The upper and lower jaw system has a very complex anatomical structure. The bone structure is characterized by a high dependence on effective blood supply and necessary nutrition for full growth and development. The full functioning of the skeletal system is directly related to the presence of all elements of the dentition. Due to the removal or long-term absence of molars, various pathological processes of the alveolar process of the upper and lower jaw develop.
In accordance with the anatomical features and existing pathologies, correction or augmentation is carried out, bone tissue is built up for successful prosthetics. Appropriate periodontal treatment makes it possible to securely fix the implant in the oral cavity without the risk of possible complications. Augmentation is often done using bone-replacing biomaterials of artificial or natural origin. An integrated approach to diagnosing pathology and a highly effective treatment method allows you to achieve the desired result.
What is the alveolar process?
Bone tissue, consisting of the basal layer, spongy tissue and cortical plate, plays an important role in reliable fixation of the dentofacial system. As a result of everyday physical activity, it undergoes morphological and histological changes. The alveolar process (AO) to the anatomical part that holds the elements of the dentition of the upper and lower jaw. It is formed from the moment the teeth erupt and atrophies after their loss.
The process consists of inner and outer cortical plates and cancellous bone tissue. It is permeated with small tubules through which blood vessels and nerves pass. The anatomical structure of the ridge has an unpaired symmetrical structure; the holes may differ in shape and size depending on the placement of the dental units. Alveoli are located in the center of the alveolar ridge; most often they have a cone-shaped shape. As a result of pathology or loss of elements of the dentition, a significant decrease in the volume of bone tissue occurs, which will require restoration of the alveolar process for subsequent implantation.
Diagnostics and correction
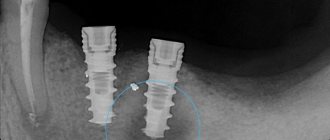
The pathological condition can be detected during a routine examination. In this case, the doctor prescribes an x-ray, which allows you to clarify the diagnosis and determine what the treatment regimen will be. Various methods are used to restore the structure; indications for correction are:
- atrophic processes affecting the ridge;
- defects caused by injuries, chronic diseases, surgical interventions.
Treatment is prescribed depending on the degree and severity of the pathology, tissue condition and other factors. The correction process usually includes the following steps:
- administration of anesthesia (conduction is used);
- surface treatment using antiseptic agents;
- removal of bone tissue particles, including fragments, if the cause of the intervention was injury or gradual destruction of the ridge;
- eliminating remaining sharp edges;
- closing the wound, applying sutures and dressings.
The exact procedure depends on the reason for the surgery, for example, you want to reduce a dislocation rather than remove sections of bone. To do this, a complete study is first carried out. After completing treatment measures, the Patient is required to comply with certain actions:
- exclude physical activity during rehabilitation;
- cessation of smoking, alcoholic beverages, and other bad habits;
- correction of the diet, exclusion of solid and spicy foods for the period of healing and recovery;
- observe the rules of personal hygiene, take care of the oral cavity;
- rinse your mouth after every meal using antiseptic agents.
Correction of the appendix is a complex stage of prosthetics or elimination of various pathologies caused by injuries or developmental disorders. Treatment should only be carried out by a qualified doctor with experience in this field.
Structure of the alveolar ridge
Taking into account the anatomical structure, the following parts are distinguished:
- Lateral. The outer wall located in close proximity to the cheeks and lips.
- Medial. The inner wall, which is directed towards the tongue and hard palate, has a compacted structure.
- Central. The location of the tooth sockets, the area has a large number of blood channels. This is where the molars and incisors are attached.
The alveoli and dental sockets are separated from each other by special bone partitions. In the alveolar part there are also interradicular septa. In the absence of functional loads on the ridge area, deformation of the alveolar process, changes in the anatomical structure and its reduction begin to be observed. The development of pathological processes in the upper and lower jaw often leads to a fracture of the alveolar process, which may require correction of this anatomical part.
Causes
Trauma often occurs in children when teeth change. This is due to the presence of molar follicles in the alveolar process, which makes the bone tissue more pliable.
