Since the creation of the modern structure of dental care, the medical record of a dental patient has been its basic element. It existed when there was no trace of other documents, without which it is impossible to imagine the work of a modern clinic (contract, protocol of voluntary informed consent, insurance policy, etc.).
At the same time, many dental clinics completely or partially ignore the role of the dental patient’s medical record: they either do not use it at all, or they modernize, modify, or invent their own versions. And if the use of various variations on the theme of a dental patient’s medical record can be understood (in many ways, the existing form already lags behind the requirements of the time), then the complete absence of a medical record is completely unacceptable.
What is a dental patient's medical record?
A medical record of a dental patient is a document that properly identifies the patient and contains information characterizing the characteristics of the condition and changes in the state of his health, established by the doctor and confirmed by laboratory, instrumental and instrumental research, as well as the stages and features of the treatment.
Registration of a medical card for a dental patient –
The medical record of a dental patient is drawn up in accordance with orders of the USSR Ministry of Health No. 1030 of October 4, 1980 and No. 1338 of December 31, 1987. At the same time, the Ministries of Health of the USSR and the Russian Federation managed to create extreme confusion with the medical record. In 1988, an order of the USSR Ministry of Health was issued (No. 750 dated 10/05/1988), according to which the Order of the Ministry of Health No. 1030 became invalid. However, another, newer Ministry of Health, now the Russian Federation, since 1993 began to regularly refer to the provisions of Order No. 1030 of the USSR Ministry of Health, introducing appropriate changes and additions to it.
There are no later basic orders or other acts of the Russian Ministry of Health establishing the form of a medical record. Therefore, although many provisions of Order No. 1030 have lost force, new regulatory documents periodically contain references to those parts of the order that relate to the maintenance of medical records. In particular, the requirement remains that all medical institutions (note, regardless of their form of ownership) are required to maintain medical records in the established form. In dentistry, this is Form No. 043/у “Medical record of a dental patient.”
What does a medical card include?
Medical record No. 043/u contains three main sections.
1) The first section is the passport part. It includes:
- card number;
- date of its registration;
- last name, first name and patronymic of the patient;
- patient's age;
- patient's gender;
- address (place of registration and place of permanent residence);
- profession;
- diagnosis at initial visit;
- information about past and concomitant diseases;
- information about the development of the present (which became the reason for the initial treatment) disease.
This section can be supplemented with passport data (series, number, date and place of issue) for persons over 14 years of age, and birth certificate data for persons under 14 years of age.
2) The second section is data from objective research. He contains:
- external inspection data;
- oral examination data and a table of dental condition, filled out using officially accepted abbreviations (absent - O, root - R, caries - C, pulpitis - P, periodontitis - Pt, filled - P, periodontal disease - A, mobility - I, II, III (degree), crown - K, artificial tooth - I);
- description of bite;
- description of the condition of the oral mucosa, gums, alveolar processes and palate;
- X-ray and laboratory data.
3) The third section is the general part. It consists of:
- examination plan;
- treatment plan;
- treatment features;
- records of consultations, consultations;
- clarified formulations of clinical diagnoses, etc.
The procedure for examining a patient and filling out a medical history during orthopedic treatment
- home
- For patients
- Articles
- The procedure for examining a patient and filling out a medical history during orthopedic treatment
- 1. Last name First name Patronymic (of the patient).
- 10. Type of bite.
- 2. Current complaints.
- 11. Language.
- 3. History of the disease.
- 12. Additional examination methods.
- 4. General condition.
- 13. Diagnosis.
- 5. External inspection.
- 14. Plan for preparing the oral cavity for prosthetics.
- 6. Research of TMJ.
- 15. Orthopedic treatment plan.
- 7. Objective data.
- 16. Diary.
- 8. Inspection of the system.
- 17. Dispensary observation.
- 9. Examination of teeth and dentition.
- 18. Epicrisis.
Last name First name Patronymic (of the patient).
