Size of modern human teeth
Over more than two million years, the size of teeth gradually decreased due to the transition to eating soft and processed foods. The first transformations affected the fangs - in primates they were larger and more strongly advanced relative to the rest of the row. The interdental spaces have disappeared, the size of the front teeth has become smaller. Refusal of raw meat led to a decrease in the chewing load and a narrowing of the jaw, as a result of which there was no room left for the “eights”. Now wisdom teeth are considered atavism and are often subject to removal.
How are tooth sizes determined?
To determine the size of a person’s permanent teeth, the calculation tables of Wetzel and V.L. Ustimenko with average standards and permissible deviations are used. However, an experienced dentist is able to independently identify the anomaly during a visual examination or by applying the formula for the ratio of the height and width of the natural crown. During diagnosis, the specialist takes into account the patient’s face shape and height. For example, with a wide jaw, the size of teeth exceeding the norm is not a pathology.
To determine the size of the root canal, there are also tables that indicate the average distance from its apex to the cutting edge or cusp of the tooth surface. The longest is the root of the canines - about 26 millimeters, the root canal of the incisors is 21 - 23 millimeters, and the size of the roots of the chewing zone and premolar teeth ranges from 19 to 22 millimeters.
What to do if the order and timing of the eruption of baby teeth in children is disrupted?
It is not uncommon for a child to cut his first milk teeth at the age of one year or even later, or, on the contrary, a four-month-old baby can already boast 1-2 incisors. Dentists and pediatricians recommend not to panic and not take any action. Under no circumstances should you start giving your child any medications or vitamins without a doctor’s prescription. The appearance and growth of primary teeth can occur according to an individual schedule, taking into account genetic predisposition.
If the baby is completely healthy, then parents should be patient and just wait. Primary (congenital) adentia is an extremely rare phenomenon. The complete absence of at least one tooth germ is found in less than 0.1% of newborns.
What to do if baby teeth are crooked?
No one can answer the question why children's baby teeth grow incorrectly. In the vast majority of cases, we are talking about hereditary predisposition or intrauterine malformations. In the photos and videos of babies you can see that the problem of crooked first baby teeth is quite common. So what to do in this case? Contact an orthodontist as soon as possible.
To correct malocclusion at a young age, the following are used:
- Vestibular plates of Dr. Hintz;
- Trainers and LM activators;
- Braces.
Often a permanent tooth appears under a baby tooth, breaking the orderly row. In this case, removal is often indicated, however, the final verdict remains only with an orthodontic specialist.
Teeth size for prosthetics
It is especially important to preserve and, if necessary, restore the natural size of teeth during prosthetics, so as not to disrupt the bite and the full functioning of the dental system. The size of the crown is selected by the dental technician, focusing on neighboring or teeth of the same name, monitoring the correct closure of the rows and adjusting the prosthesis during installation.
Determining the size of artificial teeth with complete edentia is carried out by measuring the distance between the corners of the mouth using a special ruler - it corresponds to the width of the six front teeth. And the segment from the edge of the gum to the smile line is equal to the height of the crown. For example, during implantation it is necessary to correctly calculate not only the parameters of the orthopedic design, but also the size of the dental implant. It should be equal in length to the real root, but the choice of titanium rod parameters depends largely on the volume of the jaw bone tissue.
Proportional ratio of teeth sizes
In most cases, specialists determine the proportions of a tooth by correlating its height and width. A result of about 0.75 is considered ideal. The most accurate diagnosis is carried out through the use of formulas.
- Gerlach's formula.
The method is based on the proportional ratio of the sizes of the front teeth and dental units of the chewing zone. The width of the crowns of the upper central incisors should correspond to the width of the four lower incisors. The canine, two premolars and one molar of both jaws are normally equal to each other. The width of the lateral part of the dentition is 10 mm greater than the width of the anterior segment. - Pon's formula.
The distance between the first premolars is equal to the sum of the widths of the four incisors multiplied by 100 and divided by 80, and the distance between the first molars is the sum of the widths of the four incisors multiplied by 100 and divided by 64. - Corkhouse formula.
