical spine of the patient. If you press on this part, the person should experience pain, and his health will deteriorate greatly.
Secondly, an X-ray of the facial skeleton, skull bones, and neck is taken.
At the time of diagnosis, you should carefully approach the procedures, because this disease can easily be confused with other similar pathologies, the symptoms of which are very similar. As an example, suppuration of the tonsils can be cited.
Acute purulent arthritis
The disease is caused by streptococci, staphylococci, pneumococci and other pathogens that spread to the elements of the joint through contact (with osteomyelitis of the lower jaw branch, mumps, phlegmon of the parotid-masticatory area, acute purulent otitis media, etc.), directly through wounds, trauma, lymphogenous or hematogenously from neighboring purulent foci, for example, with sore throat and other diseases. Serous, purulent or purulent-hemorrhagic exudate appears in the joint cavity. The nature of the exudate is determined by the pathogen and the stage of development of the process. In acute purulent arthritis, melting of the cartilaginous cover of the head, articular tubercle, purulent infiltration of the joint capsule and the appearance of necrotic foci in the synovial membrane may occur. In advanced cases, signs of destruction of the cortical layer of the bone elements of the joint are noted, that is, osteoarthritis of the temporomandibular joint develops. There are nonspecific arthritis caused by pyogenic microflora and specific arthritis of the temporomandibular joint, which can develop after any general infectious disease (syphilis, gonorrhea, typhoid fever, measles, dysentery, scarlet fever, etc.). According to the observations of many authors, acute purulent arthritis is rare diseases of the temporomandibular joint.
The clinical picture is determined by the stage of the process, the virulence of the infection, as well as the severity of the primary disease (otitis, phlegmon, mumps, osteomyelitis, etc.), a complication of which is acute purulent arthritis of the temporomandibular joint. As in other joints, when the capsule is damaged, swelling of the soft tissues and pain in the joint area are noted, which intensifies with any movements of the lower jaw. This leads to limited mobility of the lower jaw. When palpating the joint from the side of the external auditory canal or from the outside, sharp pain is noted. General phenomena (fever, changes in blood patterns, etc.) are often mild or absent.
With SBD there are no signs of inflammation and pain on palpation in the area of the temporomandibular joint. SBD is characterized by pain not in the joint, but in the area of the muscles that lift the mandible, and most often the external pterygoid muscle (behind the tuber maxillae).
Traumatic arthritis occurs when there is a blow or other injury in which the force applied is insufficient to cause a fracture of the articular process or its head. In these cases, soft tissue bruises usually occur in the joint area. To determine the nature of the injury, it is necessary to carefully collect anamnesis and conduct a thorough clinical and radiological examination of the patient.
When soft tissue is contused in the area of the temporomandibular joint, pain, limited mobility of the lower jaw, and sometimes swelling, hematoma, and abrasions are noted. Radiographs show no changes in the lower jaw or bone elements of the joint. A history of injury or bruise will help establish the correct diagnosis.
Clinic
In the presence of an elongated and/or curved styloid process, or a calcified stylohyoid ligament, or a calcified stylohyoid fold, or elongated horns of the hyoid bone, excessive pressure of these structures occurs on the internal and external carotid arteries. Due to this, in the areas fed by the carotid arteries, many seemingly unrelated clinical symptoms appear, such as:
- sensation of a foreign body in the throat;
- chronic inflammation of the pharyngeal mucosa;
- pain in the maxillary joint;
- pain and noise in the ears;
- unilateral and bilateral orbital or headache;
- “shooting” pain when turning the head.
According to the literature, patients with stylohyoid syndrome most often complain of poorly localized pain with unilateral localization in the upper anterior part of the neck and irradiation to the pharynx, root of the tongue, and ear. In this case, pain can spread to the temporomandibular joint, lower jaw, temporal, buccal areas, and submandibular triangle. In some patients, pain occurs in the teeth of the upper and lower jaws. M. Kiely et al. (1995) described the spread of pain to the sternocleidomastoid muscle, and D. Savic (1987) - to the supraclavicular fossa, shoulder girdle and anterior chest wall. Patients usually characterize the pain as dull, constant with periods of intensification and weakening. Its intensity increases towards the end of the day, intensifying when turning or throwing back the head, after a long conversation or singing, or changes in weather conditions.
Patients usually complain of pain in only one organ, most often in the pharynx, ear, temporomandibular joint, and only a detailed survey allows us to clarify its localization and areas of distribution. Some patients develop glossopharyngeal neuralgia with its characteristic painful paroxysms. Dysphagia is a common symptom of the disease, and difficulty swallowing is usually associated with a significant increase in pain in the throat and ear. Some patients are bothered by the sensation of a foreign body in the throat, others are worried about a “constantly sore throat”; they may experience pharyngeal spasm, persistent dry cough without objective signs of inflammation in the upper respiratory tract.