Current complaints: impaired chewing, aesthetics, tooth mobility, increased sensitivity of teeth, pain in the TMJ, pain under the base of a removable denture, poor fixation, pain in the tooth under the crown, bleeding gums, bad breath, suppuration, swelling of soft tissues , taste disturbances, etc. Complaints about parafunctions of the masticatory muscles (is there a habit of biting your lips or clenching your teeth while watching a movie, reading books or working, is there a habit of grinding your teeth, complaints from the masticatory muscles (pain, fatigue)).
History of the disease: when did certain complaints appear, what is it associated with (caries, periodontitis, periodontal disease, trauma, surgery, etc.), whether treatment or prosthetics were previously carried out (how long ago?).
General condition: presence or absence of bad habits (smoking, drinking alcohol), concomitant diseases (chronic diseases; hepatitis, tuberculosis, syphilis, HIV), allergy history, whether anesthesia was previously performed during treatment, tooth extraction, its effectiveness.
External examination: skin color, presence of defects, symmetry and type of face (conical, obverse-conical, square, round), height of the lower third of the face, protrusion of the chin, pattern of lip closure, severity of nasolabial and chin folds.
Research of the TMJ: opening of the mouth (intermittent, free, the nature of the movement of the lower jaw is smooth or jerky, displacement of the lower jaw to the side), the presence of crunching, clicking, noise in the TMJ when moving the lower jaw.
The state of the tone of the masticatory muscles and their soreness on palpation, the state of the submandibular lymph nodes, their soreness and size on palpation.
Objective data
| 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
Inspection of the mucous membranes: color and moisture content of the mucous membranes, color and shape of the gingival papillae.
Examination of teeth and dentition:
- condition of intact teeth (size, anomalies of position, shape, color of hard tissues, mobility, exposure of necks or abrasion of teeth (degree), sensitivity (type: hot, cold, sour, sweet, etc.), size of periodontal pockets);
- condition of teeth with defects of hard tissues (size and topography of the defect, condition of fillings is satisfactory or not, IROPD, mobility, exposure of necks or abrasion of teeth (degree), sensitivity (percussion, probing, temperature reaction), size of periodontal pockets);
- condition of inlays, veneers, pin structures (size, topography, condition, correspondence to the bite, mobility of the abutment tooth or prosthesis, exposure of the necks (degree), sensitivity), crowns, bridges (size, topography, condition, correspondence to the bite, mobility of the abutment teeth, exposure of the necks of the supporting teeth, sensitivity, abrasion of the chewing or other surface of the dentures), the size of the periodontal pockets of the supporting teeth;
- condition of removable dentures (type, integrity of the base and prosthesis fixation systems, service life, fixation of the denture in the oral cavity, balance, compliance with boundaries).
Type of bite: fixed, not fixed; orthognathic, direct, biprognathic, prognathic, progenic, cross, deep, open.
Condition of the dentition: shape, size and topography (classification) of defects, secondary deformations and movements of teeth.
Condition of toothless jaws: classification of the upper jaw (Doinikov, Kurlyansky, Oksman, Schroeder), lower jaw (Doinikov, Keller, Kurlyansky, Oksman); degree of mucosal compliance according to Supple; attachment of the frenulum of the upper and lower lips, buccal-gingival cords.
Tongue: size (normal, microglossia, macroglossia), shape (round, oval, V-shaped), attachment of the frenulum of the tongue.
Additional examination methods: description of x-ray examination (intraoral x-ray, panoramic x-ray, orthopantomography, targeted x-ray of teeth), description of diagnostic models, study of loss of chewing efficiency according to I.M. Oksman
| teeth | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Total |
| V/H | 1 | 1 | 2 | 3 | 3 | 6 | 5 | 4 | 25% |
| LF | 2 | 1 | 2 | 3 | 3 | 6 | 5 | 3 | 25% |
Diagnosis is a logical conclusion, a synthesis of the obtained subjective and objective research data. The diagnosis in orthopedic dentistry should reflect the size and topography of defects in the hard tissues of teeth, dentition, the condition of the oral mucosa, as well as concomitant diseases of the dental system and complications.