Damage to the upper jaw is typical for people with malocclusion, namely, a sharply pushed forward upper jaw. In this position, she takes the blow first. In this case, part of the force is not transferred to the lower jaw, since it is located several millimeters or even centimeters behind.
Damage to the alveolar process can occur when there is a blow to the upper jaw, a fall from a height, or during an accident. In some cases, even a small amount of force can cause serious damage.
Predisposing factors include: osteoporosis, osteomyelitis, tumors and cysts. In patients with such bone tissue lesions, a fracture may occur spontaneously under the influence of minor force. Patients who are missing molars and premolars are also at risk because the load distribution during impact is disrupted.
Functions of the alveolar process of the upper and lower jaw
- Fixation and maintenance of elements of the dental system.
- Active participation in chewing food.
- Makes it easier to bite into hard foods.
The state of AO is reflected in a person’s external data. The development of pathologies often leads not only to a deterioration in the performance of molars and incisors, but also affects the anatomy of the facial skeleton. Over the years, the oxygen supply to bone tissue is disrupted, which leads to various defects of the alveolar process. As a result, this can cause loss of teeth, the development of traumatic injuries, periodontal disease, periodontitis and other dental problems.
Signs of pathologies of the alveolar ridge
- Predominant swelling of the mucous membrane in the area of the alveolar ridge.
- Pain when chewing food, swallowing saliva.
- Damage to gum tissue, bleeding.
- The appearance of multiple abrasions.
- Sharp expansion of interdental areas due to loss of incisors.
- Development of pathology of occlusion of elements of the dental system.
- The appearance of various speech defects, which can be expressed in a “lisp.”
In addition, hypertrophy of the alveolar process may develop, which is expressed in an increase in the volume of bone tissue due to histological changes. An external examination and x-ray may reveal a crack in the ridge or a complete separation of bone tissue from the fundamental cranial bone.
Numerous scientific works in dentistry, otorhinolaryngology, traumatology and plastic surgery are devoted to the study of the structural features and topography of the facial part of the head, gender characteristics and age dynamics.
The anatomical structure of the bones of a given area largely determines its functionality. In particular, the features of the maxillofacial area of the head determine the functional ability of the digestive and respiratory systems, the phonetic apparatus, and also have great aesthetic significance.
At the same time, the development of bone tissue of the alveolar process is of interest to specialists from the field of practical dentistry, including those involved in the issues of dental implantation. Understanding this process largely determines the outcome of treatment.
It is necessary to take into account the pronounced dependence of the structure of the maxillofacial region on a number of physiological and pathological factors, primarily on the age-related restructuring of the bone tissue of the jaws, in particular their alveolar areas.
Numerous sources of scientific literature contain a large amount of information about the course of these processes, but over the past decades there has been a pronounced tendency towards changes in their duration and timing compared to the data of fundamental research 40-50 years ago.
Obviously, the reasons for such deviations are various factors, the influence of which on the body has intensified over the past few decades, both in connection with technological progress and the lifestyle of modern man. First of all, the condition of the oral cavity, jaws and teeth is strongly influenced by improper and irrational nutrition, low level of oral hygiene, as well as living in environmentally polluted areas.
Factors that influence the course of the formation and development of both the body as a whole and the maxillofacial region in particular include the phenomenon of acceleration, which is also confirmed by numerous scientific sources.
The research results convincingly prove that today, much earlier than indicated in the sources of the last century, the processes of eruption and replacement of teeth occur, which means that the period of their intramaxillary development is significantly reduced. As a result, the degree of mineralization of their hard tissues at the time of tooth eruption into the oral cavity is insufficient, and this, in turn, leads to rapid destruction of crowns and premature tooth loss.
Sources of professional dental literature indicate that another cause of adentia is the high incidence of periodontal diseases. Domestic and foreign authors confirm that pathological processes affecting the periodontium extend to the bone tissue of the alveolar processes of the jaw, the mucous membrane of the gums and the root of the tooth, leading to the loss of practically healthy teeth and, as a result, the restructuring of the alveolar areas.
