The smell of acetone on your breath - does diet matter?
The content of the article
An acetone odor from the breath is felt in people on a low-sugar diet. A decrease in the concentration of carbohydrates leads to the fact that the main source of energy for the body becomes fats, which form ketone bodies. Fats will also be the main source of energy received by the body in case of fasting and a small supply of sugars.
Symptoms of elevated ketone levels due to the ketogenic diet:
- Smell of acetone from the mouth.
An increased concentration of ketones is indicated by a noticeable smell of sour apples from the mouth. - Decreased activity
. Reducing the intake of carbohydrates initially leads to a feeling of constant fatigue, dizziness and nausea. Physical strength also decreases. This state lasts for several days or weeks until the body begins to burn more fat and switches to a new source of energy. - Disruption of the gastrointestinal tract
. The ketogenic diet can also lead to diarrhea and constipation. - Insomnia.
Sleep disturbances are a kind of signal from the body about carbohydrate deficiency. - Decreased appetite.
Patients begin to lose weight and appetite. This is due to the fact that a decrease in the concentration of carbohydrates in the blood leads to a decrease in the concentration of insulin and an increase in glucagon, which stimulates the oxidation of fatty acids. Increased protein degradation when using this diet can lead to negative consequences due to protein deficiency.
A low-carbohydrate, low-fat diet that leads to ketosis has long been used to treat epilepsy, especially in children.
Solutions to the problem
Comprehensive dental treatment is the key to good health of the chewing organs and oral cavity. It includes:
- full diagnostics;
- sanitation of the oral cavity;
- removal of soft and hard deposits;
- therapy of carious lesions;
- correction of bite;
- treatment of dental diseases;
The doctor pays special attention to denim tissues. If there is a need to remove teeth, surgical intervention is performed, after which prosthetics or implantation are planned.
When your breath smells of acetone, you need to eliminate all internal malfunctions and remove provoking factors. It is necessary to carry out thorough oral hygiene, which will remove unpleasant side effects. The problem can be completely overcome when the imbalance in the body is eliminated. To do this, patients must take a blood test for glucose levels, a urine test for ketones, and undergo a complete examination. Patients are prescribed a special diet. This speeds up the healing process.
Acetone breath and diabetes
Diabetes is a group of metabolic diseases that involve hyperglycemia—high blood sugar levels—associated with impaired insulin function or secretion. The patient's body, which cannot use carbohydrates as a source of energy as a result of impaired insulin secretion or action, begins to use fats for this purpose. As a result, ketone bodies are formed, which is the reason for the smell of acetone in the mouth. Some patients compare this smell to the smell of acid, gas or gasoline.
Chronic hyperglycemia causes damage to various organs, mainly the kidneys, eyes, blood vessels, heart and nerve fibers. There are several types of diabetes:
- type 1 diabetes;
- type 2 diabetes;
- gestational diabetes.
Type 1 diabetes is characterized by an absolute lack of insulin due to the destruction of beta cells in the pancreas. But the most common form of diabetes is type 2, which is characterized by impairment of both insulin secretion and function.
Diabetes
Typical symptoms of diabetes: increased thirst, polyuria, dehydration, drowsiness and weakness.
How does the smell appear?
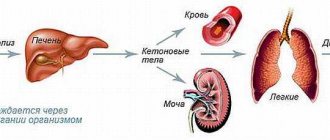
Fat metabolism disorders are the main reason why a person smells of acetone. What does it mean? During the metabolism of fatty acids, their breakdown products are formed - ketone bodies. They are the ones that give off the acetate smell.
Normally, the level of ketone bodies in the body is very low. They are quickly oxidized in the muscles and lungs, releasing large amounts of energy.
If a person smells like acetone, this means that ketones are accumulating in the body. This is observed when there is a violation of carbohydrate metabolism. Ketone bodies negatively affect the acid-base balance in the body. They shift the pH to the acidic side. Doctors call this disorder ketoacidosis. This condition poses a great health risk. Excess ketones have toxic effects on various organs.