For example:
- a defect in the hard tissues of the tooth (necessarily which one?), carious, non-carious or traumatic origin (non-carious diseases include: enamel hypoplasia, wedge-shaped defects, fluorosis, acid necrosis and pathological abrasion; trauma - acute and chronic), the degree of destruction of the coronal part of the tooth must be indicated .
- partial edentia (which jaw?) according to Kennedy: bilateral end (I class), unilateral end (P class), included in the area of the lateral teeth (W class), isolated included in the frontal region (1U class). Complications: traumatic occlusion, decreasing bite, secondary deformation (Godon-Popov phenomenon).
- complete adentia: degree of atrophy according to I.M. Oksman, pliability of the mucous membrane according to Supple.
Plan for preparing the oral cavity for prosthetics: sanitation of the oral cavity (removal of dental plaque, dental treatment, removal of teeth or roots); special preparation (depulpation of teeth, elimination of occlusal disorders, orthodontic preparation, alveolotomy, excision of scars, strands of the mucous membrane, deepening of the vestibule or floor of the oral cavity).
Orthopedic treatment plan:
- Inlay, veneer from what material and for what tooth;
- Pin structure (single-root, dismountable, how it is made, temporary, permanent) on the abutment tooth;
- Single crown (from what material) on the abutment tooth;
- The bridge prosthesis is made of what material, supported by what teeth;
- Partially removable laminar denture on the upper part, lower part, with which teeth (plastic, ceramic, porcelain), clasps on which teeth;
- Clasp prosthesis (splinting clasp prosthesis) indicating the fixation system (cast clasps, type of attachments, telescopic crowns) and on which teeth;
- Other types of structures are possible, indicating the type of materials, manufacturing method and supporting teeth.
Diary: displays the date of patient admission, the amount of work performed and must be certified by the signature of the immediate supervisor.
Dispensary observation: if necessary, the date of examination (year, month) of the subsequent visit for the following diseases is noted: pathological abrasion, periodontal tissue diseases, complete edentia, etc.
Epicrisis: describes the scope of orthopedic treatment (aesthetics, anatomical shape of teeth, integrity of dentition, height of the lower third of the face, tooth mobility), indicates the extent to which chewing efficiency has been restored (according to I.M. Oksman), and provides recommendations for oral care and the use of prostheses.
ILLUSTRATIVE EXAMPLE
“Maintaining an outpatient card for a dental patient”
Last name I.O.: Ivanov V.P.
Year of birth: 1991.
Current complaints: disturbances in chewing and aesthetics.
History of the disease: a day ago, the crown of the central tooth of the upper jaw broke off while eating. The tooth was treated three years ago due to caries complications.
General condition: bad habits – smokes; concomitant diseases – no; hepatitis, tuberculosis, syphilis, HIV – denies; allergy history - not burdened, anesthesia was previously carried out, effective, without pathologies.
External examination: skin color – clear; face – symmetrical; face type – conical; the height of the lower third of the face is not changed; the chin does not protrude; lips close without tension; nasolabial and chin folds are moderately pronounced; mouth opening – free, painless; movements of the lower jaw are smooth, there are no displacements during movement.
Examination of the TMJ: the presence of crunching, clicking, noise in the TMJ during movement of the lower jaw is not recorded, the masticatory muscles are painless on palpation, the submandibular lymph nodes are painless on palpation and are not enlarged.
Objective data:
| P | R | P | P | ||||||||||||
| 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| P | P | P |
Examination of the oral mucosa: the mucous membrane is pale pink, moderate humidity, gingival papillae are normal.
Examination of teeth and dentition:
- intact teeth without pathology, not mobile, percussion and probing are painless, temperature reaction is negative, periodontal pockets are 0.1 mm.
- The fillings are in satisfactory condition, correspond to the bite, the marginal fit is tight.
The teeth are not mobile, percussion probing is painless, the temperature reaction is negative. IROPZ 16; 25; 26; 36; 44; 45 – 0.5.
Type of bite: fixed, straight.
Condition of the dentition: the shape of the dentition is ellipsoidal in the upper jaw, parabolic in the lower jaw. There are no secondary deformations.
Tongue: normal size, oval shape, normal frenulum.
Additional examination methods: from 07/05/2010. On an intraoral radiograph, there are 21 teeth in the periapical tissues without pathological changes, the canal is sealed to the physiological aperx, along its entire length.
or according to I.M. Oksman
| teeth | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Total |
| V/H | 1 | 1 | 2 | 3 | 3 | 6 | 5 | 4 | 25% |
| LF | 2 | 1 | 2 | 3 | 3 | 6 | 5 | 3 | 25% |
Loss of chewing efficiency – 3% according to I.M. Oksman.
Diagnosis – defect of hard dental tissues as a result of caries, destruction of crown 21 on 1/2 of the surface, IROPD 16; 25; 26; 36; 44; 45 – 0.5; loss of chewing efficiency 3% according to I.M. Oksman.
Plan for preparing the oral cavity for prosthetics: not carried out.
Orthopedic treatment plan: stump pin design for 21 teeth; single metal-ceramic crown for 21 teeth.
Diary:
| date | Volume of work performed | Manager's signature |
| 5.07.2010 | Inspection, documentation. Preparation of the root of the 21st tooth for a core post structure, modeling the post structure in the oral cavity with Lavax wax, applying a temporary filling - dentin paste. | |
| 6.07.2010 | Checking and fitting the metal stump pin structure to the root of the 21st tooth. Honey. treatment of the root and canal of the 21st tooth with 3% hydrogen peroxide and liquid for degreasing the canals, air; metal stump pin structure - 95% alcohol, air. Fixation of a metal stump pin structure into the root of the 21st tooth on a Fuji. | |
| 7.07.2010 | Under application anesthesia with Ludoxor spray, insertion of a retraction thread into the periodontal sulcus of the 21st tooth, preparation of the 21st tooth for a metal-ceramic crown. Taking a double impression from the upper jaw “Spidex”, from the lower jaw – an alginate impression “Hydrogum soft”. | |
| 8.07.2010 | Determination and fixation of central occlusion. | |
| 10.07.2010 | Checking and fitting the cast frame of a metal-ceramic crown for 21 teeth. Determination of the color of ceramic cladding: Ivoclar – 4 A. | |
| 12.07.2010 | Checking and fitting a metal-ceramic crown for 21 teeth. Honey. treatment of the stump of 21 teeth with 3% hydrogen peroxide and air; metal-ceramic crown - 95% alcohol, air. Fixation of a metal-ceramic crown for 21 teeth on “Fuji”. Advice and recommendations on oral care and denture care are given. |
Dispensary observation: the patient does not need a preventive examination of the oral cavity once every six months.
Epicrisis: as a result of orthopedic treatment of a defect in the hard tissues of the 21st tooth, the anatomical shape, aesthetics, integrity of the dentition of the upper jaw, and chewing efficiency were restored in full (100%).
Patient V.P. Ivanov, born in 1991, was given the necessary recommendations for caring for the oral cavity and the metal-ceramic crown on the 21st tooth.
Some features of the medical record
The material and type of medical record of a dental patient does not matter much.
It can be produced in a clinical setting or by printing and, as a rule, is an A5 notebook. The main requirement is that it be in paper form and have records in the form approved by law. The passport part is prepared by a medical registrar, clinic administrator or nurse. All other entries in the medical record are made only by the doctor, legibly, without corrections (a printed (computerized) option for making entries is possible), using only generally accepted abbreviations. The formulations of diagnoses, anatomical formations, names of instruments and medications are indicated in full, without abbreviations, taking into account the officially used terminology. The entry made is confirmed by the signature and personal seal of the doctor.
