Myth: Braces cause tooth decay.
Of course, braces themselves do not cause caries. But they can create conditions for its development.
The main problem is the impossibility of complete oral hygiene, since braces are a complex system with many small elements and micro-gaps. Even using brushes or an irrigator, regular brushing of teeth and following a special diet does not guarantee one hundred percent removal of plaque. As a result, caries under braces develops very quickly, especially in places that are difficult to reach with a toothbrush.
Braces also complicate the process of self-cleaning of the oral cavity, which is why caries progresses quickly. Therefore, it is necessary to treat caries with braces immediately after it is identified, without waiting for the end of orthodontic treatment when the braces are removed.
A new method for preventing dental caries in patients with braces
Orthodontic treatment, despite the development of technology, is still accompanied by a significant risk of dental caries in children. Braces often become a mechanical obstacle to the natural self-cleaning of the oral cavity; long-term retention of microbial plaque leads to diffusion of acid through the interprismatic space of the enamel and dissociation of calcium and phosphates in the subsurface layer [1].
At the same time, the density of the enamel decreases and its solubility increases, which causes a change in its physicochemical properties and the appearance of a white carious spot - a focus of demineralization (Fig. 1).
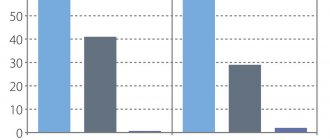
This process is reversible, and under favorable conditions, under the influence of a remineralizing liquid, calcium ions can reenter the crystal lattice, displacing hydrogen ions [3]. According to various authors who examined patients with fixed orthodontic appliances, 24.9-50% of patients were found to have foci of enamel demineralization [4, 12, 18]. The prevalence of pathology is directly dependent on the level of oral hygiene and the frequency of fluoride use. Farhadian N et al. (2007) noted a significant reduction (40%) in the depth of demineralization in a group of children undergoing orthodontic treatment when using fluoride-containing varnish. This is significantly more than in patients in the comparison group (P < 001) [6]. Fluoride varnishes may be considered for clinical use as an effective method to prevent or reduce demineralization during orthodontic treatment, especially in patients with poor oral hygiene [5]. The prevalence of pathology is directly dependent on the level of oral hygiene and the frequency of fluoride use. According to O' Reilly MT et al. (2013), Biscover LV material (Bisco) in patients with braces demonstrated a clinically small but statistically significant effect in preventing the appearance of whites stains on enamel [16]. A number of authors in vitro, using DIAGNOdent ® (KaVo) and a scanning electron microscope (SEM), analyzed the effectiveness of various drugs for the remineralization of enamel, on the surface of which foci of demineralization were artificially simulated. All three experimental groups showed a statistically significant effect compared to the control group. However, with the added benefit of fluoride content (NaF 0.2%), casein phosphopeptide amorphous calcium phosphate fluoride (CPP-ACPF) and tricalcium phosphate fluoride (TCP-F) showed a marginally greater degree of enamel remineralization than casein phosphopeptide amorphous calcium phosphate (CPP). -ACP) [14].
A number of authors, after 7 weeks of orthodontic treatment, observed the appearance of white spots on the enamel around braces. Lesion volume, which was studied using microcomputed tomography, ranged from 0 to 1.2931 mm (3) and was significantly correlated with color intensity [15]. Twetman S. et al. (1997), Torlakovic L. et al. (2012) diagnosed a statistically significant decrease in the number of white spots and an increase in the degree of enamel mineralization around brackets when fixed with glass ionomer cement compared to the use of composite materials (p < 0.05 ) [19, 21]. Koji Kawasaki, Masaki Kambara (2014) investigated the process of enamel demineralization and the remineralizing properties of filling materials using the induced fluorescence and electron probe method (EPMA). The ion concentration was measured using inductively coupled plasma and ion electrode atomic emission spectrometry (ICP). Filling materials containing and not containing glass ionomer filler were compared. As a result of research, it was found that only materials containing glass ionomer filler prevent demineralization of enamel [10].
In connection with the above, there is no doubt that the issues of prevention and treatment of initial forms of caries in children undergoing orthodontic treatment using braces are relevant. Analyzing the existing methods of remineralization therapy (the use of calcium-phosphorus gels, fluoride-containing varnishes and gels, deep fluoridation, electrophoresis or applications of 10% calcium gluconate and 2% sodium fluoride), we have to admit that they are imperfect [7— 9, 11, 13, 20]. A long course of treatment requires a lot of time for the dentist and the patient, and the effectiveness is not always high [17].