It is necessary to take into account the complex anatomical structure of the upper jaw and the presence of the maxillary sinus, characterized by individual differences, the relative position of the sinus, the roots of the maxillary dentition and the bone tissue of the alveolar process of the upper jaw in different age periods. An in-depth study of these anatomical formations is important to ensure high-quality restoration of the structure and functionality of the dentofacial apparatus in pathological conditions of various etiologies, as close as possible to physiological ones.
Patterns of formation of skull bones
The processes of formation and development of the musculoskeletal system, in particular the skeletal system, have always attracted the attention of researchers. Domestic and foreign authors continue to thoroughly study the features of development and age-related restructuring of the skull, especially its maxillofacial part.
Numerous scientific studies are devoted to the study of the characteristics of the formation of the skull during the intrauterine period of ontogenesis. The author of the fundamental work “Fundamentals of Medical Craniology” V.S. Speransky described 3 stages of the intrauterine period of skull development - membranous, cartilaginous and bone.
At the first stage, the components of the membranous skull are mesenchymal cords, the placement of which is associated with the growth of the embryo’s head. Starting from the fourth week of intrauterine development, the formation of a cartilaginous skull occurs, the development of which originates from the occipital bone and spreads in the ventral direction. Ossification of the cartilaginous skull begins in the 3rd month of intrauterine development, but in some bones of membranous origin, ossification centers appear earlier.
The process of ossification of the skull has been well studied, but the results obtained often differ significantly from each other (according to 28 authors, there are from 115 to 120 ossification centers in the skull, some of which lie in the cartilage, some in the mesenchymal base).
However, the vast majority of researchers argue that the first points of ossification in the areas of jaw formation are formed in the 7th week of embryogenesis, and the boundaries between individual bones of the skull at the sites of future sutures are visualized starting from the fourth month of intrauterine development.
It is known that most skull bones have several centers of ossification, and therefore at the time of birth of a child the number of skull bones is much greater than in adulthood, and the fusion of individual parts in such bones continues for a certain time after birth.
The characteristic appearance of the embryo is determined by the gill arches, which are formed during 4-5 weeks of intrauterine development. The formation of the jaws begins in the cartilage zone of the first branchial arch, which consists of a dorsal part (maxillary protrusion located under the orbit) and a ventral part (mandibular protrusion), which contains Meckel's cartilage and forms a kind of rod. Around the latter, the formation of the lower jaw occurs.
Numerous studies by morphologists, anthropologists, craniologists, as well as representatives of practical medicine, whose area of professional interest is the area of the head, as well as organs and systems associated with it functionally or topographically, have been devoted to the study of the patterns of development of individual bones of the skull.
V.S. Speransky claims that the formation of the skull is characterized by an uneven course in different time periods. In particular, until the end of the intrauterine period of development, the skull is 70-80% represented by formed bone tissue. In this case, the bones of the base of the skull are separated by cartilaginous layers, between the bones of the vault there are remnants of membranous tissue that forms the theme, expanding at the intersection of the sutures, and the bones of the facial skull are combined using syndesmoses.
The development of the head, the bony basis of which is the skull, after the birth of a child is characterized not only by an increase in size, but also by a change in the shape and spatial relationships of its component parts. In particular, this concerns the relationship between the brain and facial areas of the skull.
Each of them is characterized by a different type of growth and depends on the structural and functional characteristics of a given area. The bones of the cranium are structurally connected to the brain and its membranes, as well as to the sensory organs. The bones of the facial skull, primarily the jaw, are associated with teeth of both generations and depend on the course and duration of the processes of their formation, formation, growth, development, change and loss, as well as on the degree of pneumatization of the air-bearing bones.
The upper jaw, frontal and sphenoid bones contain air sinuses, and the ethmoid bone contains a labyrinth. All this determines certain features of the growth and formation of bones in the maxillofacial region, which today attract the attention of scientists and practicing doctors.