In addition to the records, the following must be included (pasted) in the medical record:
- test results (if any) - originals or copies;
- extracts from other medical institutions where dental care was provided, especially if the provision of dental care in other institutions occurred after the patient first applied (began to be observed) in this dental clinic;
- medical reports, expert opinions, consultations received in connection with the diseases for which the patient is observed in this clinic; medical reports, expert opinions, consultations received in connection with other diseases, the course of which may affect the characteristics of the dental disease;
- information on cancer examinations (based on the order of the Ministry of Health of the Russian Federation “On measures to improve the organization of cancer care for the population of the Russian Federation” No. 270 dated September 12, 1997);
- information on radiation doses received by the patient during X-ray examinations (based on the order of the Ministry of Health of the Russian Federation “On the introduction of state statistical monitoring of radiation doses of personnel and the population” No. 466 of December 31, 1999);
- X-rays of the patient’s teeth and maxillofacial area, taken in this dental clinic.
Let's take a closer look at the last point. Of the entire evidence base that is used by the parties when considering consumer claims in court in connection with the quality of services provided, X-ray images are of the greatest importance. Why? As an example, let’s look at a controversial situation that arises most often.
The patient had his teeth treated in several clinics and collected his x-rays from everywhere after the treatment was completed. At the same time, of course, in all clinics there were certain documents confirming the fact of treatment (service agreements, entries in the medical record, payment receipts, checks, etc.). In one of the clinics, an instrument broke off in a tooth canal during treatment. However, the patient sued not the clinic where the instrument was broken, but the richest of those where he was treated.
At the same time, it is almost impossible to prove the absence of fault of the clinic specified in the claim if the clinic cannot present an x-ray taken after completion of treatment. That is why the clinic is extremely interested in keeping all the images taken on the patient. However, certain legal difficulties arise here.
The fact is that radiography is usually included by clinics in the price list as a separate type of service. And on the basis of the Civil Code of the Russian Federation and the Law “On the Protection of Consumer Rights”, the patient has the right to regard the x-ray performed as a service paid for by him, the material expression (result) of which is an x-ray. Accordingly, the patient acquires the full right to take this image for himself.
Of course, this situation does not suit the clinic at all. Therefore, the clinic usually uses the following exit options:
- include in the Contract for the provision of dental services a clause according to which x-rays taken in the clinic are an integral part of the medical record of the dental patient. In this case, all images taken at the clinic remain its property on the basis of an agreement concluded with the patient.
- They give the patient not the image itself, but its image on paper or other media - for example, a copy from a visiograph, or a printout of a scanned image.
However, all of the above applies to the medical record of a dental patient, form No. 043/u. If a dental clinic uses its own form of medical records, then it may face serious problems in court proceedings. The fact is that the patient can submit a request for the clinic to provide evidence of a medical record of a dental patient in the form established by law (form No. 043/u).
In this case, the provision of a medical card of a different form by the dental clinic may be interpreted by the court as a formal basis for recognizing this form as not meeting the requirements of the law, and on this basis the card may not be accepted as written evidence. And this will allow you to ignore all the entries made in the card and give the patient grounds to accuse the clinic of improper record keeping.
Since this form of card is truly outdated and does not fully reflect both changes in civil legislation and new diagnostic and treatment standards, its certain modernization becomes inevitable. Therefore, in dentistry, as a way out of this situation, they use a loose leaf for the medical record (information sheet), taking into account the specific features of a particular clinic. It is much worse for a dental clinic if the dental patient’s medical record is not maintained at all.
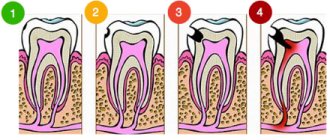
2).Deep caries:
Complaints: the presence of a carious cavity, food ingress, short-term pain from cold in ..... (tooth formula).