Stylopharyngeal syndrome
As a rule, it is right-sided, since the right styloid process is normally longer than the left by an average of 0.5 cm. Pain occurs as a result of pressure, for example, by an elongated and inwardly curved styloid process, on the tissue in the area of the tonsillar fossa and irritation of the nerve endings of the glossopharyngeal nerve. The intensity of pain varies greatly - from minor pain or the sensation of a foreign body in the throat, especially when swallowing, to sharp, severe constant pain in the throat and tonsils, radiating to the ear. Some patients also note pain on the front surface of the neck, in the area of the hyoid bone. Occasionally, these sore throats are mistakenly associated with pathological changes in the tonsil and it is removed, and ongoing pain is explained by irritation of the nerve endings by a postoperative scar. However, stylopharyngeal syndrome should be differentiated not only from damage to the tonsils, for example by a chronic inflammatory process, but also from neuralgia of the glossopharyngeal nerve. Neuralgia of the latter is characterized by paroxysmal burning or shooting pains in the pharynx, tonsils, root of the tongue, radiating to the ear, which occur during talking, laughing, coughing, yawning and eating.
Styloid-carotid syndrome (“carotid artery syndrome”).
The pathogenesis consists of pressure from the tip of the elongated and outwardly deviated styloid process on the internal or external carotid artery near the bifurcation of the common carotid artery, irritation of the periarterial sympathetic plexus and pain receptors. When the internal carotid artery is irritated, the pain is constant and is felt in the frontal region, orbit, eyes, that is, in the area of branching and blood supply of the internal carotid artery or its branches, in particular the orbital artery. Due to the pressure of the appendage on the external carotid artery, pain radiates along its branches to the temple, crown, face (below the eye).
- Why does the jaw hurt on one side when chewing near the ear: what does pain on the right and left mean, how to treat it?
Stylohyoid syndrome: symptoms, ICD, treatment
Stylohyoid syndrome - syndrome of elongated styloid process, Eagle's syndrome is characterized by a variety of symptoms: pain in the lateral wall of the pharynx and maxillary region, radiating to the ear, temporal, submandibular region or lower jaw. The syndrome was first described by Watt Eagle in 1937. There is also evidence that ossification of the stylohyoid ligament was described in the early 17th century by the Italian anatomist Pietro Marchetti.
According to the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS), ICD-10 stylohyoid syndrome (ICD-10) is classified by the following codes:
- G50.1 (atypical pain in the face)
- R07.0 (sore throat)
- M54.2 (cervicoalgia)
- R13.19 (other dysphagia)
- M62.89 (other specified muscle diseases), in the USA the code M62.8
Another potential code is M89.8 (other specified bone lesions). In the United States, the procedure for shortening the styloid process is coded 21499 CPT (Other musculoskeletal procedures of the head, and CPT stands for Current Procedural Terminology - a modern medical terminology for procedures, a reference used for payment of medical services in the United States).
Symptoms are usually characterized by a feeling of pharyngeal constriction, the presence of a “foreign body” in the area of the root of the tongue or pharynx, soreness, dizziness, a sharp decrease in performance and other signs of discomfort. The authors associate the appearance of such symptoms with the mechanical effect of the tip of the displaced styloid process on the tissues and organs, vascular and nervous formations of the neck.
In this case, two variants of stylohyoid syndrome are distinguished: the stylohyoid syndrome itself and the syndrome of compression of the carotid artery by the elongated styloid process. Some authors associate the mechanism of injury to organs and tissues of the neck with the apex of the elongated and mixed styloid process, while other authors observed multiple fractures and pseudarthrosis on radiographs and macroscopic specimens of removed styloid processes. There are indications of a significant role in the development of stylohyoid syndrome: sclerosis of the stylohyoid ligament.
Pointing to the variety of clinical symptoms, the authors provide clinical observations of patients with stylohyoid syndrome with elongated styloid processes, with a joint-like connection with the lesser horn of the hyoid bone, with tuberous spherical growths of bone tissue at the sites of fracture of the styloid process, with sclerotic stylohyoid ligaments, and note the fusion of the styloid process with small horns of the hyoid bone. At the same time, according to the majority. authors, other mechanisms of disease development are possible. One of them may be painful dysfunction of the muscles attached to the styloid process. The cause of its occurrence can be various types of injuries, including those associated with excessive opening of the mouth and overload of the masticatory muscles.