Growth and remodeling of skeletal bones in general, and the skull in particular, occur as a result of the synchronous flow of two interrelated processes - opposition and resorption of bone tissue. Thus, the restructuring of bone structures is especially important for the upper jaw, since simultaneously with changes in its size and external shape, processes of formation and restructuring of the maxillary sinus, anlage, development, eruption and replacement of teeth occur in the thickness of the bone body.
Another significant feature characteristic of the head skeleton is that at different age periods the intensity and direction of growth of the skull changes. This fact must be taken into account in pediatrics, especially in the practice of neurosurgery, otorhinolaryngology and maxillofacial surgery.
Craniometric studies show that the size of the head changes especially rapidly during the first 3-4 years of a child’s life. Their intensity decreases somewhat at the age of 5-6 years and intensifies again after 7 years.
At the same time, different directions of growth prevail at different periods of time, and the longitudinal and transverse dimensions of the skull alternately change. The periods of the most intensive growth of the skull in length are 2-3 and 7-8 years, and the most active growth of bones in width continues during the 1st year of a child’s life.
The results of craniometric studies tell us that the formation of the alveolar areas of the jaws and the associated vertical growth of the anterior part of the face is completed after reaching 10 years of age.
The directions of skull growth in individuals of different sexes during adolescence are different. In boys, during this period, longitudinal head growth prevails, and in girls, the size of the skull increases synchronously in the vertical and horizontal directions. Scientists agree that the increase in the size of the skull in width continues in girls up to 15, and in boys up to 16 years; in height - up to 16 years for girls, and up to 18 for boys.
However, with the end of the main stage of growth and formation of the skull, its restructuring does not end. Under the influence of local factors that determine the individual characteristics of each part of the face (the intensity of the load on the masticatory muscles, the prevalence of nasal or mouth breathing, bad habits), remodeling processes continue throughout life.
This fact must be taken into account not only during surgical interventions in this area, but when planning orthodontic or orthopedic measures.
Craniometric studies undertaken in various areas of the facial skull over various time periods indicate that in the fetal period the size of the jaws increases by 3-4 times, and the most active growth is observed in width. After birth and until the formation of the permanent occlusion is completed, increased growth of the maxillofacial region occurs, as a result of which the size of the jaws in three mutually perpendicular planes increases by 7-9 times.
Development of bones of the maxillofacial region and alveolar process
Since with age the growth rate in individual areas has different dynamics, the proportional ratios of the width, height and length of the jaws change significantly throughout life. Consequently, in each age period, regardless of the general gradual slowdown in the rate of bone growth, the jaws have areas of increased and relatively slow growth.
In areas of increased growth, a quantitative increase in bone structures occurs, and in areas of slow growth, their qualitative restructuring occurs. In this regard, growth zones should be understood not as permanent, clearly defined areas, but as places where, in a given period of time, opposition processes prevail over resorption processes.
In adults, the formed upper jaw (UM) is a paired bone of a complex structure, consisting of a body and four processes - alveolar, palatine, zygomatic and frontal. The thickness of the bone body contains the air-bearing maxillary sinus (MSS), and the cells of the alveolar process contain fixed tooth roots that form the maxillary dentition.
Research shows that the alveolar process is built of spongy bone tissue, covered with a compact layer, which is better expressed on the palatal side. This structure of the bone tissue of the HF in general and the alveolar process in particular is largely determined by the load acting on the bone during chewing.
It is due to the uneven load, which is distributed and spread in a certain way by the bone beams, that in certain areas of the processes and body of the upper jaw its spongy structure is compacted, forming buttresses and thus changing the external relief of the bone.
The presence and severity of buttresses is associated both with the presence or absence of teeth (after their loss, not only the area of the alveolar process of the jaw is resorbed, but also bone tissue, a buttress is formed at the level of a given dentofacial segment and along the line of pressure distribution), and with the condition of periodontal tissues, pathology which changes the distribution of chewing load on the jaw.
Some studies are devoted to the structural features of the maxillofacial region and structures of the oral cavity, depending on the constitutional structure of the skull. The results of anthropometric studies indicate that dolichocephals always have a high palate and high alveolar processes of the upper jaw, while brachycephals always have a low palate and low but massive alveolar processes.
In adulthood, after the completion of the basic formation of the permanent occlusion and growth of the skull, a number of factors are identified that influence the condition of the bone tissue and the functional ability of the jaws. These include the general condition of the body, the presence or absence of chronic diseases and metabolic disorders, as well as the method of nutrition, which determines the load on the teeth, periodontium and jaw bone tissue.
However, of course, the main factor determining the characteristics of jaw restructuring in adulthood is the preservation or loss of teeth.
Among the causes of acquired adentia, trauma is common, as well as tooth loss due to periodontal diseases, complications of carious lesions and pathological processes in the bone tissue of the jaws (periostitis, osteomyelitis).
Restructuring of the bone tissue of the alveolar process of the upper jaw and the alveolar part of the lower jaw after tooth loss consists not only of a decrease in bone mass, a decrease in the height of the alveolar process at the level of one or several dentofacial segments. According to research results, with edentia, the quality of bone tissue also changes - the volume decreases due to a significant thinning of the bone layers, which is also confirmed by a decrease in their density.
According to a number of authors, whose professional interests concern the state of bone tissue and its age-related dynamics, changes in the density of skeletal bones, as well as its individual parts, are due to several systemic and local reasons.
General reasons include, first of all, age-related metabolic changes occurring in the body - changes leading to a decrease in the content of mineral elements (calcium) in the bones, as well as organic compounds. This mainly implies the development of osteopenia and osteoporosis.
Most scientists consider the main local reason for the decrease in the quality of bone tissue of the maxillofacial region and alveolar process to be the redistribution of the load during chewing - a sharp decrease and uneven distribution of pressure on bone tissue in edentulous areas with various types of tooth loss.
After tooth loss, atrophy of the alveolar processes occurs differently in dolichocephals and brachycephals. When the size of the alveolar process is small, bone atrophy under the influence of compression pressure increases, which causes a change in the width of the arch. The processes of bone tissue resorption have different intensities in different zones of the cellular areas, but they are most pronounced on the vestibular side.
When teeth are lost, atrophy of the alveolar process is not only an aesthetic problem. It leads to a change in the proportions of the face and may in the future become the root cause of the restructuring of a number of anatomical formations, including the displacement of the neurovascular bundles passing through the incisive and palatal canals, individual facial muscles, as well as all masticatory muscles, asymmetry of the jaws and dentition, and, as the consequence is dysfunction and even destruction of the temporomandibular joint.
Another important factor to consider when examining dental patients is the different visualization of the alveolar process in different areas of the jaw. In particular, in the central part of the jaw at the level of the incisive and canine dentoalveolar segments, the height and shape of the alveolar process are well visualized, and changes in their morphological parameters can be detected in a timely manner.
But in the lateral areas of the alveolar process, primarily at the level of segments of large molars, manifestations of bone resorption will be more difficult to establish, especially taking into account the shape, size and topography of the maxillary sinus.
Therefore, often an objective determination of the condition of the bone tissue of the alveolar process of the upper jaw in the lateral areas, both in the presence of teeth and in edentia, is impossible during a standard dental examination and requires additional examinations.
When planning surgical and orthopedic measures aimed at restoring the aesthetic appearance and functional ability of the maxillofacial area, it is necessary to take into account not only the condition of the bone tissue in general and the degree of atrophy of the alveolar process of the upper jaw in a certain area in particular, but also a number of others, no less important factors. These are the patient’s gender and age, the presence of systemic and chronic diseases, diet and quality of nutrition.
It is also necessary to take into account local factors that affect the condition of the bone tissue of the jaws, in particular the volume of previous dental interventions and the dental status in general, including the shape of the palate and the type of bite.
It should also be remembered that the presence of the maxillary sinus in the thickness of the body of the upper jaw of an adult person contributes to significant relief, but at the same time, weakening of the bone. Most often, the lowest point of the sinus is located in the projection of the first large molar, although both the shape and size of the sinus are characterized by significant variability, as well as their symmetry and relationship with the roots of the maxillary teeth.
Given the presence of a large number of scientific publications on the peculiarities of the formation and development of the maxillary sinus, its relationship with the rudiments (in the process of formation) and roots of teeth of the milk and permanent generation of teeth, the main emphasis in the study of this area is on its pathology. About 15-30% of patients in otorhinolaryngological and dental clinics suffer from sinusitis of various etiologies.
In the scientific literature we find the results of studies devoted to the study of the shape, size and degree of pneumatization of the sinuses, their topography and features of the relationship with the roots of the teeth of the upper dentition in adults and the rudiments of various groups of teeth in children and adolescents during all stages of the formation of the primary and permanent dentition.
Morphometric, radiographic and tomographic studies make it possible to classify the maxillary sinuses in accordance with the characteristics of their structure (size, shape) and the degree of pneumatization.
Researchers distinguish three types of maxillary sinuses:
- Pneumatic type: the sinus is large in size, with thin walls, the bottom goes deep into the thickness of the alveolar process, forming so-called bays, the roots of large and small molars are separated from the bottom of the sinus by a thin bone plate, and often directly contact the mucous membrane of the sinus.
- Sclerotic: the maxillary sinus is of small volume with pronounced, fairly massive bone walls.
- An intermediate type, having average characteristics between the first and second types of anatomical structure.
The relationship between the bottom of the maxillary sinus and the roots of the teeth of the upper dentition is also of great importance for practical dentistry and otorhinolaryngology.
As dental practice shows, 20% of patients have a risk of developing odontogenic sinusitis in the presence of dental pathology or dental manipulations on the teeth and periodontium of the upper dentition, since the roots of these teeth are located in the area of the bottom of the upper jaw or penetrate into the cavity. Only in 45-50% of dental patients the apices of the roots do not fit the bottom of the sinus, and the thickness of its bone wall is sufficient, that is, from 1 to 15 mm.
Of course, the cavity and walls of the upper jaw are characterized by certain age-related changes. If the formation of the sinus and its walls is completed with the completion of the formation of the permanent occlusion and the growth of the skull as a whole, then after 40-45 years, thinning of the bone walls of the sinus is observed, which progresses with age and leads to an age-related increase in bone pneumatization.
The distal areas of the upper jaw differ in a number of characteristic anatomical features. First of all, such features include the close location of the pterygoid venous plexus and the branches of the maxillary artery.
It is this topographical position of these structures that is important when planning surgical operations. Since older people have varying degrees of severity of alveolar process atrophy, during surgery the likelihood of vascular injury and massive bleeding increases.
Implications for practical dentistry
An analysis of the sources indicates that the restructuring of the maxillofacial region does not stop with the completion of skull growth, but continues throughout life.
Age-related features of the structure and topography of the maxillofacial region are closely related to a number of factors (from the general condition of the body to the method and mode of nutrition) and must be taken into account when planning therapeutic, preventive or rehabilitation measures.
It must be remembered that changes in the bone tissue of the jaws, which are quantitative in nature and diagnosed during examination of patients, are, as a rule, irreversible. Therefore, the presence or absence of qualitative changes in bone tissue, which can only be detected by additional examinations using radiation methods, is of decisive importance for dental practice.
Such an examination is necessary for the correct choice of treatment tactics for dental implantation to restore the integrity of the dentition and functionality of the jaws, and timely detection of qualitative changes in the bone tissue of the alveolar process of the jaws opens up opportunities for optimizing the choice of treatment.
Knowledge of the structural features of the maxillofacial region, understanding the patterns of their age-related dynamics is important for practical dentistry, since one of the main prerequisites for adequate diagnosis and treatment of pathological processes localized in this area.
Causes of alveolar process atrophy
- Injuries, mechanical damage to the area.
- Morphological changes associated with significant disruption of blood circulation.
- Formation of uneven edges of the alveoli after the removal of dental units.
- Osteomyelitis of the alveolar process, inflammatory processes of bone tissue.
- Neoplasms, cysts that lead to ridge degeneration.
- Loss of elements of the dental system.
Other causes of the development of pathological processes may include chronic inflammatory processes, fibrous osteitis, which is expressed in the thinning of the bone structure, or tumors of the alveolar process. Pathology may also be associated with hereditary factors and genetic predisposition. In all these cases, correction and immediate intervention by a dental surgeon are required, since the tissue itself does not recover.
Diagnosis of diseases of the alveolar process
In order to correctly select a therapeutic or surgical treatment method, an appropriate set of diagnostic procedures is carried out: blood tests, radiography. Additionally, MRI, CT of the upper jaw, and biochemistry may be prescribed. The last analysis is prescribed if there is a suspicion of metabolic disorders in the body. Densitometry and orthopantomogram are also prescribed as diagnostic procedures. Comprehensive diagnostics allows you to build the correct correction tactics.
Treatment and restoration of the alveolar process
- Split-Control technology. The main purpose of this procedure is to expand the jaw bone to allow subsequent implantation. The procedure is performed as follows. The specialist saws the comb, places biomaterial, a bone tissue substitute, into the cavity, and applies sutures.
- Intercortical osteomia. It involves splitting the alveolar process to correct the bone structure. During the surgical intervention, the ridge is cut to form a movable fragment, which the dental surgeon then moves to another part where there is a lack of bone tissue. The moving part is fixed with special screws, and the cavity is filled with biomaterial.
The rehabilitation time after surgery and resection of the alveolar process can be several months. After this, you can begin to implant the implant. In each case, you must consult directly with your dentist. He will track the dynamics and determine the condition of the alveolar process in which there was a cleft or damage.
Why is the procedure needed?
The alveolar process is the basis for holding the implant in the jaw bone. Due to the lack of chewing load, the bones gradually thin out and become looser, decreasing in size. This makes it difficult to securely fix the implant.
The longer you put off going to the dentist after losing teeth, the more difficult it is to restore your dentition by installing implants.
Implantation is also difficult to do if the jaws are deformed. It is provoked by neoplasms in the mouth, severe infectious diseases, and injuries of the maxillofacial apparatus.
Therefore, in case of atrophy and deformation of bone structures, bone grafting is prescribed before implantation, in particular, expansion of the alveolar ridge using the splitting method.
Benefits of bone grafting
- Reliable adhesion of the implant to the bone tissue.
- Minimal trauma. Minor swelling and hematoma.
- High efficiency. Allows you to start prosthetics in a short time.
Before performing correction of the alveolar process, it is necessary to make sure that there are contraindications, for example, the absence of an allergic reaction to biomaterial and drugs. Dental treatment is not carried out for cancer and autoimmune diseases, as well as poor blood clotting. In some cases, surgery may be delayed until the underlying conditions have resolved.
Why is the operation performed?
In the presence of a narrow ridge, it is impossible to carry out high-quality dental restoration, especially on toothless jaws. The jaw may have this shape naturally or acquire it as a result of atrophy, injury, removal of a tumor, or a previous disease. Indications for surgical intervention:
- Insufficient tissue volume.
- Thin alveolar process.
- Atrophy or other defects of the jaw.
Recommendations for rehabilitation
The rehabilitation period is aimed at restoring the functions of the affected area. After surgery it is recommended:
- Follow all doctor's recommendations.
- Avoid eating too cold or hot food.
- Follow the rules of oral hygiene.
- Avoid serious physical activity.
- Follow the recommendations for a gentle diet.
Additionally, oral baths using antiseptic solutions and the use of soft toothbrushes may be recommended to eliminate the risk of damage to the operated area. If you follow the recommendations, there are no risks of possible complications. Successful recovery depends on the skill level of the surgeon. Our AlfaDent clinic employs exclusively professionals who take advanced training courses and regularly improve their skills.