Each person goes through the stages of the eruption of the first teeth, the development of milk teeth and their subsequent replacement by permanent ones. Despite their similar appearance and function, temporary and permanent teeth have differences, which we will talk about, at the same time we will consider the timing of the appearance of the main teeth, possible problems with them in the process of their development.
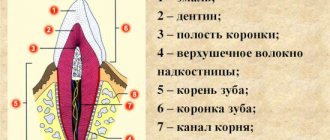
The photo shows a diagram of the structure of human teeth
The structure of human teeth
Teeth are not only intended for mechanical processing of food, but are also necessary for the formation of speech, breathing, and influence facial features. To navigate what dentists advise, how to take care of your teeth, and what the risks of disease are, it is useful to know how they work.
Anatomical structure
3 parts that make up a tooth:
- Crown. The visible part of the tooth used for chewing. The outside is covered with durable enamel, which protects it from bacteria, chemicals contained in food, water, and saliva. The surfaces have their own names: Facial (vestibular) - in contact with the lip or cheek.
- Lingual (lingual) – the opposite of the facial, involved in the formation of speech.
- Occlusion – the upper surface in contact with the tooth of the opposing jaw.
- Contact (approximal) – contacts with adjacent teeth.
Milk teeth, having a largely similar structure, also have differences in anatomy:
- They are noticeably smaller in height than permanent ones.
- The crown is much wider than the root.
- Enamel is thinner and more fragile.
- The roots are more round.
- The wear of baby teeth, as well as their spontaneous loss, is a normal physiological process.
Histological structure
The structure has several layers:
- Enamel is the most durable fabric. When a tooth just erupts, a cuticle is located on it, which is gradually, under the influence of saliva, replaced by a pellicle.
- Dentin is a highly mineralized tissue that resembles bone, but has better mechanical strength. Instead of enamel, the root part of the dentin is covered with cement.
- The pulp, the central part of the tooth, is a soft connective tissue containing a large number of blood vessels. Caries and inflammatory processes “owe” pain to the pulp with its large number of nerve endings.
Milk teeth are distinguished by dentin with a lesser degree of mineralization, which weakens their protection against caries. The volume of pulp occupies most of the tooth, and small protective layers (enamel and dentin) provide less protection against the penetration of bacteria and the development of inflammatory processes.
Types of teeth
There are 4 groups:
- Incisors. 4 chisel-shaped cutters. The largest are a pair of upper central incisors, and the situation is opposite from below - the lateral incisors are slightly larger than the central ones.
- Fangs. 2 on the upper and the same number on the lower jaw. Their length is longer than the others, the front wall is convex.
- Premolars. There are 8 in total, prismatic in shape, the upper surface with two tubercles (buccal and lingual). Premolars have 2 roots. The second premolar has a larger buccal surface. There are no primary premolars.
- Molars. The first molar (molar) is the largest tooth in the upper jaw. The chewing surface has four tubercles, 3 roots. The cubic-shaped second molar is smaller, and the buccal tubercles are larger than the lingual ones. The third (“wisdom tooth”) is in many ways similar to the second, but not everyone has it.
Eruption of permanent molars
The replacement of temporary teeth with permanent ones begins with the appearance of molars, which are not present in the primary dentition. They will be the first in the root and occupy the 6th position in the row. This process lasts for two years and begins when the child reaches 5-8 years of age. During this period, the resorption of the roots of temporary teeth begins, they gradually become loose and fall out. The age at which teeth change, as well as their appearance, is individual and depends on a number of factors. Including place of residence and gender. It has been established that boys become the owners of permanent teeth later than girls.
Next, at 10-12 years old, the first and second premolars are replaced. In this situation, they are the first and second molars of the primary occlusion. The second molars, whose serial number is seven, erupt in about a year. And the third molars complete the formation of the dentition. They are called wisdom teeth.
Dental formula
In order to improve the convenience of describing each tooth, numbering them, and filling out cards, it is customary to record the order of the teeth using a special formula. There are several varieties of it.
Zsigmondy-Palmer system (quadratic-digital)
Arabic numerals are used, numbering starts from the central incisors in each direction:
- 1 and 2 – incisors.
- 3 – fang.
- 4, 5 – premolars.
- 6-8 – molars.
Milk teeth are designated differently - using Roman numerals:
- I and II – incisors.
- III – fang.
- IV and V – molars.
Two-digit Viola system
Teeth numbering uses 2 digits. The jaws are divided into 4 quadrants. The first digit shows its number.
For adults this is:
- 1 – upper jaw on the right.
- 2 – upper jaw on the left.
- 3 – lower jaw on the left.
- 4 – lower jaw reference.
For a similar description of baby teeth, numbers 5 to 8 are used.
So, there are 8 teeth in each quadrant, its number is shown by the second digit. Thus, the first molar of the lower jaw on the left is designated 35, and the child’s canine from the lower right is designated 43. Therefore, the phrase that “treatment of the 48th tooth is required,” or, for example, the 55th, does not indicate the doctor’s lack of qualifications or what - or pathology in your child, who suddenly acquired so many teeth.
When do molars erupt?
Molars are the last teeth that erupt in the child’s lower and upper dentition. As a rule, the first units appear on the lower jaw at the age of 12-18 months, a month later molars erupt on the upper row. The second molars appear in a child between 24 and 30 months of age.
Replacement of primary molars of the lower jaw occurs at the age of 6-8 years. In place of the upper units, molars grow only by the age of 9-12 years. However, these are average indicators and may vary depending on individual characteristics.
The timing of eruption depends on the following factors :
- hereditary predisposition;
- the general health of the child;
- congenital features;
- climatic living conditions;
- nature of nutrition;
- gender of the child.
Dental development
The differences between primary and molar teeth begin with their number - only 20 primary teeth, 8 incisors and molars, and 4 canines. This is explained by the fact that children simply have nowhere to fit more teeth. In this regard, there are no primary premolars. By the time the permanent teeth appear, the adolescent's jaws are already sufficiently developed for all teeth to appear.
The formation of tooth buds in humans begins at the 6th week of intrauterine development, and at the 14th week hard dental tissue appears. The crown develops first. The development of the rudiments of permanent teeth begins in the 5th month.
By the time a child is born, the formation of the rudiments of both milk and permanent teeth is almost complete. The process of development of permanent teeth, which have no analogues among milk teeth, begins a year after birth.
While the first teeth may appear at 4 months, and their eruption may be delayed for up to a year, permanent teeth erupt in everyone at approximately the same age. The sequence of their eruption is the same as in the case of milkweeds:
- 6-7 years. The central incisors appear from below.
- 7-8 years old. The central incisors on top and the lateral incisors on the bottom are replaced.
- 8-9 years old. The lateral incisors of the upper jaw appear.
- 9-12 years old. Canines and premolars are replaced.
- From the age of 12. From this age, molars begin to change, and from about 14 years of age, teeth appear, which were not among the milk teeth.
What teeth are called premolars and their structural features
Premolars are the 4th and 5th small molars located behind the canines. Dentists call them chewables. An adult has 8 small molars, located in pairs on the right and left sides of both jaws.
Premolars are not primary; they erupt during the formation of a permanent dentition. In children, milk molar teeth take their place, and premolar teeth erupt after they fall out (see photo). This is due to the lack of space on a small child's jaw.
Premolars belong to the transitional type of dental units - in terms of the size of the dental crown and the structure of the root system, they are similar to canines, but in terms of the chewing surface area they are more similar to molars. The differences are clearly visible in the photo.
The main function of premolars is the same as that of canines - capturing, tearing and crushing food. But thanks to their wider chewing surface, they are also involved in grinding pieces of food.
The crowns of premolar teeth have a prismatic shape and two tubercles on the chewing surface. The upper premolars are anatomically different from the lower ones:
- The upper ones are larger, have a more rounded barrel shape and two channels.
- The lower molars usually have one canal.
Features of the lower premolars
Anatomically, the first premolar is similar to the adjacent canine. Its buccal surface is convex and longer than the palatal surface. There is usually one channel, but in rare cases there may be two.
The anatomical structure of the second premolar is similar to the second molar: the crown of the tooth is inclined inward, the sizes of the tubercles are approximately the same, between them there is an enamel ridge, separated from the edges by a horseshoe-shaped fissure. This structure allows it to withstand high chewing loads and grind food better. The second premolar dental unit has one cone-shaped, slightly flattened root.
Features of the upper premolars
The first premolar of the upper jaw, due to its pronounced vestibular cusp, visually resembles a canine. The crown has a prismatic shape, the buccal cusp is more pronounced than the palatal cusp, and between the cusps there is a deep groove that does not reach the edges of the crown. Enamel ridges are located along the edge of the chewing surface. There are two roots - buccal and palatine.
The size of the palatal root exceeds the size of the buccal root. Normally, they are separated in the apical region, but in dentistry there are cases of their separation in the middle and cervical region. There are usually two channels, in rare cases - one or three.
The second premolar is smaller than the previous one. Their structure is almost identical, except that the second has a less convex vestibular tubercle and one canal. A maxillary second premolar with two canals is a rare occurrence, occurring in less than a quarter of dental patients.
According to dental statistics, adult molars and premolars are especially susceptible to caries. This is due to their inaccessibility during cleaning and the complex structure of the tooth surface: the fissures covering it act as a favorable environment for the accumulation of pathogenic bacteria. Therefore, during oral hygiene procedures, it is necessary to pay increased attention to cleansing the coronal surface of the teeth located at the end of the dentition.
Signs of the imminent appearance of molars
You can determine when you should soon wait for the baby teeth to begin replacing with permanent teeth based on several signs:
- The gradual growth of the baby's jaws leads to increasing gaps between the teeth.
- The tooth begins to wobble. This is due to the fact that the already small root begins to gradually dissolve, causing the fixation of baby teeth to be significantly weakened.
- A fallen tooth indicates that the formed permanent one, which is about to appear, pushed it out.
- Swelling and redness may appear on the gums at the site of the eruption of a permanent tooth.
- Pain in the gums, where the permanent tooth erupts, increased temperature, and poor health of the child indicate problems have arisen, and it is necessary to see a doctor. The process of erupting molars should be painless.
Features and nuances that need to be taken into account during treatment
On the chewing surface of the molars there are tubercles and, accordingly, grooves - the latter are called fissures. They are cone-shaped, teardrop-shaped and grooved - they provide the ability to thoroughly crush and grind incoming food. Plaque settles in the fissures, food debris gets stuck, so they are especially susceptible to caries. More often in children's, but also in adult dentistry, a sealing procedure is carried out to prevent carious processes.
The photo shows chewing teeth
On a note! Many people call all chewing teeth “molars,” but this is not entirely true. In fact, premolars (small) and molars (large) are molars - their roots do not dissolve when the bite changes.
The first ones on the upper jaw are sixes
The first ones on top are considered the largest in the mouth. Their length can reach up to 2.5 cm. They have a diamond-shaped chewing surface on which there are four tubercles - two on the side of the cheeks and tongue. Moreover, the former have a conical shape, while the latter have a rounded shape.
On one of the anterior tubercles there is also an additional tubercle, and on the lateral surface on both sides there is a small groove. The surface on the lingual side is more convex. When a primary dentition changes, these sixth teeth are usually the first to grow. The process usually begins at the age of 5-8 years.
The photo shows the structure of the first upper molar
Second permanent molar – upper seventh
Slightly smaller than sixes in size, the second upper molars usually grow to 1.9-2.3 cm. The chewing surface is diamond-shaped or triangular with smoothed edges, 3-4 cusps, but without additional ones. In most people (about 57%), the upper second have 3 roots and 3-4 canals. In rare cases, there are 4 roots or the two front ones grow together.
The photo shows the structure of the second upper molar
Third or eight on the upper jaw
The eighth teeth in the top row, also known as wisdom teeth, are distinguished by their diamond-shaped or spike-shaped crown part. There can be from 2-4 to 6 tubercles on the chewing surface. The root system is often very twisted and tangled. Usually the top eights have 2-3 roots, less often their number varies from 1 to 4-5 pieces.
It should be noted that in about 15% of all people, wisdom teeth do not grow at all. It is believed that this is not an anomaly, but a natural evolutionary process. In fact, these are rudiments, the need for which a person lost quite a long time ago, as he developed and abandoned raw hard food in favor of heat-processed food. But to this day, for most of us, by the age of 20-25, eights begin to emerge - this process is usually difficult and painful, often accompanied by inflammation and in most cases requires complete removal of the problematic element.
The photo shows the structure of the third upper molar
Another difficulty is that the canals in the root system of third molars are almost always deformed and impassable. These teeth, as a rule, remain impacted and dystopic, that is, they do not erupt completely and initially grow in the wrong direction. When the inflammatory process occurs, tissue infection occurs, caries or pulpitis develops. It is almost impossible to cure a tooth with such a complex and difficult-to-reach root system. However, if the eights are completely fine, doctors leave them. Subsequently, they can become a good support for the prosthesis.
Sixths on the lower jaw
These are the largest molar teeth on the lower jaw, from 1.9 to 2.4 cm long. The diamond-shaped chewing part is covered with tubercles - 2 on the lingual side and 3 on the cheek side. They are separated by grooves - fissures. The crown is slightly inclined inward, the surface on the side of the cheek is voluminous, but not as convex as on the upper antagonist. There are usually 2 roots and 3-4 canals, in rare cases there may be 2.
The photo shows the structure of the first lower molar
Second lower molars and their features - sevens
The shape is almost identical to the neighboring sixes, but slightly smaller in size. Usually they have 4 tubercles, sometimes with a small additional one. They are also separated by fissures by longitudinal and transverse pits. They usually have 2 roots, but in some cases they grow together. There are usually 3 to 4 root canals.
The photo shows the structure of the second lower molar
Eights – wisdom teeth of the lower jaw
The crown of the figure eight can have a different shape, but there are usually 4-5 tubercles on the chewing surface. Most often there are 2 roots, but there are cases when there is only one. As on the upper jaw, on the lower jaw they grow dystopic or remain impacted, have a complex and difficult-to-reach root structure, and therefore are most often subject to removal.
The photo shows the structure of the third lower molar
Possible problems
At the moment the molars appear, certain dental problems are possible. In order to take timely measures to eliminate them, parents must have an idea about them.
Molars do not erupt
A situation is possible in which baby teeth do not fall out in a timely manner, or they have fallen out, but molars have begun to appear in their place. The reason for this must be determined by the dentist, who must be visited without delay. A general x-ray is usually taken to show the degree of development of the molars.
Among the options for the lack of eruption of molars in due time can be indicated:
- Hereditary predisposition, which is the cause of a possible delay in the appearance of molars. If the x-ray shows that the process of forming the rudiments of teeth is underway, then you will just have to wait a little for their appearance.
- Adentia. Disturbances in the processes of formation of tooth germs during the intrauterine development of a child, inflammatory processes can lead to a similar pathology - the absence or death of tooth germs. The solution is prosthetics.
Pain
The first time after teething, the tooth is poorly protected from caries and the effects of various bacteria. This is explained by the low degree of enamel mineralization at the initial stage. Almost nothing interferes with the development of caries; tooth tissue is destroyed, pulpitis occurs, with the subsequent risk of its transition to periodontitis. Severe pain, changes in body temperature and deterioration in well-being may occur.
It is highly advisable not to let the situation get worse, not to cause severe pain, but to visit a dentist as soon as painful sensations appear. If a child is predisposed to caries, it is better to carry out preventive procedures, for example, fissure sealing. The folds on the chewing surface are covered with a composite material that protects such natural cavities from the accumulation of food debris in them, the development of bacteria, and inflammatory processes.
In the worst case, you can lose a tooth.
Teeth grow crooked
A common situation is when the molar has already begun to erupt, but the baby tooth does not want to fall out. The result is that the new tooth seeks alternative growth paths, which leads to its displacement and change in the direction of growth. Hence the malocclusion and the alignment of the dentition. Treatment by an orthodontist will be required.
If this situation occurs, you should not remove or loosen a baby tooth yourself; you should visit a doctor.
Loss of molars
An alarming symptom of the presence of diseases (caries, etc.) in the oral cavity, or there are problems with the entire body (connective tissue diseases, diabetes, etc.). A visit to the doctor is mandatory.
This is necessary to develop a strategy for restoring a lost tooth. This is necessary for the proper growth of the remaining teeth and the formation of the maxillofacial system. Considering that the jaw tissue is still in the process of growth, prosthetics are only possible temporary, which must be adjusted as the jaws develop. Permanent prosthetics will be available only after their formation is completed.
Injuries
The first few years after teething, teeth are at increased risk of injury from impact. Sports injuries, falls, and blows can lead to chipping of parts of the tooth and cracks. Be sure to contact a dentist who will restore the lost part with modern materials.
Third permanent tooth (figure eight) of the upper jaw
The top eights are usually slightly smaller in size than their “neighbors.” The coronal part is diamond-shaped, sometimes spike-shaped. The chewing surface is represented by 3-4 tubercles, but sometimes there are 6 tubercles. The roots come in different shapes and are often curved (like their canals). Most often, the last molar has 2-3 roots. Less common are 1, 4 and even 5-root.
They are often impacted and dystopic, i.e. they do not erupt for a long time or grow incorrectly, injuring neighboring teeth, soft tissues, and causing pain. Often subject to removal, both on the upper and lower jaws. Treatment is difficult due to the strong curvature of the roots and canals and the fact that they are located very far away - it is difficult to get there. However, dentists are still trying to preserve the eights - they can become a support for the prosthesis. And if you remove them ahead of time, the rest of the row may move away.
Caring for children's teeth
The pattern of teething in children determines the approximate time of their appearance, but it is necessary to start observing oral hygiene as early as possible, without waiting for the teeth to erupt.
Breasts cannot take care of themselves, so they need help cleaning their gums. This is done either with the help of a fingertip, or, if there is none, with the help of an ordinary bandage dipped in warm boiled water and wound around the finger.
If teeth begin to erupt, you cannot do without the use of special products (baby pastes, brushes, etc.).
Structure and functions
The structure of molars includes two parts:
- pulp, that is, soft tissue;
- group of hard tissues - dentin layer, enamel, cement.
Anatomically, the following areas are also distinguished:
- crown part protruding above the gum tissue;
- neck in the form of a border between the crown and root system, clinical and anatomical parts are distinguished;
- root system that provides fixation, located deep in the bone structure.
Eights belong to this group of teeth, but they may not be present in everyone. They do not carry any special functional load; if problems arise during development or eruption, removal of wisdom teeth is recommended.