The length of the segment from the midline to the first molar of the upper jaw should be 2 mm greater than the same distance on the lower jaw.
Numbering of teeth in dentistry
Numbering of teeth in dentistry
In world dentistry, several alternative tooth numbering options are used. In European countries, which includes the Russian Federation, the European International two-digit numbering system Viola is widely used. In America, the alphanumeric system is used. There is also the Haderup technique, in which the elements of the upper and lower row are designated by the symbol “+” or “-”, the Zsigmondy-Palmer scheme and the universal system, in which each element is assigned a serial number, and the numbering goes from right to left, starting with the right upper molar.
Practical meaning of numbering
From a practical point of view, tooth numbering in dentistry is very important. Firstly, it is necessary to fill out medical documentation, which is maintained by all dentists. Secondly, without it it is difficult to imagine coordinated interaction between doctors with different specializations (dental therapists, prosthetists, orthodontists, surgeons). How to inform a colleague about what elements of the dentition have been treated, especially when the patient receives treatment in different clinics? With the help of a single scheme this is quite simple.
A separate area of application of tooth numbering in dentistry is diagnostics. Numbering is used when describing a panoramic image or teleradiography. It is even more important when performing computed tomography, because a 3D image does not always allow one to understand which element of the dentition is depicted.
Finally, numbering simplifies communication between patient and specialist. Of course, the patient can explain and even show the doctor which tooth is bothering him. However, it is much easier to do this using a universal nomenclature or the correct names of teeth, with which we will begin a more detailed study of this issue.
What are the teeth called?
Each tooth has a unique name. The four front ones - two left and two right - are usually called incisors. Immediately behind them are the fangs. Behind the fangs begin the elements of the chewing group - premolars. The lateral elements are usually called molars.
Incisors are usually divided into medial (central) and lateral (lateral). Accordingly, each person has an upper left medial incisor and a left lateral, a lower central left and a lateral. The same exact elements are located on the right.
With fangs everything is much simpler. There are top left and right, bottom left and right. There are four fangs in total in the oral cavity, regardless of whether they are baby teeth of a child or molars of an adult.
There are two premolars in each half of the dentition. They are designated by a serial number, starting from the center line - the first left premolar from above, the second from the left, and so on.
There are the most molars - twelve in total. When designating them, the same principle is applied as when numbering premolars. An element of the dentition is named by a serial number indicating its location - in the upper or lower row, on the left or on the right.
Milk teeth have a significant difference. The child has no premolars, only two molars on each side. Accordingly, there are eight molars in total, and they should be named the same as those of an adult.
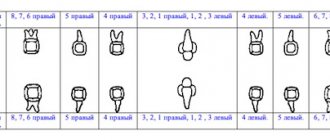
Viola system: European two-digit circuit
As we can see, even without any numbering, the patient can explain to the dentist exactly which tooth hurts. But it won’t be possible to describe a panoramic photograph of the jaws or fill out a medical card - the description will be too cumbersome. The orthodontist will encounter even more problems when installing braces. Each lock is designed for a strictly specific tooth, and it must be clearly indicated for which one.
To simplify the work of dentists and, more importantly, eliminate the possibility of error, the two-digit Viola numbering system was developed in 1971. The dental system is divided into four segments or quadrants. The right quadrant of the top row received index 1, the top left quadrant received index 2, the bottom left quadrant received index 3, and the bottom right quadrant received index 4. Thus, the first digit in the designation of a particular tooth refers to the segment in which it is located.
- 1 - right side of the top row.
- 2 - left side of the top row.
- 3 - left side of the lower jaw.
- 4 - right side of the lower jaw.
The second number indicates the location of the element in the dentition. Numbering begins with one and proceeds from the central incisors to the third molars. Accordingly, the lateral incisor is designated by the number 2, the first premolar by the number 4. The wisdom tooth receives the number 8.
By combining indices (designation of a segment) and serial numbers (indicating a specific tooth), we obtain a universal system that eliminates the possibility of error. For example, 32 is the lateral incisor of the left half of the lower jaw. 18 - third molar of the right half of the upper row. Obviously, such a nomenclature greatly simplifies both patient management in a dental clinic (stages of diagnosis, treatment) and communication between specialists.
Practical examples
Try giving a name to the maxillary canine on the left. The correct answer is 23. The index “2” is assigned to the element of the left half of the upper jaw. The number three is the number of the element in a given segment of the dentition. Fangs come third.
Another task. Which element is numbered 45? Index 4 unmistakably indicates the right half of the lower jaw. The second digit is the serial number. Fifth are the second premolars. So, 45 is the second right premolar of the lower row.
Viola system and baby teeth
The universalism of the international Viola system becomes obvious when describing teeth in children. For primary teeth, other indices are used:
- 5 - right half from above.
- 6 - left side of the top row.
- 7 - left half of the bottom row.
- 8 - right half of the bottom row.
The second digit indicates the element's serial number. Accordingly, 55 is the second primary molar on the upper jaw on the right. 71 - central incisor of the lower jaw on the left.
It happens that a child has already erupted some permanent teeth, but still has milk teeth. In such a situation, numbering according to the Viola scheme is very convenient. The dentist will write down 31 and 72 in the medical record. What does this mean?
This means that the central incisor of the left half of the lower row (31) has already been replaced by a permanent one, while its neighbor, the lower left lateral incisor (72), still remains one of the baby teeth.
The Viola numbering system was adopted by WHO and is recognized as the most universal, and therefore we paid maximum attention to it. We will not analyze other schemes in such detail, since they are used much less frequently in Moscow clinics.
Other numbering systems
Universal system. You can not divide the dental system into squares, but simply designate the elements by their serial number. The count starts from the upper right third molar and goes counterclockwise in a circle. Accordingly, 8 is the upper central incisor on the right, 10 is the left canine on top, 17 is the wisdom tooth in the bottom row on the left, and 25 is the medial incisor of the lower jaw on the right.
For baby teeth, the universal system uses not numbers, but letters of the Latin alphabet from A to T, which is not very convenient. The letters from A to E indicate the upper milk teeth on the right, from F to J - the left upper milk teeth, from K to O - the lower left milk teeth, from P to Q - the right milk teeth from below.
Haderup system. At first glance, this is a simple and convenient numbering system, but due to the constant use of the same numbers, only with different indices, when using it, the likelihood of error increases. According to the Haderup system, teeth are designated as follows:
- numbers from 1 to 8, where 1 is the central incisor, and 8 is the third molar;
- indexes + or -, where “+” denotes the teeth of the upper jaw, “-” denotes the teeth of the lower jaw;
- for baby teeth, 0 (zero) is placed before the serial number;
- when designating the teeth of the right half, the index + or - is placed to the right of the number;
- when designating the teeth of the left half, the index + or - is placed to the left of the number;
Examples of numbering according to the Haderup system:
- 8+: right maxillary third molar;
- -1: left mandibular central incisor;
- 02-: lateral primary incisor of the lower jaw on the right.
Alphanumeric system. The system was proposed by US dentists. In this numbering scheme, each type of teeth receives its own capital letter of the Latin alphabet, and the serial number of the element in a given group of teeth is indicated by a digital code. Baby teeth are numbered in exactly the same way, only small letters are used instead of capital ones:
- I (i) - incisors.
- C (c) - fangs.
- P - premolars (not in children).
- M (m) - molars.
Examples: I2 - lateral incisor. M3 - third molar. The first primary molar is numbered m1.
The disadvantage of the alphanumeric system is that it does not indicate in which jaw the element of interest to the doctor is located; it does not take into account whether it is on the right or left.
There are other systems for numbering teeth in dentistry, but they are considered imperfect and are practically not used today. In order not to confuse the reader, we will not dwell on them.
