How do “eights” erupt?
Wisdom teeth are the last teeth to erupt. Sometimes at 18–20 years old, but more often at a later age. In addition to the fact that these are the largest teeth, there are cases when they are located in the jaw bone not vertically, but at an angle. Therefore, problems most often arise with their eruption: the tooth does not grow upward, but to the side, pressing on the root of the nearest tooth, causing pain and inflammation. Often, to avoid such problems, wisdom teeth are removed without waiting for them to fully erupt.
Wisdom teeth often cause problems when they erupt
But if the tooth grows more or less without problems, the person does not see a dentist; there is no indication for tooth extraction. And then it turns out that due to the growth of molar No. 3, the front teeth have moved.
“Eights” are large teeth, and if there is not enough space in the dentition, they move neighboring teeth, and even the front ones.
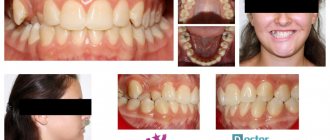
Crowded teeth
Is it possible to remove a tooth and return everything as it was?
If you remove a tooth, nothing will change. Orthodontist patients know that after treatment a consolidation stage is needed, otherwise the roots of the teeth will begin to move to their old familiar place. It takes at least two years for the teeth to adjust and strengthen in their new position, and to do this they are held in place with the help of retainers and aligners.
During orthodontic treatment, the pressure from braces or aligners is much greater than that exerted by the growing wisdom tooth. Therefore, with an orthodontic system, teeth are moved within a few months, and the first results are visible within a few weeks.
Aligners correct the position of teeth in a few months
A growing molar erupts very slowly, over 2–3 years, and puts pressure on neighboring teeth, causing them to move. The process occurs almost imperceptibly, the teeth shift by fractions of a millimeter per month. During this time, they get used to the new (wrong) position. The ligamentous apparatus that supports the teeth is rebuilt to a new position, and the bone tissue around the roots is strengthened. And even if wisdom teeth are removed, it will not be orthodontically beneficial. Neither from a health point of view, nor from an aesthetic point of view.
Signs of teeth: 1) sign of crown angle, 2) sign of crown curvature, 3) sign of root.
The belonging of teeth to a certain side of the jaw is determined by the general characteristics of the teeth. In this case, three signs are basic: the sign of crown angles, the sign of crown curvature and the sign of root position.
The sign of the crown angle
is expressed in the fact that the angle between the occlusal and medial surfaces is more acute than the angle between the occlusal and distal surfaces of the crown. The sign of crown curvature is determined by examining the tooth from the occlusal surface. In this case, the medial part of the crown on the vestibular side is more convex than the distal part. The enamel of the vestibular surface of the crown thickens in the mesial direction and has a steeper bend at the mesial edge than at the distal one. A sign of root position (visible only on a tooth extracted from the jaw, or on an x-ray) is characterized by deviation of the root distal to the longitudinal axis of the tooth crown.
Ticket 13
1. Muscles and fascia of the lower limb girdle. Muscular and vascular lacunae. Pelvic muscles - surround the hip joint. They start from the sacrum, pelvic bones and spine, and are attached to the proximal end of the femur. Topographically, they are divided into two groups: internal and external pelvic muscles. Internal muscles of the pelvis 1. The iliopsoas muscle (m. iliopsoas) consists of two muscles: the iliac muscle (m. iliacus), starting in the iliac fossa, and the psoas major (m. psoas major). Both muscles connect together and pass under the inguinal ligament. in the muscle lacuna and are attached to the lesser trochanter of the femur 2. The psoas minor muscle (m. psoas minor) is unstable, starts from the bodies of the XII thoracic and I lumbar vertebrae; attaches to the fascia iliaca.3. The piriformis muscle (m. piriformis) starts from the pelvic surface of the sacrum and passes through the greater sciatic foramen; attaches to the greater trochanter of the femur.4. The internal obturator muscle (m. obturatorius internus) starts from the inner surface of the obturator membrane and the inner surface of the pelvic bone around the obturator foramen; attaches to the trochanteric fossa. 1. The gluteus maximus muscle (m. gluteus maximus) starts from the outer surface of the ilium, from the dorsal surface of the sacrum and coccyx; attaches to the gluteal tuberosity of the femur.2. The gluteus medius and minimus muscles (mm. gluteus medius et minimus) are located under the gluteus maximus muscle. Start from the outer surface of the ilium; are attached to the greater trochanter of the femur.3. The tensor fasciae latae is located on the outer surface of the thigh. It starts from the iliac crest, from the superior external iliac spine, goes down and passes into the fascia lata, covering the muscles of the thigh.4. The quadratus femoris muscle (m. quadratus femoris) starts from the ischial tuberosity; attaches to the intertrochanteric ridge.5. The external obturator muscle (m. obturatorius externus) starts from the outer surface of the pelvic bone, from the obturator membrane; attaches to the trochanteric fossa. Muscles of the free lower limb 1. Quadriceps femoris 2. Sartorius muscle (m. sartorius). Biceps femoris muscle (m. biceps femoris 3. Semimembranosus muscle Pectineus muscle (m. pectineus). Long adductor muscle (m. adductor longus) starts from the superior branch of the pubis. Thin muscle (m. gracilis). 4. Short adductor muscle ( m. adductor brevis) originates from the lower branch of the pubic bone. Muscles of the lower leg Taught! let's list the Fascia of the lower limb iliac fascia Own fascia of the thigh - fascia lata The popliteal fossa (fossa poplitea) contains the vessels of the same name, the sciatic nerve and its branches, lymphatic vessels and nodes. Fascia shins, fascia cruris, -
intermuscular septa of the leg
to the fibula the anterior one,
septum intermusculare anterius cruris,
separating the peroneal muscles from the extensors, and the posterior one,
septum intermusculare posterius,
separating the extensors from the flexors.
Parietal and visceral branches of the abdominal aorta:
1. Inferior phrenic artery, a. phrenica inferior, - the first branch of the abdominal aorta, the steam room, departs from it in the aortic opening of the diaphragm at or above the celiac trunk (truncus coeliacus). On the way to the diaphragm, the artery gives off the superior adrenal arteries, aa. suprarenales superiores.2. Lumbar arteries, aa. lumbales, extend from the posterior semicircle of the aorta and go to the abdominal muscles. In their branching they correspond to the posterior intercostal arteries. Each artery gives off a dorsal branch, g. dorsalis, to the muscles and skin of the back in the lumbar region. The spinal branch, M. spindlis, departs from the dorsal branch, penetrating through the intervertebral foramen to the spinal cord. Visceral branches of the abdominal aorta. Among the visceral branches of the abdominal aorta, unpaired and paired branches are distinguished. The unpaired branches include the celiac trunk, superior and inferior mesenteric arteries. The paired branches of the abdominal aorta include the middle adrenal, renal, testicular (ovarian) arteries. Unpaired visceral branches of the abdominal aorta: 1. The celiac trunk, truncus coeliacus, begins from the anterior semicircle of the aorta at the level of the XII thoracic vertebra. Above the upper edge of the body of the pancreas, the celiac trunk is divided into three arteries: the left gastric, common hepatic and splenic.1) Left gastric artery, a. gastrica sinistra, gives off esophageal branches, gg. oesophageales, to the abdominal part of the esophagus.2) Common hepatic artery, a. hepatica communis, is divided into two arteries: the proper hepatic and gastroduodenal arteries. Proper hepatic artery, a. hepatica propria, gives off right and left branches, Mr. dexter et r. sinister. Gastroduodenal artery, a. gastroduodendlis, is divided into the right gastroepiploic and superior pancreaticoduodenal arteries. 3) Splenic artery, a. liendlis, gives short gastric arteries to the fundus of the stomach, aa. gastricae breves, and branches to the pancreas - pancreatic branches, rr. pancreatici. At the hilum of the spleen, the left gastroepiploic artery departs from the splenic artery, a. gastroepiploica sinistra. On its way, it gives off branches to the stomach - gastric branches, rr. gastrici, and to the omentum - omental branches, rr. epiploici.2. Superior mesenteric artery, a. mesenterica superior, originates from the abdominal part of the aorta behind the body of the pancreas at the level of the XII thoracic - I lumbar vertebra. This artery gives off the following branches: 1) lower pancreatic and duodenal arteries, aa. pancreaticoduodenales inferiores, depart from the superior mesenteric artery 2) jejunal arteries, aa. jejunales, and ileointestinal arteries, aa. iledles, originate from the left semicircle of the superior mesenteric artery. 3) ileocolic artery, a. ileocolica, gives off the anterior and posterior cecal arteries, aa. caecdles anterior et posterior, as well as the artery of the appendix, a. appendicularis, and the colonic branch, g. colicus, to the ascending colon; 4) right colon artery, a. colica dextra, starts slightly higher than the previous one. 5) middle colon artery, a. colica media, arises from the superior mesenteric artery.3. Inferior mesenteric artery, a. mesenterica inferior, starts from the left semicircle of the abdominal aorta at the level of the third lumbar vertebra, gives off a number of branches to the sigmoid, descending colon and left part of the transverse colon. A number of branches depart from the inferior mesenteric artery: 1) left colic artery, a. colica sinistra, nourishes the descending colon and the left transverse colon. 2) sigmoid arteries, aa. sigmoideae, directed to the sigmoid colon; 3) superior rectal artery, a. rectalis superior, supplies blood to the upper and middle sections of the rectum. Paired visceral branches of the abdominal aorta: 1. Middle adrenal artery, a. suprarenalis media, arises from the aorta at the level of the first lumbar vertebra.
2. Renal artery, a. renalis, departs from the aorta at the level of the I-II lumbar vertebrae, gives off the inferior adrenal artery, a. suprarenalis inferior, and ureteral branches, gg. ure-terici, to the ureter.
3. Testicular (ovarian) artery, a. testicularis, departs from the aorta at an acute angle below the renal artery, ureteral branches, rr. ureterici, and tubal branches, rr. tubdrii.
Solid sky. Its bone part, soft tissues, individual and age-related differences in shape. Palatal ridge. The mucous membrane, the nature and location of the submucosal layer in various parts of the hard palate.
The hard palate (palatum durum) consists of the bony palate (palatum osseum), including the palatine process of the maxilla and the horizontal plate of the palatine bone, and the soft tissues covering it. It is a partition that separates the oral cavity from the nasal cavity. The hard palate has two surfaces: the oral and the nasal, which is the bottom of the nasal cavity. The mucous membrane of the hard palate is covered with stratified squamous keratinizing epithelium and is tightly connected to the periosteum almost throughout. In the area of the palatal suture and in areas of the palate adjacent to the teeth, the submucosal layer is absent, and the mucous membrane is directly fused with the periosteum. Outside the suture of the palate there is a submucosal layer penetrated by bundles of fibrous connective tissue connecting the mucous membrane with the periosteum. As a result, the mucous membrane of the palate is motionless and fixed to the underlying bones. In the anterior section of the hard palate, in the submucosal layer between the connective tissue trabeculae, there is adipose tissue, and in the posterior section of the palate there are accumulations of mucous glands. Outside, at the point of transition of the mucous membrane from the hard palate to the alveolar processes, the submucosal layer is especially well expressed; Large neurovascular bundles are located here.
The mucous membrane of the hard palate is pale pink, and the soft palate is pinkish-red. A number of elevations are visible on the mucous membrane of the hard palate. At the anterior end of the longitudinal suture of the palate, near the central incisors, the incisive papilla (papilla incisiva) is clearly visible, which corresponds to the incisive fossa (fossa incisiva) located in the bony palate. In this fossa, the incisive canals (canales incisivi) open, through which the nasopalatine nerves pass. Anesthetic solutions are injected into this area to provide local anesthesia to the anterior palate.
What to do?
Treatment with braces or aligners will help correct the position of your teeth. However, it is not necessary to remove grown wisdom teeth. Whether to save them or not is decided individually in each case and only after examination. If it is possible to expand a row of teeth so that there is enough space for all teeth, then there may be no indication for removal. It is always better to preserve healthy teeth, this also applies to third molars.
If the teeth were initially straight and the erupting wisdom tooth has distorted them, a slight disturbance in the position of the teeth usually occurs. Regardless of the patient’s age, it can be corrected in a few months.
Complications of growing crooked teeth
Regardless of which teeth grow crookedly - baby or permanent - the consequences are completely identical. In addition, if the very first teeth grow crookedly, it is not at all necessary that the ones following them will also grow abnormally. However, the process must be monitored together with an orthodontist in order not to miss the moment when effective treatment can begin.
- Crooked teeth make maintaining oral hygiene significantly more difficult. In such cases, it can be very difficult to clean the entire surface of the tooth. In addition, curvature often causes food to get stuck in the interdental spaces, which increases the risk of developing caries,
- the inability to chew food normally can lead to problems with the gastrointestinal tract,
- Often, gum inflammation is the result of improper tooth growth, which is explained by the appearance of gum pockets between crooked teeth as a result of the impossibility of high-quality cleaning, and, as a result, periodontitis occurs. There is a constant chronic focus of infection in the oral cavity, which can cause the development of many diseases - in particular, diseases of the digestive tract and respiratory tract,
- With crooked teeth, a person may develop speech defects, because an incorrect bite prevents the full development of the speech apparatus.