X-rays and computed tomography (CT) help to establish the diagnosis, in the images of which one can often be surprised by the curvature or elongation of the styloid processes of the temporal bones of the skull, as well as, less commonly, ossification of the stylohyoid ligament. The diagnosis of stylohyoid syndrome can also be confirmed by performing a blockade with a local anesthetic. Reduction of pain after injection confirms the syndrome and also allows us to exclude other causes of pain in this area, such as glossopharyngeal neuralgia or a tumor in the retropharyngeal space.
The authors did not note a direct relationship between the size and shape of the process and the likelihood of this syndrome occurring. There is always a need for differential diagnosis with other diseases when pain radiates to the ear, submandibular region, or lower jaw teeth. As a rule, patients unsuccessfully turn to various specialists and take various procedures that do not lead to a pronounced positive effect and are always short-lived.
Sufferers of stylohyoid syndrome often complain of pain in the throat: pulling, cutting, constant, intensifying periodically, radiating to the ear, temporal, premaxillary or submandibular region, root of the tongue, teeth of the lower jaw, pain in the root of the tongue. With localized pain in the lateral wall of the pharynx, patients indicate the site of pain as the palatine tonsil, most often the right one. Patients distinguish discomfort from constant pain. In addition, patients complain of headaches, dizziness, decreased performance, deterioration during physical activity, bad mood, reluctance to engage in physical activity, and sleep disturbances. The feeling of a foreign body in the throat, in some patients it intensifies when swallowing, there may be coughing and vomiting. When patients complained of pain or discomfort in the maxillary region, pain in the direction of the styloid process was expressed by palpation to varying degrees, from aching to acute. During intraoral palpation of the lateral wall of the pharynx, the pain point was more often detected behind the anterior palatine arch in the projection of the upper pole of the palatine tonsil, less often in the upper part of the pterygomandibular fold or in the projection of the palatine tonsil. Only one observation revealed pain in the lateral wall of the pharynx behind the posterior palatine arch. As a rule, the pain was more intense on the right.
All patients often have a history of observation and treatment by an ENT doctor using antibiotics without significant improvement; in addition, some patients had consultations with therapists, neurologists, and neurosurgeons.
There is also a psychological connection and after radical treatment it does not always become easier. In such cases, it is necessary to carry out psychotherapy to reduce the level of stress and anxiety, prescribe sedatives in the postoperative period, gradually the complaints of anxious patients disappear.
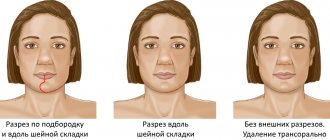
Professor Levents A.A. A surgical treatment technique has been developed: through an incision in the maxillary region along the upper cervical fold, about 50 mm long. The upper end of the incision is located at a distance of about 10 mm from the top of the earlobe. After retracting the lower pole of the parotid salivary gland, the peripharyngeal space is separated, the styloid process is isolated, freed from the surrounding tissues (attached muscles, ligaments, scars) and its resection is performed.
PS In the Krasnoyarsk region, since 2011, more than 50 patients with stylohyoid syndrome have been surgically treated. The condition of patients in the postoperative period is being studied. The duration of observation of patients after surgery is from 4 months to 5 years.
Based on materials from the authors: Anatoly Aleksandrovich Levenets – Doctor of Medical Sciences, Prof. head department surgical dentistry and maxillofacial surgery of Krasnoyarsk State Medical University; e-mail: [email protected] Simonov Andrey Gerbertovich - head. Department of Maxillofacial Surgery, Regional Clinical Hospital; tel. 8(391)2201517, tel.: 8(391)2201547.
Diagnostics
To make a diagnosis, it is very important to carefully collect complaints and medical history. So, it is necessary to establish when the painful sensations appeared, what nature they are, what provokes an increase in pain, and what causes a weakening. It is necessary to accurately determine the areas where pain occurs and where it radiates. This is important for differential diagnosis with neuralgia of other nerves (occipital, glossopharyngeal, upper laryngeal, trigeminal, auriculotemporal).
It is mandatory to examine the throat to rule out pharyngitis and tonsillitis.
An additional examination method is skull radiography (or targeted radiography of the stylohyoid process).
Diagnosis of stylohyoid syndrome in Pirogov
At the National Medical and Surgical Center named after N. I. Pirogov, the diagnosis is made by studying the anamnesis in conjunction with studies carried out in the clinic.
The disease is most often detected by the following method: palpation of the cervical spine or the fossa of the tonsillar part of the oral cavity occurs, resulting in pain.
Then the patient receives a referral for fluoroscopy, which confirms the diagnosis. There have been cases when an increase in the size of the stylohyoid process did not have a painful effect on patients. Before the pathology was discovered, they felt quite comfortable.