If you have questions regarding the timing of the eruption of primary and permanent teeth in children, oral hygiene, correction of malocclusions, diagnosis or treatment of dental diseases, ask them to a dentist at the Galaktika clinic (Moscow) during an individual consultation.
Normal and deviations in tooth sizes
All dental units of the same name have approximately the same height and width, except for the central (medial) incisors. The size of the front teeth of the upper jaw is normally slightly larger than that of the lower jaw. The height of the crown of the upper central incisors varies from 9 to 12 millimeters, width - from 8 to 9 millimeters. The lower teeth are similar in height, but are about 5 millimeters wide. The size of a person's wisdom teeth does not differ from the parameters of other molars. The table below shows the average width of dental crowns in millimeters.
| Upper jaw | Lower jaw | |
| Medial incisor | 8.5 mm | 5.3 mm |
| Lateral incisor | 6.5 mm | 6 mm |
| Fang | 7.6 mm | 6.7 mm |
| First premolar | 6.7 mm | 6.8 mm |
| Second premolar | 6.4 mm | 7 mm |
| First molar | 9.4 mm | 10 mm |
| Second molar | 9.4 mm | 10.2 mm |
Anomalies in the size of human teeth can be congenital or acquired and are accompanied by malocclusion, impaired chewing functions and an unaesthetic appearance of a smile. The most common deviations are macrodentia and microdentia.
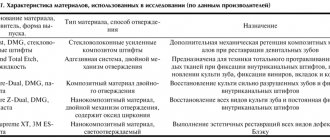
Fundamentals of clinical dental morphology: textbook
3.1.1. Maxillary medial incisor
The medial incisor of the maxilla is the largest in the group of incisors.
Near the cutting edge, the crown is flattened in the vestibular-lingual direction and is shaped like a shovel. The shape of the root is comparable to a cone, unevenly compressed from the sides.
To determine whether a tooth belongs to the right or left side of the dental arch, all three main signs of lateralization are used.
In vestibular and lingual norms
(Fig. the shape of the crown is close to trapezoidal, with a large base at the cutting edge.
the shape of the crown is close to trapezoidal, with a large base at the cutting edge.
Rice. 8. Medial incisor of the upper jaw, right.
a — vestibular norm; b - language norm
The occlusal contour is often uneven. In unworn teeth, the occlusal contour has cusps of the cutting edge, among which the outermost ones are more noticeable. The line of the occlusal contour passes into the approximal contours, forming the corners of the crown. The medial angle of the crown is pointed and smaller in size than the rounded distal angle (sign of the crown angle).
The approximal contours of the crown converge towards the neck of the tooth, and the medial contour of the crown is more inclined towards the USV than the distal one. The most prominent points on the contours of the contact surfaces are located near the border of the occlusal and middle third of the crown (the location of the equator of the tooth).
The line of the enamel-cementum border is curved towards the root, and on the lingual side the amplitude of the curvature is slightly greater than on the vestibular side. The point of greatest convexity of the enamel-cementum border in the vestibular and lingual norms is located near the USV.
The medial contour of the crown in the cervical region has a smoother transition to the corresponding contour of the root than the distal one.
The root is cone-shaped, with the apex deviated distally from the USV. In the lingual norm, both contact surfaces are visible on the root, converging in the lingual direction, so the shape of the root is more like a triangular pyramid.
On the vestibular surface of the crown there are two vertical grooves separating three vertical ridges, among which the extreme ones (medial and distal) are more pronounced. The ridges continue to the cutting edge in the form of three tubercles with a more pronounced medial one compared to the middle and distal ones.
The lingual surface at the edges bears two protrusions - medial and lateral marginal ridges, which are separated from each other by a small depression - a groove. The groove is delta-shaped, with diverging edges from the neck of the tooth. The marginal ridges, connecting with each other at the base of the crown, form a belt on the lingual surface. From the belt towards the cutting edge, along the cervical third of the crown, a convexity is noticeable - the tubercle of the tooth.