Our attention was drawn to a new dental material that has the property of releasing fluoride for long-term tooth protection. One of the indications for its use is the protection of caries-prone areas around the site of fixation of orthodontic structures. Clinpro™ XT Varnish (3M ESPE) is a light-curing, modified glass ionomer cement designed to coat enamel and dentin in specific areas of the tooth. The material has a prolonged effect due to the release of fluoride and remains on the surface of the teeth for up to 6 months or more. Available in clicker form (liquid-paste system), which ensures accurate dosing and easy mixing. The paste contains radiopaque fluoroaluminosilicate glass, and the liquid consists primarily of polyalkenic acid (2-hydroxyethyl methacrylate) (HEMA), water, initiators (including camphoroquinone) and calcium glycerophosphate. Fluorine is contained in particles of fluoroalumosilicate glass. The reaction occurring at the interface between the material and the hard tissues of the tooth leads to the immediate release of fluoride, while the rest of the material layer serves as a fluoride reservoir. Clinpro™ XT Varnish also contains calcium glycerophosphate, which releases calcium and phosphates, which have a positive effect on mineral metabolism in the oral cavity. Calcium glycerophosphate in the composition ensures the release of calcium and phosphates for six months. Thus, Clinpro™ XT Varnish material combines the advantages of glass ionomer cements: adhesion to tooth tissue and long-term fluoride release, and also has the additional advantage of calcium and phosphate release.
Clinpro™ XT Varnish is designed to:
- for the treatment of hypersensitivity when the dentin of the tooth root is exposed due to gum recession;
- to protect newly erupted teeth, caries-prone areas (including around orthodontic appliances), including chalky spots without signs of caries or cavities.
Not intended for use under braces; for use instead of traditional sealants that remain in the tooth cavity for a long time; for patients with dry mucous membranes (for example, due to mouth breathing) and is not used as a filling material for restoring hard dental tissues.
To study the properties of the material, we used data from the technical description of the 3M product [2]. In vitro studies have shown that the coating will remain on the tooth surface and resist mechanical stress during tooth brushing for at least 6 months. The transverse tensile strength and compressive strength of Clinpro™ XT Varnish and other glass ionomer cements are statistically virtually identical. The adhesion force with open dentinal tubules was 6.44, with unprepared enamel - 17.8 (2.4), and with the smear layer - 9.42 (1.69). It was found that at 24 hours, the total fluoride release of Clinpro™ XT Varnish was higher than that of a traditional sodium fluoride varnish, and after 24 hours, the amount of fluoride and calcium released was higher than that of another brand of glass ionomer cement. Interestingly, Clinpro™ XT Varnish has a so-called battery effect that lasts for 4.5 hours after brushing your teeth or using a fluoride rinse. A number of authors used scanning electron microscopy to study the properties of this material. Studies have shown that Clinpro™ XT Varnish reduces dentin permeability to approximately the same extent as a non-fluoride-releasing adhesive and also penetrates and occludes dentinal tubules. Clinpro™ XT Varnish creates a barrier on the tooth surface that resists demineralization and inhibits the formation of chalk stains directly under and around the cementum.
Clinical case
Patient R., 12 years old. He is undergoing orthodontic treatment using a brace system. KPU = 5, OHI-S = 2.3, low degree of susceptibility to caries according to RM Grainder, G. Nikiforuk (1960). Occlusion: crossbite on the right, tortoanomaly of teeth 12, 22, crowding of teeth in the anterior part of the lower jaw. The mucous membrane of the gums is pale pink and moist. The attachment of the frenulum of the tongue and lips is normal (Fig. 2). The plaque on the teeth was stained with a dye; the level of hygiene was poor (Fig. 3).
After training in oral hygiene and professional hygiene (Fig. 4), 37% phosphoric acid gel was applied around the braces on teeth 11, 21, 22 according to the instructions for use of the Clinpro™ XT Varnish (3M ESPE) material for 15 seconds (Fig. 5), then the conditioner was washed off with distilled water and the teeth were carefully dried with air (Fig. 7). Clinpro™ XT Varnish was mixed for 5 seconds (working time 2.5 minutes) and applied around the brackets to the enamel of teeth 11, 21, 22 using a brush (Figure 7). Photopolymerization of glass ionomer cement was carried out (20 seconds) (Fig. 8). Figure 9 shows the final stage of treatment using Clinpro™ XT Varnish (3M ESPE). The patient and her parents were trained in the standard method of brushing teeth, the use of floss for interdental hygiene, fluoride-containing rinse, and toothpastes with calcium and fluoride was recommended. The use of Clinpro™ XT Varnish (3M ESPE), which has the ability to release fluoride for a long time, to prevent dental caries in patients with braces is a simple and effective method. The advantage of this technique is the preservation of hybrid glass ionomer cement on the surface of the teeth, which for six months, thanks to the “battery effect,” releases fluorine, calcium and phosphate compounds into the hard tissues of the tooth and oral fluid, preventing the development of foci of enamel demineralization around braces.
Rice. 1. Multiple chalky spots in patient L., 15 years old, after orthodontic treatment using a brace system. Rice. 2. The condition of the oral cavity in patient R., 12 years old, undergoing orthodontic treatment using a brace system. Rice. 3. Determining the patient’s level of oral hygiene using a dye. Rice. 4. Condition after professional oral hygiene. Rice. 5. Applying conditioner (37% phosphoric acid gel) around the braces on teeth 11, 21, 22. Fig. 6. Teeth 11, 21, 22 after removing the conditioner. Rice. 7. Apply Clinpro™ XT Varnish (3M ESPE) fluoride-releasing dental material for long-term dental protection around brackets (teeth 11, 21, 22). Rice. 8. Photopolymerization of Clinpro™ XT Varnish material (3M ESPE). Rice. 9. Material Clinpro™ XT Varnish (3M ESPE) on teeth 11, 21, 22 after photopolymerization.
Literature
- Kiselnikova L. P., Ramm N. L., Bimbas E. S., Dashchenko E. A. Resistance of hard tissues according to the TER test and its correction in persons with CFA / Bulletin of the UGMA, vol.
2, Ekaterinburg, 1996, pp. 49-51. - Clinpro™ XT Varnish Fluoride Release Dental Material for Long-Term Teeth Protection (3M ESPE) - Product Data Sheet
(3M ESPE). – 19 p. - Dentistry for children.
Therapy ./Ed. V. M. Elizarova: Textbook. — M.: OJSC “Publishing House “Medicine”. – 2009. – 408 p. - Terekhova T. N., Naumovich D. N. Modern approaches to the prevention of major dental diseases during orthodontic treatment. // Modern dentistry.
- No. 4. - 2007. - P. 15-19. - Didem Nalbantgil, Mehmet Oguz Oztoprak, Derya Germec Cakan, Kemal Bozkurt, and Tulin Arun. Prevention of demineralization around orthodontic brackets using two different fluoride varnishes Eur J Dent.
Jan 2013; 7(1): 41-47. - Farhadian N, Miresmaeili A, Eslami B, Mehrabi S. Effect of fluoride varnish on enamel demineralization around brackets: an in-vivo study.
Am J Orthod Dentofacial Orthop. 2008 Apr; 133(4 Suppl): S95–8. - Hicks J, Wild T, Flaitz CM, Seybold S. Fluoride varnishes and caries development in primary tooth enamel: an in vitro study.
ASDC J Dent Child. 2001 Sep-Dec; 68 (5-6): 304—10, 300. - Hicks J, Garcia-Godoy F, Flaitz C. Biological factors in dental caries: role of remineralization and fluoride in the dynamic process of demineralization and remineralization (part 3).
J Clin Pediatr Dent. 2004 Spring; 28(3): 203–14. - Hicks J, Flaitz C. Role of remineralizing fluid in in vitro enamel caries formation and progression.
Quintessence Int. 2007 Apr; 38 (4): 313–9. - Koji Kawasaki* and Masaki Kambara.
Effects of Ion-Releasing Tooth-Coating Material on Demineralization of Bovine Tooth Enamel Int J Dent. 2014; 2014: 463149. Published online Jan 21, 2014.
A complete list of references is in the editorial office.
Caries during treatment with aligners
From the point of view of preventing and treating caries, mouthguards are more convenient than braces.
Oral hygiene with aligners is effective and simple: you remove the aligners, brush your teeth as usual, rinse the aligners themselves and put them back on. While braces retain food debris, aligners do not in any way prevent the teeth from being thoroughly cleaned. Accordingly, the risk of developing caries is less than with treatment with braces.
If caries does occur, treating teeth with aligners is also much more convenient. We said above that caries can be treated with braces, but sometimes you have to peel off the bracket or remove the arch. The aligners are simply removed, and the doctor gets full access to the teeth.
conclusions
Flash Free technology makes the doctor’s work and the patient’s life easier during and after treatment with braces. And it really protects the enamel around and under the bracket from acids and reduces the risk of developing caries. Despite all the obvious advantages, it cannot be called a panacea for all ills - without proper hygiene, careful care and without close supervision by a doctor, you cannot be sure of the result of orthodontic treatment.
- The number of bacteria in saliva is about 1-5 billion. And in the plaque that forms on the surface of the teeth, their number is many times greater - there are from 10 to 1000 billion cells.
- If you divide the process of installing braces into stages, then with the classical method there will be approximately 11 of them, and when installing braces with Flash Free technology there will be only 5.
- Delivery of braces with Flash Free backing installed on them is a definite problem. After all, you cannot allow the side of the brace with which it is attached to the tooth to touch other surfaces. To transport such braces, we had to make special packaging, which was tested in various tests.
If you want to have a healthy and beautiful smile, come to the Golden Section clinic. Our specialists are always happy to help you!
Where to treat caries with braces or aligners
We will not examine the question of how to treat caries under braces or with aligners: the technique remains at the discretion of the specialist and is unlikely to be useful to the patient. But the choice of clinic and doctor depends on you. The fact is that caries treatment must be carried out without compromising orthodontic treatment, that is, the therapist must not only eliminate the disease, but also understand how to adjust the anatomy of the tooth to the anatomy of aligners or braces. Such knowledge is usually correlated with the dentist's experience. Our clinic specializes in correcting bites, so the entire team, including therapists, have experience working with the dental system during orthodontic treatment.
Need some advice?
Enter your phone number and we will give you a free consultation on your problem
Make an appointment
*By making an appointment you consent to the processing of your data
Flash Free Method
The principle of Flash Free technology is the creation of an individual base for each tooth and each bracket. This technology is the result of development by 3M ESPE. They created a special material from very small polypropylene fibers, intertwined in a special way. The main feature of this material is that it compresses in the direction between the tooth and the bracket, but does not change in size in length and width. That is, it does not go beyond the bracket and does not form excess. An individual backing is made for each brace, strictly according to its dimensions and parameters. Next, this substrate is impregnated with a special glue, also developed specifically for this technique. It has several features:
- It does not spread over the surface of the tooth, as it has surface tension. On the surface of the tooth, the material looks like a drop of water on the surface of glass.
- It ensures reliable fixation of the bracket on the tooth not only through gluing, but also through the distribution of pressure between the tooth and the bracket.
- Due to its properties, this material is used in small quantities for fixation.
- The material practically does not absorb dyes and does not change color much during the treatment process.
Thanks to these features, Flash Free technology ensures a perfect fit of the bracket to the tooth - without gaps or excess material. 3M specialists also note that braces with Flash Free technology come off less often - in only 0.75% of cases (compared to 2.91% for braces fixed using the conventional method).
Prevention of caries
Some tips on how to avoid caries under braces or when treated with aligners:
- brush your teeth after eating, use oral hygiene products recommended by your doctor;
- When treating with braces, follow a diet: avoid sticky, fibrous, adhesive foods that can get stuck between the teeth and braces and cause the development of caries;
- use toothpaste and mouthwash with remineralizing properties (in consultation with your doctor);
- If the enamel darkens or plaque forms, undergo professional cleaning (in consultation with your doctor);
- do not miss scheduled visits to the orthodontist: they are needed not only to monitor the progress of orthodontic treatment, but also for the timely detection of problems with teeth and gums;
- After removing braces, some patients are prescribed a course of enamel remineralization to strengthen the enamel and prevent the occurrence of caries.
Following these recommendations will reduce the risk of caries when treated with braces or aligners. You can find out which bite correction method - braces or mouth guards - is right for you during a consultation at our clinic. Sign up now!
Proper care of braces and the oral cavity is the best prevention of caries
When deciding to install braces, it is important to understand that the orthodontic structure in the oral cavity makes brushing your teeth very difficult. And to maintain hygiene, it is important to follow a number of rules.
- A regular toothbrush will not be enough for cleaning.
To remove plaque and food debris even from hard-to-reach areas (from under the arch, around the clasps, in the spaces between teeth), you will need several devices. A person with braces should have a mono-beam and a V-shaped brush in their hygienic arsenal. Mono-beam is necessary to clean each tooth individually. Thanks to its compact size and special shape, it penetrates well under the arch and efficiently cleans dirt around the clasps of the orthodontic system, near the gums. A brush with a V-shaped cut ensures a tight fit of the bristles to the surface of the teeth, as if it goes around an arc on the teeth.
Recommendations:
- In addition to special brushes, it is important to use flosses and mouth rinses, which help remove dirt from hard-to-reach areas and reduce the number of bacteria in the oral cavity.
- For people who wear braces, it is advisable to purchase an irrigator with a special orthodontic attachment. Using a powerful water jet, this device qualitatively cleans the interdental spaces and all elements of the bracket system, increasing the cleaning efficiency several times.
- When wearing braces, it is recommended to brush your teeth not twice a day, but after every meal. The duration of cleaning should not be less than two to three minutes.
- The procedure for cleaning teeth when wearing braces is as follows: first, a V-shaped brush is passed over the entire dentition, then each tooth is cleaned individually with a monotuft brush-brush. At the end of the procedure, floss and rinse or oral irrigator are used.
How does cervical caries develop?
The beginning of cervical caries is the accumulation of plaque near the neck of the tooth.
Against the background of increased acidity and lack of oxygen, as well as under the action of enzymes secreted by bacteria, the enamel softens, opening the gates of infection.
The basal form of caries develops in 4 stages:
- in the first, known as the white spot stage, a dull white spot appears on the tooth at the level of the gum margin;
- at the second stage, a superficial carious lesion develops, which looks like darkening of the enamel;
- on the third, the carious cavity deepens through the enamel into the thickness of the dentin;
- at the fourth stage, deep caries develops, and a “hollow” forms in place of the spot.
The final stage of the disease is a fracture of the tooth in the neck area, pulpitis, accompanied by acute pain, and sometimes an abscess in the gum.
Why is a special diet recommended for patients with braces?
Products with a viscous consistency - chewing gum, toffee, halva, baked goods, corn sticks, chips - easily stick to the smooth surface of teeth and braces and are quite difficult to clean off, which means they contribute to the formation of plaque and the development of caries. It is easier to refuse their use during the treatment period, especially since they do not provide any particular benefit to the body as a whole.
Demineralization of teeth is known to be caused by sweet carbonated drinks and an abundance of sweets, the consumption of which should also be avoided. When wearing braces, it is recommended not to bite off hard fruits and vegetables such as apples and carrots, but to eat them cut into portioned cubes, so as not to increase the load on the teeth.
Treatment Options
A variety of techniques are used to treat cervical caries. Their choice depends on the stage of development of the carious lesion.
Spot stage
At the spot stage, radical methods of therapy are not used. To restore the strength of the enamel, it is enough to carry out 3-4 courses of remineralizing treatment, which consist of several stages:
- Professional teeth cleaning.
- Application of a carious stain with fluoride-containing compounds.
- Systematic oral care with products containing a high fluoride content: mouth rinses, toothpastes.
- Including salt and water enriched with fluoride in the diet.
After just 1-2 courses of remineralization, the white spot will be eliminated, and the risk of recurrent caries will decrease.
Stage of superficial caries
When caries spreads superficially, the doctor removes tartar and plaque, and then grinds the surface of the pathological focus to healthy tissue. To strengthen the enamel and prevent repeated destruction, several courses of remineralization are carried out.
Stage of middle caries
If enamel and dentin are damaged, preventive cleaning and fluoridation of tooth enamel is indispensable. To eliminate the pathology, the doctor will have to clean the carious cavity from putrefactive tissue, then literally saturate the dentin with drugs that suppress bacterial activity. Finally, the hole in the tooth is filled with polymer materials.
Stage of deep caries
With deep caries, treatment is extremely painful, so it is carried out only under local anesthesia. After the medicine takes effect, the doctor begins treatment:
- Pulls back the edge of the gum to have full access to the carious cavity.
- Cleans the carious cavity from necrotic tissue with dental instruments and a drill. If necessary, the pulp is removed and the dental nerve is extracted.
- The tooth cavity is isolated with special adhesive materials, and the equine canal is filled.
- Layer-by-layer filling is carried out with photopolymerization of each layer.
- The final grinding of the filling and tooth is performed.
This procedure takes several days or even weeks and costs several times more than treatment at the initial stage.