Smell of acetone on the breath - ketoacidosis
Patients with diabetes can develop a life-threatening complication called ketoacidosis. This is a complex of acid-base disorders in which ketones appear in the urine and blood. This condition occurs as a result of insulin deficiency. Ketone bodies are most often produced in patients with type I diabetes, but may be present in test results in patients with other types of diabetes.
Sour breath is not the only symptom of this type of metabolic acidosis. Dehydration, glucose in the urine, electrolyte disturbances, disturbances of consciousness, feelings of weakness, drowsiness, vomiting, nausea, abdominal pain, chest pain, headache, dizziness, flushing, rapid heartbeat and rapid breathing are also observed. Without treatment, acidosis can cause coma.
In addition to diabetes, ketoacidosis and therefore acetone breath can cause:
- bacterial, fungal, viral infections, which increase the need for insulin;
- errors in insulin treatment;
- heart attack and stroke;
- pancreatitis.
Symptoms of an unpleasant odor
The symptoms of an unpleasant “aroma” depend on the amount of ketone substances present in the body. A mild form of symptoms manifests itself as follows:
- The drinker experiences morning sickness.
- The person begins to feel weak.
- The occurrence of ketonuria. It can only be determined by urine analysis.
If a drinker has consumed a lot of alcohol, he may develop more serious symptoms, the causes of which are hidden in the drinking of alcohol. These signs include:
- Decreased amount of urine. This occurs due to the fact that water metabolism in the body is disrupted.
- The mouth and tongue are covered with a thin film.
- The appearance of vomiting (especially in the morning).
- Weakness that appears for no reason.
- Severe pain in the temple area.
Having identified these symptoms, you need to take measures to eliminate them, as they quickly cause the appearance of an acetone odor.
Acetone smell from child's mouth
Children's breath smells like acetone most often due to type I diabetes. The disease develops slowly and insidiously, so parents often do not know that their child is sick. In addition, young patients often experience weight loss, excessive thirst, weakness, and pollakiuria.
This type of odor can also occur when a child doesn't drink enough. Sometimes parents report an ammonia odor from their child's mouth during an infection such as pharyngitis.
A strange smell from the mouth should prompt parents to contact a pediatrician, who will prescribe the necessary examinations.
Possible reasons
What disease causes a person to smell of acetone? The accumulation of ketones can occur with various ailments. Most often, ketoacidosis develops against the background of the following pathological conditions:
- diabetes mellitus;
- pathologies of the liver and kidneys;
- disorders of the thyroid gland;
- infectious diseases;
- deficiency of carbohydrates in food;
- long fasting.
Next, we will consider in detail the above diseases and methods of treating them.
How to get rid of odor
What to do if a person smells of acetone? You can completely get rid of an unpleasant odor only after eliminating its cause. Therefore, first of all, you need to treat the underlying pathology and avoid too strict diets.
The following recommendations from doctors will also help reduce the odor:
- You should try to consume enough fluid.
- Long breaks between meals should be avoided.
- You should shower regularly and use antibacterial soap.
- Wearing clothes and underwear made from natural fabrics will help reduce sweating.
- It is recommended to use deodorants with zinc and aluminum.
The acetone smell is a rather dangerous symptom that should never be ignored. Timely treatment will help avoid intoxication of the body and damage to organs from ketones.
If the problem is in the nose
Most often, the smell of acetone in the nose is associated with foreign bodies entering the nasal passage.
Moreover, even after the object has been successfully removed, unpleasant sensations may persist for some time.
If the discomfort does not go away for a long time, you need to make sure that there are no wounds on the mucous membrane that could become infected.
- Smells in the nose: causes, possible diseases, treatment methods, reviews
By the way, the second most common reason is damage to the mucous membrane and the development of small foci of infection.
In this case, it is necessary to treat the infection with antiviral or antibacterial drugs. Some of them will have to be taken orally, others are available in the form of a spray and drops.
Remember! One of the reasons that causes unpleasant odors in the nose is ozena: a complex but, fortunately, rare disease.
Hyperketonemia syndrome in children and adolescents: pathogenesis, causes, diagnosis
Part 2. Read the beginning of the article in No. 6, 2022.
Starvation
Fasting is a state of the body associated with partial or complete disruption of food intake. In a state of starvation, the body's energy sources for the most important structures of the body are sharply reduced. Under conditions of nutrient deficiency in the body, energy production occurs due to the intensification of glucogenesis and the synthesis of ketone bodies. The blood glucose level decreases to the lower limits of normal (3.5 mmol/l) and is maintained at this level during subsequent periods of fasting. In the liver, during fasting, glucose is not able to provide the required amount of oxaloacetate, since it simply is not in the cell. Therefore, during fasting, fatty acids do not “burn” in the TCA cycle, but are converted into ketone bodies.
A decrease in glycogen reserves in the liver is accompanied by an increased supply of free fatty acids from adipocytes. The concentration of fatty acids in the blood increases 3–4 times compared to the post-absorptive state. The level of ketone bodies in the blood increases 10–15 times after a week of fasting. At the same time, carbohydrate deficiency inhibits the oxidation of ketone bodies, slowing down their resynthesis into higher fatty acids [13].
The energy needs of muscles and most other organs are met by fatty acids and ketone bodies. When insulin levels are low, glucose does not penetrate into muscle cells; glucose consumers are insulin-independent cells and, above all, brain cells, but even in this tissue, bioenergetics is partially provided by ketone bodies. At this concentration, acetoacetic acid is actively decarboxylated to form acetone, which is excreted in exhaled air and through the skin. Already on the 3rd–4th day, the smell of acetone emanates from the mouth and skin of the fasting person.
The body includes alternative methods of energy production - gluconeogenesis and the synthesis of keto acids, which are consumed by the central nervous system. During fasting, the release of glucagon increases, which activates lipolysis in adipocytes and oxidation in the liver. The amount of oxaloacetate in mitochondria decreases, since it, having been reduced to malate, enters the cytosol of the cell, where it is again converted into oxaloacetate and used in gluconeogenesis.
Gluconeogenesis continues due to the breakdown of tissue proteins. Amino acids are formed as a result of the breakdown of muscle proteins and are included in gluconeogenesis during prolonged fasting. Pyruvate is formed in the liver from lactate and alanine. Alanine and glutamine are the most important glucogenic amino acids during fasting. Pyruvate and metabolites of the TCA cycle are capable of forming oxaloacetate and being involved in gluconeogenesis.
During fasting, the use of acetyl-CoA in the TCA cycle is suppressed and it is used exclusively for the synthesis of hydroxymethylglutaryl-CoA, which leads to an increase in the formation of ketone bodies. Under these conditions, ketone bodies are an alternative (to glucose) energy material for the brain and other tissues. 75% of the brain's energy needs are met by acetyl-CoA [4].
If fasting continues for days or weeks, other homeostatic mechanisms are activated that ensure the preservation of the protein structure of the body, slowing down gluconeogenesis and switching the brain to utilize ketone molecules. The signal for the use of ketones is an increase in their concentration in arterial blood. With prolonged fasting, extremely low concentrations of insulin in the blood are observed. In this case, intensive ketogenesis is a compensatory adaptive reaction.
The metabolic rate is generally reduced: after a week of fasting, oxygen consumption decreases by approximately 40%, oxidative processes in mitochondria are inhibited and oxidative phosphorylation is inhibited with the formation of ATP, i.e., a hypoenergetic state develops.
Accumulating in the blood, ketone bodies suppress the secretion and activity of glucocorticoids, thereby preventing the destruction of structural proteins of the body and inhibiting the secretion of glucagon [2]. If alanine or other glycogenic amino acids are administered to a fasting person at this time, the level of glucose in the blood increases and the concentration of ketone bodies decreases.
During fasting, ketosis does not pose a danger, since it does not reach the level of ketoacidosis. The latter develops with accompanying factors - dehydration, alcohol intoxication and other conditions.
Alcohol intoxication
Overproduction of ketoacids and ketoacidosis after excessive drinking are common observed conditions. Ethyl alcohol catabolism occurs mainly in liver mitochondria. Here, from 75% to 98% of the ethanol introduced into the body is oxidized. Alcohol oxidation is a complex biochemical process. Nicotinamide adenine dinucleotide (NAD) plays a major role in ethanol metabolism. This enzyme converts ethanol into the toxic metabolite acetaldehyde and reduced NADH, and the latter corresponds to the synthesis of acetoacetate and β-hydroxybutyrate.
Alcohol dehydrogenase catalyzes a reversible reaction, the direction of which depends on the concentration of acetaldehyde and the NADH/NAD+ ratio in the cell. An increase in the concentration of acetaldehyde in the cell causes the induction of the enzyme aldehyde oxidase. During the reaction, acetic acid is formed.
The acetic acid obtained during the reaction is activated by the enzyme acetyl-CoA synthetase. The reaction takes place using coenzyme A and the ATP molecule. The resulting acetyl-CoA, depending on the ATP/ADP ratio and the concentration of oxaloacetate in the mitochondria of hepatocytes, can be “burned” in the TCA cycle or used for the synthesis of fatty acids or ketone bodies.
In the initial stages of alcoholism, acetyl-CoA in the TCA cycle is the main source of energy for the cell. Excess acetyl-CoA in citrate leaves the mitochondria, and fatty acid synthesis begins in the cytoplasm.
During the period of acute alcohol intoxication, despite the presence of a large amount of acetyl-CoA, the lack of oxaloacetate reduces the rate of citrate formation. Under these conditions, excess acetyl-CoA is used for the synthesis of ketone bodies. An increase in the concentration of NADH compared to NAD+ slows down the lactate oxidation reaction, and the lactate/pyruvate ratio increases. The concentration of lactate in the blood increases, which leads to hyperlactic acidemia and lactic acidosis. An increase in the blood levels of lactate, acetoacetic acid and β-hydroxybutyrate causes metabolic acidosis during alcohol intoxication [14].
Promotes enhanced ketogenesis during alcohol intoxication and hypoglycemic conditions associated with vomiting and fasting. It is also known that in such patients the level of insulin in the blood is reduced, while the levels of cortisol, growth hormone, glucagon and adrenaline are increased. Ethanol inhibits gluconeogenesis. Dehydration in these cases promotes ketogenesis.
Ketosis due to hormonal imbalance
Blood glucose levels are influenced by a wide range of hormones, with only insulin causing the hypoglycemic effect. All hormones have a contrinsular effect with an increase in blood glucose levels: glucagon, adrenaline, glucocorticoids, adrenocorticotropic (ACTH), somatotropic (STG), thyroid-stimulating (TSH), thyroid.
The effects of insulin and counter-insular hormones normally regulate stable blood glucose levels. When insulin concentrations are low, the hyperglycemic effects of other hormones, such as glucagon, adrenaline, glucocorticoids and growth hormone, are enhanced. This happens even if the concentration of these hormones in the blood does not increase.
The pathogenesis of ketosis with an excess of thyroxine, glucocorticoids, somatotropin and/or other hormones is essentially similar to the already discussed mechanisms of hyperproduction of ketoacids due to an excess of contrainsular hormones [6]. It is known that during periods of increased growth, as well as during hyperthyroidism, significant weight loss occurs.
Stress
Under stress, the sympathetic nervous system is activated and counter-insular hormones are released, the body's carbohydrate reserves are depleted, and the liver's ability to synthesize and store glycogen is impaired. There is an excessive intake of non-esterified fatty acids into the liver. As a result of increased production of glucocorticoids, protein breakdown and increased formation of ketone bodies from ketogenic amino acids occurs.
Hypercortisolism
Acetonemic syndrome may be the first clinical manifestation of hypercortisolism, when the characteristic signs of the disease have not yet formed.
Glucocorticoids enhance the mobilization of neutral fats from adipose tissue and inhibit lipogenesis. But this effect in the body can be overlapped by other effects of these hormones: the ability to cause hyperglycemia and stimulate insulin secretion, accumulation of glycogen in the liver, which leads to inhibition of fat mobilization and its deposition in adipose tissue; the ability in large doses to delay fat-mobilizing and stimulating fat oxidation by somatotropin.
This may explain the accumulation of fat in fat depots during hypercortisolism (Cushing's disease and syndrome). In addition, in this condition, the formation of dihydrocortisone is increased, which stimulates the pentose cycle and the conversion of carbohydrates into fats. Corticotropin, by stimulating the secretion of glucocorticoids, can influence fat metabolism in the same direction, but, in addition, it also has an extra-adrenal fat-mobilizing effect [6].
Thyrotoxicosis
An excess of thyroid hormones in the blood can be a consequence of diseases manifested by hyperfunction of the thyroid gland. A severe complication of the underlying disease, accompanied by hyperfunction of the thyroid gland, is thyrotoxic crisis, which is a sharp exacerbation of all symptoms of thyrotoxicosis. Excessive intake of thyroid hormones into the blood causes severe toxic damage to the cardiovascular system, liver, nervous system and adrenal glands. The clinical picture is characterized by severe agitation (up to psychosis with delusions and hallucinations), which is then replaced by weakness, drowsiness, muscle weakness, and apathy. Dyspeptic disorders intensify: thirst, nausea, vomiting, loose stools. Possible liver enlargement. Against this background, the processes of ketogenesis sharply intensify, which can provoke symptoms of acetonemia.
Thyroxine has a fat-mobilizing effect. With hyperthyroidism, carbohydrate metabolism is increased. Increased utilization of glucose by tissues. Phosphorylase of the liver and muscles is activated, resulting in increased glycogenolysis and depletion of these tissues in glycogen. Hexokinase activity and glucose absorption in the intestine increase, which may be accompanied by nutritional hyperglycemia. Liver insulinase is activated, which, together with hyperglycemia, causes intense functioning of the insular apparatus and, in case of its functional inferiority, can lead to the development of diabetes mellitus. Strengthening the pentose pathway of carbohydrate metabolism promotes the formation of NADP-H2. In the adrenal glands, this causes increased steroidogenesis and greater production of corticosteroids [4].
Hormone deficiency
Hypoglycemia always occurs with panhypopituitarism, a disease characterized by a decrease and loss of function of the anterior pituitary gland (secretion of adrenocorticotropin, prolactin, somatotropin, follitropin, lutropin, thyrotropin). As a result, the function of the peripheral endocrine glands sharply decreases. However, hypoglycemia also occurs with primary damage to the endocrine organs (congenital dysfunction of the adrenal cortex, Addison's disease, hypothyroidism, hypofunction of the adrenal medulla, glucagon deficiency). With a deficiency of contrainsular hormones, the rate of gluconeogenesis in the liver decreases (impacting the synthesis of key enzymes), glucose utilization in the periphery increases, and the formation of amino acids in the muscles, the substrate for gluconeogenesis, decreases.
Glucocorticoid deficiency
Primary adrenal insufficiency is a consequence of decreased secretion of hormones from the adrenal cortex. This term refers to variants of hypocortisolism that differ in etiology and pathogenesis. Symptoms of adrenal insufficiency develop only after 90% of the adrenal tissue volume has been destroyed.
The causes of hypoglycemia in adrenal insufficiency are similar to the causes of hypoglycemia in hypopituitarism. The difference is the level of occurrence of the block - with hypopituitarism, the secretion of cortisol is reduced due to ACTH deficiency, and with adrenal insufficiency due to the destruction of the tissue of the adrenal glands themselves.
Hypoglycemic conditions in patients with chronic adrenal insufficiency can occur both on an empty stomach and 2-3 hours after eating a meal rich in carbohydrates. Attacks are accompanied by weakness, hunger, and sweating. Hypoglycemia develops as a result of decreased cortisol secretion, decreased gluconeogenesis, and glycogen stores in the liver.
Catecholamine deficiency
This condition can occur with adrenal insufficiency with damage to the adrenal medulla. Catecholamines, entering the blood, regulate the release and metabolism of insulin, reducing it, and also increase the release of glucagon. With a decrease in the secretion of catecholamines, hypoglycemic conditions are observed, caused by excess insulin production and reduced glycogenolysis activity.
Glucagon deficiency
Glucagon is a hormone that is a physiological antagonist of insulin. It is involved in the regulation of carbohydrate metabolism and affects fat metabolism, activating enzymes that break down fats. The main amount of glucagon is synthesized by the alpha cells of the pancreatic islets. However, it has been established that special cells of the duodenal mucosa and gastric mucosa also synthesize glucagon. When glucagon enters the bloodstream, it causes an increase in the concentration of glucose in the blood, up to the development of hyperglycemia. Normally, glucagon prevents an excessive decrease in glucose concentration. Thanks to the existence of glucagon, which prevents the hypoglycemic effect of insulin, fine regulation of glucose metabolism in the body is achieved.
With a deficiency of the above hormones, the insulin content is reduced, and the excretion of ketone bodies in the urine is increased [4].
The role of the liver in energy metabolism disorders
The liver is involved in maintaining normal serum glucose levels through glycogenogenesis, glycogenolysis, and gluconeogenesis. The basis of carbohydrate metabolism disorders in liver diseases is damage to mitochondria, which leads to a decrease in oxidative phosphorylation. Liver functions are secondarily affected. In severe acute hepatitis, hypoglycemia is usually observed, and in liver cirrhosis this occurs in the final stage - with liver failure [15]. Hypoglycemia is explained by a decrease in the ability of the liver (due to extensive damage to its parenchyma) to synthesize glycogen and a decrease in the production of insulinase (an enzyme that destroys insulin).
Carbohydrate deficiency also leads to increased anaerobic glycolysis, as a result of which acidic metabolites accumulate in cells, causing a decrease in pH. In liver cirrhosis, the level of lactate in the blood serum may also increase due to the reduced ability of the liver to utilize it for gluconeogenesis.
In liver diseases, the role of fats as an energy source increases. In the liver, fatty acids are synthesized and broken down to acetyl-CoA, as well as the formation of ketone bodies, saturation of unsaturated fatty acids and their inclusion in the resynthesis of neutral fats and phospholipids. Catabolism of fatty acids is carried out by β-oxidation, the main reaction of which is the activation of fatty acids with the participation of the coenzyme acetyl-CoA and ATP. The released acetyl-CoA undergoes complete oxidation in the mitochondria, as a result of which the cells are provided with energy.
In a number of liver diseases, the synthesis of lipoproteins is also reduced, which leads to the accumulation of triacylglycerides with subsequent infiltration and fatty degeneration of the liver. The causes of this condition, in particular, are the lack of lipotropic substances in food (choline - a component of lecithin, methionine). The formation of ketone bodies increases [4].
So, the clinical picture of secondary acetonemic syndrome directly includes the phenomena of ketosis, signs of the underlying disease against which ketosis developed, as well as manifestations of the condition that triggered the pathological process (stress, excessive physical activity, infection, etc.).
Acetonemic cyclic vomiting
In practice, one has to deal with idiopathic acetonemic vomiting, which occurs with ketoacidosis (acetonemic vomiting, non-diabetic ketoacidosis). In the English-language literature, it is included in the syndrome of idiopathic cyclic vomiting [16, 17].
The pathogenesis of acetonemic vomiting is not fully understood. It is assumed that in children after infectious diseases, skull injuries, organic diseases of the central nervous system, a dominant focus of stagnant excitation remains for a long time in the hypothalamic-diencephalic region, inducing disorders of fat metabolism (increased ketogenesis, disruption of the normal use of ketone bodies due to depletion carbohydrate reserves in the body). In the pathogenesis of acetonemic vomiting, constitutional anomalies, relative incompetence of liver enzyme systems, and disturbances in endocrine regulation of metabolism may play a role.
The concept of cyclic vomiting syndrome as a mitochondrial pathology is promising [18, 19]. Since mitochondria are, figuratively speaking, the energy stations of the cell, energy metabolism is disrupted in this disease. Under conditions of stress and hypoxia, energy metabolism is disrupted with a predominance of faster anaerobic glycolysis, but only 2 ATP molecules are formed, whereas under aerobic glycolysis - 38 [5]. There is an energy deficit.
Such disorders are closely related to disorders of purine metabolism, since energy in the body is stored in the form of nucleotides, among which adenine and guanine are purines, and they are metabolized to uric acid, and thymine, cytosine and uracil are pyrimidines and are metabolized to form ketone bodies, ammonia and β-isobutyric acid. These ideas pathogenetically bring together the syndrome of cyclic vomiting and the syndrome of acetonemic vomiting, and also explain the need and possible ways of metabolic correction.
Others believe that the reason for the sharp increase in ketone bodies may be insufficient consumption of carbohydrates in children with an excess of fats and ketogenic amino acids.
Crises can occur suddenly at intervals of several weeks or months. Provoking factors may be: poor diet (fried and baked foods), fever, refusal to eat, physical and mental stress.
Harbingers of cyclic vomiting syndrome are anorexia, lethargy or increased excitability, nausea, headaches, abdominal pain, and the smell of acetone from the mouth.
Then repeated or uncontrollable vomiting appears, which can last from one to five days. Cramping pain in the abdomen intensifies. During a crisis, the patient becomes drowsy. As a result of vomiting, hemodynamic disturbances may develop: tachycardia, soft pulse, muffled heart sounds, hypotension.
The liver is moderately enlarged. In some cases, the temperature rises. The smell of rotten apples is felt in the exhaled air and vomit. There is a high concentration of ketone bodies in the urine. Seizures can resolve spontaneously without treatment.
An excess of ketone bodies has a narcotic effect on the central nervous system, which is clinically manifested by lethargy and lethargy.
A biochemical blood test reveals a disorder of lipid metabolism (hypercholesterolemia), a tendency to hypoglycemia, and hyperketonemia. General blood test: moderate leukocytosis, neutrophilia, accelerated ESR.
Acetone is found in urine and exhaled air, and an increased concentration of ketone bodies is found in the blood. The electroencephalogram reveals various abnormalities that do not disappear completely after the attack stops.
This syndrome is more common in preschool age and is accompanied by attacks of repeated vomiting and ketonemia. Such patients are often diagnosed with increased excitability, uric acid nephropathy, diabetes mellitus, and obesity.
Ketosis during prolonged vomiting, malnutrition or fasting represents a classic compensatory process designed to compensate for the energy deficit, more precisely, the lack of carbohydrates, through alternative energy substrates of keto acids.
The diagnosis of acetonemic vomiting syndrome can be confirmed only after excluding other diseases accompanied by vomiting: appendicitis and peritonitis, encephalitis, meningitis, the onset of cerebral edema, poisoning, toxicosis and infectious diseases, etc. But primarily diabetic ketoacidosis.
Acetonemic crises in most children stop after 10–12 years, but there remains a high probability of developing pathological conditions such as gouty crises, vegetative-vascular dystonia of the hypertensive type, and arterial hypertension.
Transient ketosis in children and adolescents can be detected during fever, stress, infectious diseases, fasting (during illness), eating foods rich in fat, and strenuous physical activity. In these cases, the content of ketone bodies in the urine is no more than 2+.
Treatment
Treatment and prevention of hyperketonemia depend on the cause of its occurrence, but in all cases are aimed at improving liver function and normalizing energy metabolism. This is achieved by limiting the fat content in the diet, prescribing lipotropic agents (methionine, etc.), B vitamins, and, if necessary, insulin and cocarboxylase.
During an attack of cyclic acetonemic vomiting syndrome, severe dehydration, hypovolemia, metabolic acidosis and electrolyte disturbances are the main factors that determine the severity of the condition. It is necessary first of all to eliminate acidosis: prescribe gastric and intestinal lavage with 1–2% sodium bicarbonate solution. A 5–10% glucose solution with the addition of the required amount of insulin, as well as Ringer’s solution, have antiketogenic properties [20].
If drinking does not provoke vomiting, sweetened tea, Regidron, Oralit are recommended - in frequent and small volumes. After the condition improves and it becomes possible to take fluids, feeding the child is prescribed. The diet should contain easily digestible carbohydrates and a limited amount of fat (semolina, oatmeal, buckwheat porridge; mashed potatoes, baked apples, crackers, dry cookies).
So, elucidating the mechanisms of development of ketonemic syndrome and identifying the most likely causes of the formation of ketosis make it possible to establish the genesis of the disease, and thereby normalize the patient’s condition and prevent relapses of ketonemia.
Literature
- Berezov T. T., Korovkin B. F. Biological chemistry. Textbook. 3rd ed. M.: Medicine, 2004. 704 p.
- