{jcomments on}Treatment of victims with jaw fractures consists of repositioning and immobilization of jaw fragments, as well as drug treatment and physical therapy. Reposition involves aligning or moving facial bone fragments into the correct position. If it is not possible to compare the displaced fragments at once, they are reduced gradually, over several days, using elastic traction. Immobilization means securing the fragments in the correct position for the period necessary for their fusion (consolidation), i.e. until callus formation. On average, this period is 4-5 weeks for uncomplicated healing of a fracture of the upper jaw and a unilateral fracture of the lower jaw. With a bilateral fracture of the lower jaw, the immobilization period can increase to 5-6 weeks. Drug and physical treatment are necessary to prevent the development of complications during the period of consolidation of fragments (antibacterial, anti-inflammatory, antihistamines; medications that improve the rheological properties of blood and tissue microcirculation, immunostimulants, drugs that optimize osteogenesis). In addition, the question of the advisability of preserving teeth in the fracture gap and the need for therapeutic measures in relation to these teeth must be resolved.
Types of conservative methods of immobilization of jaw fragments
There are temporary methods of immobilization (including transport) and permanent (therapeutic). Temporary methods for securing jaw fragments are divided into: - extraoral (bandage, chin sling, improvised bandages using improvised means); — intraoral (methods of intermaxillary ligature fastening, splints-spoons with “mustaches” of different designs). Permanent (therapeutic) methods of immobilization are divided into : - non-laboratory splints (individual dental splints made of metal or other material, standard dental splints); — laboratory-made splints (Weber’s supragingival splint, simple or with an inclined plane, Vankevich and Vankevich-Stepanova splints, various dental aligners, Port’s supragingival splint).
Temporary (transport) immobilization
Indications for imposing temporary (transport) immobilization: - lack of conditions for permanent (therapeutic) immobilization and the need to transport the victim to a specialized medical institution; — lack of specialized personnel who can carry out permanent immobilization; - lack of time required for permanent (therapeutic) immobilization. This usually happens during combat operations or other emergency situations (earthquake, accidents with a large number of casualties, etc.), when a large flow of victims and wounded with trauma is simultaneously observed; - severe general somatic condition (traumatic shock, coma, intracranial hematoma, etc.), which is a temporary relative contraindication for therapeutic immobilization. Temporary immobilization is imposed for a period of no more than 3-4 days (the maximum time required to transport victims to a specialized institution or call a specialist to the patient), since with its help it is impossible to achieve the required long-term immobility of fragments. In exceptional cases, this period is extended due to the severe general condition of the patient, in which therapeutic immobilization is temporarily contraindicated. Temporary immobilization can be performed both outside a medical institution and in a specialized clinic. If it is imposed while the victim is being transported to a medical facility, it is called “transport”. Typically, temporary immobilization is applied by junior or nursing staff, as well as in the form of self- or mutual assistance. Some methods are performed only by specialists (intermaxillary ligature fastening).
Extraoral methods of temporary (transport) immobilization.
— A simple bandage parietal-chin bandage . It is applied for fractures of the upper and lower jaw. A wide gauze bandage is used, circular tours of which are carried out through the chin and parietal bones. You can use improvised material: a headscarf, scarf, etc., which is less convenient. A simple bandage does not stay firmly on the head and must be adjusted frequently. — The parietal-chin bandage according to Hippocrates is securely fixed on the head and does not require correction. Used for fractures of the upper and lower jaw.
Parietomental bandage according to Hippocrates
— Standard soft chin sling by Pomerantseva-Urbanskaya. Used for fractures of the upper jaw and lower jaw. It consists of a chin sling, to which wide elastic bands are sewn on both sides, turning into fabric ribbons with holes for a lace. The sling is convenient and versatile, but is not used for fractures of toothless jaws and the absence of dentures.
Standard soft chin sling Pomerantseva-Urbanskaya
— Standard bandage for transport immobilization (rigid chin sling) for fractures of the lower and upper jaw. This bandage consists of a standard dimensionless cap and a rigid chin sling with slots and protrusions used to fix rubber rings and the victim’s tongue, as well as to drain wound contents. Intraoral methods of temporary (transport) immobilization.
Standard bandage for transport immobilization
— Standard transport splint for immobilization of the upper jaw . Consists of a standard cap and a standard metal spoon splint with extraoral rods (“whiskers”) firmly fixed to the spoon splint. — Intermaxillary ligature fastening . It is used most often in clinical practice. For immobilization, wire ligatures are used, which should be easy to bend, not oxidize and be inexpensive. Bronze-aluminum wire with a diameter of 0.5-0.6 mm meets this requirement. To apply an intermaxillary ligature fastening, take pieces of bronze-aluminum wire 7-10 cm long and tools (crampon forceps, Billroth-type hemostatic clamps, scissors for cutting metal wire, anatomical tweezers). Indications for the application of intermaxillary ligature fastening are to prevent displacement of fragments and eliminate intra-wound trauma during the transportation of the victim and during his examination, until the moment of therapeutic immobilization. General rules observed when applying intermaxillary ligature fastening: immobilization is carried out under local anesthesia, tartar is first removed, mobile teeth and teeth located in the fracture gap are not used for intermaxillary ligature fastening, stable antagonist teeth are used, wire ligatures are twisted clockwise. There are a large number of different methods of intermaxillary ligature fastening of jaw fragments.
Feature of the technique
There are several methods for applying wire ligatures according to Ivey, Geikin and others. However, immobilization of jaw fragments using splints is considered a more rational method compared to ligature binding, which is only a temporary procedure and is combined with the application of a chin sling. The Tigerstedt fixation method is considered universal, since it is used for almost all jaw bone fractures. For production, aluminum wire with a cross section of up to 2.0 millimeters is used.
The natural softness of aluminum allows structures to be made by hand. It does not require complex instrumentation, so the fixator can be customized for each patient and used in any setting.
This technique was modernized by domestic scientists A.A. Limberg and A.E. Rauer.
Methods of intermaxillary ligature fastening.
— Silverman . A bronze-aluminum ligature is drawn around each of the two adjacent teeth and twisted, then the ends of these two ligatures are also twisted. The same is done in the area of antagonist teeth. The upper wire flagellum is twisted with the lower one, and the end is cut off. Advantages: ease of manufacture. Disadvantages: after twisting the ligatures, thick wire flagella are formed in the vestibule of the mouth, injuring the mucous membrane; if necessary, open the patient’s mouth and cut the thick wire flagella, which is quite difficult. After examining the oral cavity, the structure has to be redone.
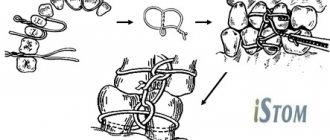
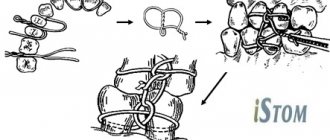
— Intermaxillary ligature fastening using the Ivey method.
Intermaxillary ligature fastening using the Ivey method
It is most often used in clinical practice, usually in all cases of jaw fractures. In case of a fracture of the upper jaw, the intermaxillary ligature fastening is supplemented with the application of a chin sling to prevent its displacement downward when the lower jaw involuntarily drops. Advantages: simplicity and efficiency, the ability to quickly open the mouth if necessary, without compromising the integrity of the structure. Intermaxillary ligature fastening according to Kazanyan is less convenient compared to the Ivey method. The technique differs in that a figure-of-eight ligature is placed around the adjacent teeth of one fragment and its two ends are twisted in the vestibule of the mouth. The same manipulation is carried out on the antagonist teeth and on the teeth of the other fragment. The free ends are twisted and trimmed. Thus, the common end of the wire (flagellum) consists of four ends. The disadvantages of the method are the presence of a thick wire harness in the vestibule of the mouth, which can injure the mucous membrane, as well as the need to re-apply ligatures if they break or after emergency cutting of the ligatures.
— Intermaxillary ligature fastening according to Gotsko.
A polyamide thread is used as a ligature. It is passed around the neck of the tooth and tied with a knot on its vestibular surface. Next, both ends of the thread are passed through the interdental space of the antagonist teeth from the vestibule - into the oral cavity, then each end is taken out of the cavity into the vestibule of the mouth (distal and medial), pulled up and tied together with a knot, immobilizing. Advantage : low trauma, high efficiency.
Intermaxillary ligature fastening using the Gotsko method
How to remove splints after a jaw fracture?
The decision to remove splints from the jaws is made only by the attending physician. To determine whether the damaged bones have recovered, X-rays must be taken. They allow you to accurately assess the patient’s condition and understand whether he still needs fixation structures.
Condition of the oral cavity before removing splints from the jaw after a fracture
Removing splints from the jaw after a fracture is a separate issue that worries patients. The procedure cannot cause any difficulties for an experienced specialist. Typically, patients want to know whether it hurts to remove splints after a jaw fracture. Although people have different pain thresholds, most who have undergone this procedure agree that it does not cause significant discomfort.
Difficulties usually arise later. It takes time to get used to the lack of a support mechanism. In addition, at first the muscles are weakened. Particular attention should be paid to nutrition.
Therapeutic (permanent) immobilization using non-laboratory dental splints
Individual dental wire splints by Tigerstedt. Types of Tigerstedt dental splints: - smooth splint-bracket; — bus-bracket with a spacer bend; - tire with hook loops.
The splints are made of aluminum wire d=1.8-2.0 mm and 12-15 cm long. They are tied to the teeth using bronze-aluminum wire d=0.5-0.6 mm. The splint is bent individually for each patient using crampon forceps. General rules for applying dental splints . 0.5 ml of a 0.1% atropine solution is injected subcutaneously to reduce salivation, splinting is carried out under local anesthesia, it is necessary to remove tartar to freely pass the ligature into the interdental space, bend the splint from the side of the fracture, try it on the teeth in the mouth, and bend it outside the oral cavity, the splint should be adjacent to the neck of each tooth at least at one point, the splint is tied to each tooth with a ligature wire, which is twisted clockwise. The production of the splint begins with bending a large hook that clasps the first tooth, or a hook spike inserted into the interdental space. To try on a splint, it is applied to the teeth in the mouth.
Smooth splint.
It is used to treat fractures of the lower jaw, provided that the larger fragment contains at least four, and the smaller fragment contains at least two stable teeth.
Smooth splint
Indications for use : linear fractures of the lower jaw, located within the dentition, without displacement or with easily reducible fragments, fractures of the alveolar process, fractures and dislocations of teeth, tooth mobility in acute odontogenic osteomyelitis and periodontitis, fractures of the upper jaw (Adams and Dingman methods), to prevent pathological fracture of the lower jaw. After treatment, before removing the splint, loosen the ligatures and check the lack of mobility of the fragments by rocking them. The splint is removed after 4-5 weeks. The patient needs to take liquid food. The doctor should regularly examine the patient 2-3 times a week. In this case, it is necessary to monitor the state of the bite, the strength of fixation of the fragments, the condition of the tissues and teeth in the fracture gap. When the fixation of the splint on the teeth becomes loose, it is necessary to tighten the ligatures by twisting them. If the ligature bursts, it is replaced with a new one. The patient is taught hygienic measures to prevent the development of gingivitis. For this purpose, the patient should brush his teeth and splint with toothpaste and a brush 2 times a day, after each meal, remove food debris with a toothpick, and rinse his mouth with antiseptic solutions 3-5 times a day.
Busbar with spacer bend.
The spacer bend prevents lateral displacement of fragments.
Busbar with spacer bend
Indications for use : fracture of the lower jaw within the dentition and the presence of a bone tissue defect of no more than 2-4 cm, fracture of the lower jaw without displacement or with easily reducible fragments, if the fracture gap passes through the alveolar part, devoid of teeth.
Tire with hook loops.
The splint is most often used to treat jaw fractures. Two splints with hooking loops are made for the teeth of the upper and lower jaw.
Tire with hook loops
Indications for use : fractures of the lower jaw outside the dentition, within the dentition - in the absence of four stable teeth on the larger fragment and two stable teeth on the smaller one, fractures of the lower jaw with difficult-to-reduce fragments requiring traction, bilateral, double and multiple fractures of the lower jaw, fracture of the upper jaw (with the obligatory use of a chin sling), simultaneous fractures of the upper and lower jaw. When making a splint, its hook loop should be at an angle of 45° relative to the gum. The towing loops are bent on the tire so that they are located in the area of the 6th, 4th and 2nd teeth. If the patient does not have these teeth, then hooking loops are made in the area of other teeth that have antagonists. Usually, 3-4 hook loops are bent on the splint adjacent to the teeth of the larger fragment, and 2-3 hook loops on the smaller one. The base of the loop must be within the crown of the tooth. If the displacement of the fragments is large and it is difficult to bend one splint onto both fragments, splints can be made and secured to each of the fragments. After their reposition, rubber rings are put on the hook loops at an angle so that they create compression of the fragments, which significantly prevents their movement. Periodically (2-3 times a week) the patient is examined, ligatures are tightened, rubber rings are changed, the vestibule of the mouth is treated with antiseptic solutions, and the condition of the bite is monitored. 10-25 days after applying the splint, an X-ray examination is performed to monitor the position of the fragments. After fusion of the fragments, before removing the splints, it is necessary to remove the rubber rings and allow the patient to walk for 1-2 days without fixation, eating soft food. If the fragments do not move, the splints are removed. If there is a slight change in the bite, the rubber traction is retained for another 10-15 days.
Splinting using the A.P. method Vikhrov and M.A. Slepchenko.
The authors proposed using a polyamide thread to strengthen the attachment of the splint to the teeth. To do this, take a bronze-aluminum wire ligature, fold it in the form of a hairpin and insert both of its ends into one interdental space from the mouth towards the vestibule of the mouth. The ligature is tightened so that a small loop is formed on the lingual surface of the interdental spaces. A similar procedure is performed in the area of all interdental spaces. Take a polyamide thread with a diameter of 1 mm and pass it through all the loops on the lingual side, the ends of the thread are brought out into the vestibule of the mouth behind the last teeth on both sides. Next, a previously made splint is placed on the teeth so that it is located between the two ends of the same previously made bronze-aluminum ligatures, which are then twisted. According to the authors, the advantages of their method are the following: stronger fastening of fragments, reduction of splint fastening time, and absence of trauma to the gum mucosa.
Splinting using the Vikhrov-Slepchenko method
Tooth standard splints.
Good manual skills are required to make custom wire splints. Their production requires a lot of time and frequent fitting to the dental arch. It is especially difficult to bend them in case of malocclusion, dental dystopia, etc. Taking into account the above, standard splints were proposed, which are manufactured in the factory, do not require bending of the hook loops and simplify splinting. In Russia, standard belt tires were proposed by V.S. Vasilyev. The tire is made of a thin flat metal strip 2.3 mm wide and 134 mm long, which has 14 hooking loops. The tire bends easily in the horizontal plane, but does not bend in the vertical plane. The Vasiliev splint is cut to the required size, bent along the dental arch so that it touches each tooth at least at one point, and tied to the teeth with ligature wire. The advantage of the splint is the speed of its application . The disadvantage is the impossibility of bending it in a vertical plane, which does not allow to avoid injury to the mucous membrane in the lateral parts of the jaws due to the discrepancy between the splint and the curve of Spee. This splint is not suitable for single-jaw splinting due to its low strength. Abroad, there are various designs of standard tires made of steel wire (Winter tires) and polyamide materials that can be bent in any plane. Tires are manufactured with pre-made hooks.
General rules and basic provisions when applying structures
The application of orthopedic structures, regardless of their type, occurs in compliance with the following rules:
- the manipulation is carried out after the administration of local anesthetics;
- to reduce saliva production, a subcutaneous injection of Atropine is performed;
- the structure begins to bend from the left side;
- the structure bends outside the oral cavity;
- according to medical agreement, the ligature wire is twisted only clockwise.
The main criteria that indicate that the orthopedic design is installed correctly:
- has a location on the neck;
- comes into contact with each tooth (at least at one point);
- repeats the outline of the dentition;
- does not spring;
- despite contact with the gingival papillae, they are not injured.
In recent years, practicing dentists in the treatment of fractures of the lower jaw bones have given preference to surgical methods rather than wire mobilization. This is due to the fact that the recovery process is shortened, and, as a result, the patient’s time in hospital is reduced.
Another advantage of surgical therapy is easier dental care. It is also important that the patient’s nutrition does not cause any particular difficulties.
Therapeutic immobilization of jaw fragments using laboratory-made splints
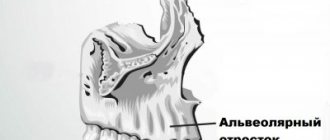
Laboratory-made splints are classified as orthopedic immobilization methods. They perform both an independent immobilization function and can be an additional device for various surgical methods of fastening fragments. Removable orthopedic structures include supragingival splints (simple or inclined plane Weber supragingival splint, Vankevich splint, Vankevich-Stepanov splint) and Porta supragingival splint. Non-removable orthopedic structures include dental splints with fixing elements of various modifications. Indications for the use of laboratory-made splints : - severe injuries of the jaws with significant defects of bone tissue, in which bone grafting of the jaw is not performed; — the presence of concomitant diseases in the victim (diabetes mellitus, stroke, etc.), in which the use of surgical immobilization methods is contraindicated; — the patient’s refusal to surgically fix the fragments; — the need for additional fixation of fragments simultaneously with the use of wire splints. To produce laboratory splints, the following conditions are required: a dental laboratory, special materials. Dental work is carried out by dental technicians.
Simple Weber dentogingival splint.
Can be used independently or as one of the main elements when using the surrounding suture method for fractures of the lower jaw. The Weber splint is used for significant defects of the lower jaw as a result of traumatic osteomyelitis or after resection of the lower jaw for a tumor. In these cases, long-term wearing of the splint (for 2-3 months) can lead to the elimination of pronounced lateral displacement of the lower jaw after removal of the splint. The Weber splint is prepared in the laboratory, after taking impressions of jaw fragments. To prevent lateral displacement of fragments, an inclined plane is made on it in the area of the molars. You can make a splint directly in the patient’s mouth from quick-hardening plastic.
Bus Vankevich and bus Vankevich-Stepanova.
They are dental splints supported on the alveolar process of the upper jaw and the hard palate. In the lateral sections it has two inclined planes facing downwards, which abut against the anterior edges of the branches or the alveolar part of the lateral sections of the body of the lower jaw, mainly from the lingual side and do not allow fragments of the lower jaw to move forward, upward and inward. The Vankevich splint is used to fix and prevent lateral and rotational displacement of fragments of the lower jaw, especially with significant defects, due to the emphasis of the inclined planes on the anterior edges of the branches of the jaw. The Vankevich splint as modified by Stepanov differs in that instead of a maxillary base there is a metal arch, like a clasp prosthesis. The Port splint is used in case of a fracture of the edentulous lower jaw without displacement of the fragments and the patient does not have removable dentures and teeth in the upper jaw. The splint consists of two base plates for each jaw, similar to complete removable dentures, rigidly connected to each other in the position of central occlusion. There is a hole in the front section of the tire for food intake. The Porta splint is used in combination with wearing a chin sling bandage.
Dental splints with fixing elements.
Used for immobilization of fragments of the lower jaw in the presence of a bone tissue defect within the dentition, when the fragments have a sufficient number of stable supporting teeth. These splints consist of metal caps fitted to the teeth of the lower jaw. The caps are soldered together and fixed on the teeth of each fragment. With the help of various locks (pins, levers, etc.), after their reposition, the fragments are secured for the period necessary for consolidation. The teeth used for splinting are not prepared.
Types of Tigerstedt tires
Practicing dentists use five types of jaw retainers using the Tigerstedt method.
Smooth splint
Used for a fracture of the lower jaw, if 4 teeth are preserved (on a large chip). Splinting with a smooth splint is performed in the following cases:
Fastening is done using aluminum wire. It is bent in an arc, engaging the wisdom tooth, after which each dental unit is covered. At the end of the manipulation, the ligatures (distal and medial ends) are twisted. The ends of the cut ligatures are placed in the spaces between the crowns.
This orthopedic product is removed after 5 weeks.
With spacer
A wire splint with a spacer is placed if the crowns in the area of injury are not preserved, and the fracture itself passes along the alveolar part. A special feature of this splint is the location of the spacer at the fracture site.
To prevent displacement, the edges of the bend are placed with emphasis on the adjacent teeth.
With hook loops
Tires with toe loops are produced at an angle of 90 or 45 degrees.
This method allows you to eliminate a fracture of the lower jaw with or without displacement. If the integrity of the upper jaw is compromised, it becomes necessary to wear a sling bandage.
Five or six loops are made on the tire, the length of which is from 3 to 4 mm. They are placed on even-numbered dental units. Rubber tubes are put on the hooks, which are changed every six days. Ligatures are tightened periodically at intervals of 2 days.
With inclined surface
A splint with an inclined surface is used if there is a need to prevent lateral displacement to the fracture site. The supporting inclined plane is provided by vertically installed hinges, which are twice the height of the molars.
With reference plane
An orthopedic product with a retaining (supporting) plane helps prevent sagging tissues and flaps of the hard palate. Therefore, when installing this type of product, there is a positive dynamics of the treatment process in case of traumatic damage to the bones of the upper jaw or after surgical therapy on it.