In medial and distal norms
(Fig. 9) the shape of the crown is close to a triangle, the most acute angle of which is formed at the point of transition of the vestibular and lingual contours into the occlusal one.
Rice. 9. Medial incisor of the upper jaw, right.
a - medial norm; b - distal norm
A short line of the occlusal contour, which in the lingual direction is slightly shifted towards the base of the crown, connects the vestibular and lingual contours. The point of connection of the occlusal contour with the vestibular one is located near the USV, often shifted to the vestibular side. The greatest convexity of the vestibular contour of the crown is located near the border of the cervical and middle thirds. The lingual contour has a convexity in the area of the lingual tubercle (usually in the cervical third) and a concavity along the remaining length to the incisal edge.
The line of the enamel-cementum border is curved towards the cutting edge of the crown with the point of greatest convexity located on the vestibular side of the USV. In the distal norm, the amplitude of the curvature of the enamel-cementum border is less pronounced than in the medial one.
The root is cone-shaped, with the apex located near the USV. The vestibular contour of the root, as a rule, has a convexity towards the vestibular side, and the lingual contour is often straight. In the medial norm, a vertical groove runs along the root. The distal surface of the root, in contrast to the medial one, is somewhat convex, with a smoothed relief.
In occlusal norm
(Fig. 10, a) the shape of the crown approaches a triangle with rounded corners. The mesial-distal size of the crown often prevails over the vestibular-lingual one.
Rice. 10. Medial incisor of the upper jaw, right.
a - occlusal norm and cut at the level of the base of the crown; b - tooth cavity.
The vestibular and lingual contours converge towards the distal angle of the crown. The vestibular contour has a slope in the medial-distal direction (a sign of crown curvature). The medial contour is wider than the distal one.
The cutting edge is relatively smooth and slightly wider in the area of the medial corner of the crown than the distal one. In unworn teeth, the tubercles of the cutting edge turn into ridges of the vestibular surface.
Horizontal sections of the root at different levels have the form of triangles with a rounded apex along the lingual contour.
On the medial contour of the root there is a depression (groove on the medial surface of the root).
Tooth cavity
corresponds to its external shape (Fig. 10, b). The crown cavity is flattened in the vestibular-lingual direction. Towards the cutting edge, the cavity of the crown forms depressions corresponding to the corners of the crown and the tubercles of the cutting edge.
Macrodentia
The tooth size exceeds the norm by more than 2 millimeters. Pathology occurs due to the fusion of two rudiments or the main and supernumerary teeth during the period of formation. The cause of macrodentia can be endocrine diseases, metabolic disorders or heredity. There are five types of pathology:
- localized - one or two teeth are significantly larger than the rest;
- generalized - the entire dentition differs in size from the other;
- isolated - enlargement of one medial incisor;
- absolute - the size of the teeth of both jaws exceeds the norm;
- relative - excessive growth of the upper or lower incisors.
Microdentia
The size of teeth in microdentia is less than anatomical standards. The list of reasons for deviation includes exposure to radiation, premature removal of a baby tooth, narrow jaw, and infectious diseases. There are several types of anomalies:
- isolated - a single violation affecting the lateral incisors;
- relative - the teeth are of normal size, but look smaller due to the enlarged jaw, as a result of which interdental spaces and diastema are formed;
- generalized - the defect covers a group of teeth.
Which baby teeth do children cut first?
Typically, the lower primary teeth erupt first, followed by the upper pair of antagonists. The first teeth always grow in twos, with a slight time difference.
So which tooth comes in first? First, 2 central lower incisors appear, then 2 central upper ones. Following them, the lateral incisors are cut in a similar sequence - first the lower, then the upper.
Then the lower pair of first molars erupt through a short space from the lateral incisors. A similar picture is observed from above. After some time, a pair of fangs will grow in this gap. The formation of a temporary occlusion ends with the appearance of second molars, which also erupt first from below and then from above.
Dentists and pediatricians allow some deviations in the order of eruption, designating this as a variant of the individual norm.