Objectively: on….(name) surface…(tooth formula) there is a carious cavity,…..according to Black, filled with softened dentin. Probing is slightly painful along the entire bottom of the carious cavity. Short-term pain from temperature stimuli. Percussion is negative.
R.V.G.
Treatment: Under topical anesthesia (.... (name)) and
Infiltration (conduction) anesthesia (….. (name)) is formed
and the cavity was treated with medication. Medical pad.. (name).
Insulating gasket…. (Name). (description of the manipulations performed - filling, restoration, inlay, etc., with the name of the material and an indication of the color). Sanding,
polishing
FAQ -
- Who makes entries in the medical record? The passport part is filled out by the registrar, administrator or nurse; all other entries are made only by the doctor.
- How are entries entered into the medical record? Legibly, using only generally accepted abbreviations, without corrections, handwritten or printed, certified by signature and the doctor’s personal seal.
- Why do you need a medical card? To reasonably protect the interests of the dental clinic, first of all, in court.
- Can dentistry issue a medical card to a patient? Formally yes, in fact no.
- What problems can there be for using the wrong card options? An incorrect version of the map may not be recognized by the court as written evidence, and the resulting lack of documentation required by law may become the reason for legal claims.
- Does the patient have the right to collect x-rays? Yes, at least copies of photographs on paper or other media.
- How do dentists update medical records? Use the medical record insert – information sheet.
The procedure for obtaining a medical card for an outpatient patient
The article discusses the basic requirements for drawing up a medical card for an outpatient, and responsibility for filling it out incorrectly.
Legal regulation
1. Federal Law of November 21, 2011 N 323-FZ “On the fundamentals of protecting the health of citizens in the Russian Federation”;
2. Order of the Ministry of Health of Russia dated December 15, 2014 N 834n (as amended on January 9, 2018) “On approval of unified forms of medical documentation used in medical organizations providing medical care in outpatient settings, and procedures for filling them out.”
Paragraph 11 of Article 79 of the Federal Law of November 21, 2011 N 323-FZ “On the fundamentals of protecting the health of citizens in the Russian Federation” (hereinafter referred to as Federal Law No. 323-FZ) establishes a general requirement for the obligation of medical organizations to maintain medical documentation in the prescribed manner and submit reports on types, forms, within the time frame and to the extent established by the authorized federal executive body.
The form, procedure for registration and maintenance of a medical record when providing outpatient care are provided for by Order of the Ministry of Health of Russia No. 834n dated December 15, 2014 “On approval of unified forms of medical documentation used in medical organizations providing medical care in outpatient settings, and procedures for filling them out” (hereinafter referred to as Order No. 834n).
Meaning of a patient's medical record
Registration form N 025/у “Medical record of a patient receiving medical care on an outpatient basis” (hereinafter referred to as the card) is the main registration medical document of a medical organization (other organization) providing medical care on an outpatient basis (hereinafter referred to as a medical organization). The card is filled out for each patient who seeks medical care in an outpatient setting for the first time.
It should be noted that cards are not maintained for patients receiving treatment in the following profiles: oncology, phthisiology, psychiatry, psychiatry-narcology, dermatology, dentistry and orthodontics - for these profiles, medical workers fill out their registration forms.
Who fills out the card?
According to paragraph 4 of Order No. 384, the card is filled out by doctors. Medical workers with secondary vocational education who conduct independent appointments fill out a logbook for patients receiving medical care on an outpatient basis.
The immediate procedure for receiving a doctor of a particular specialty is regulated by Orders of the Ministry of Health of the Russian Federation on approval of procedures for the provision of medical care in a particular profile (direction) or a specific disease (group of diseases).
So, for example, in accordance with paragraph 4 of the Order of the Ministry of Health and Social Development of the Russian Federation dated April 18, 2012 N 381n “On approval of the Procedure for providing medical care to the population in the field of cosmetology,” medical care in the field of cosmetology is provided by a cosmetologist. Nursing staff can provide medical services and manipulations as prescribed by a cosmetologist.
Consequently, filling out the medical card is carried out only by the doctor who is conducting the appointment.
It should also be noted that the card is filled out directly at the doctor’s appointment. The information that a doctor can fill out a card within 2 weeks after an appointment or within a month, distributed in some sources, is not true.
In what form is the map maintained?
The card is issued in paper form, and can also be issued in the form of an electronic document signed using an enhanced qualified electronic signature of a doctor, in accordance with the procedure for organizing a document flow system in the field of health care in terms of maintaining medical records in the form of electronic documents, approved by the Ministry of Health of the Russian Federation Federation in accordance with paragraph 11 of part 2 of article 14 of the Federal Law of November 21, 2011 N 323-FZ “On the fundamentals of protecting the health of citizens in the Russian Federation”.
How long should you keep your medical record?
A medical record is stored for 25 years; more information about the storage periods for medical records can be found here.
What items are provided on the card to fill out?
The card is filled out for each patient visit. The map is maintained by filling out the appropriate sections.
The title page of the card is filled out at the registry of a medical organization when the patient first seeks medical help. The title page of the card contains the full name of the medical organization in accordance with its constituent documents, the OGRN code, and the card number is indicated - the individual Card registration number established by the medical organization.
The card reflects the nature of the course of the disease (injury, poisoning), as well as all diagnostic and therapeutic measures carried out by the attending physician, recorded in their chronological sequence.
Entries are made in Russian, accurately, without abbreviations, all necessary corrections in the card are made immediately, confirmed by the signature of the doctor filling out the card. It is allowed to record the names of medicinal products in Latin.
The card contains only 35 points that need to be filled out. In particular, the card contains the information contained in the patient’s identity document, the series and number of the compulsory health insurance policy, the insurance number of the individual personal account (SNILS), the name of the medical insurance organization, information about marital status, education, place work and position, blood type and Rh factor, final (updated) diagnoses established for the first time or again, information about hospitalizations and surgical interventions.
When providing medical care and filling out medical documentation, it is necessary to remember that the criterion for the quality of medical care is the use of registered medicines and medical devices in accordance with the instructions for use.
What liability is provided for incorrectly filling out the card?
According to clause 1, part 2, art. 73 Federal Law No. 323-FZ, medical workers must provide medical care in accordance with their job descriptions, qualifications, and job responsibilities.
If the card is filled out incorrectly, the medical worker may be subject to disciplinary action for failure to perform or improper performance of official duties through his own fault in accordance with Article 192 of the Labor Code of the Russian Federation.
The correctness of filling out a medical record is one of the criteria for assessing the quality of medical care under an agreement on paid provision of medical services in accordance with Order of the Ministry of Health of the Russian Federation dated May 10, 2022 No. 203n “On approval of criteria for assessing the quality of medical care.” A medical organization that has compensated a patient for harm caused by the actions of a medical worker may subsequently, by way of recourse, bring the medical worker to civil liability in accordance with Article 1081 of the Civil Code of the Russian Federation.
Criminal liability of medical workers cannot be excluded if they enter knowingly false information into medical documents out of selfish interest. Thus, by verdict No. 1-11/2016 1-388/2015 of August 19, 2016 in case No. 1-11/2016 of the Leninsky District Court of Komsomolsk-on-Amur, a medical worker was found guilty of entering knowingly false information into medical records guilty of committing a crime under Part 1 of Art. 292 of the Criminal Code of the Russian Federation.
Finally, it is necessary to understand that when conducting an examination within the framework of a criminal case, medical documentation is also examined (and in some cases, exclusively) and its incorrect completion may indicate inadequate quality of medical care provided, which may lead to criminal liability under Art. 238 of the Criminal Code of the Russian Federation, while in order to be held accountable under this article, the occurrence of adverse consequences in the form of death or harm to the patient’s health is not necessary.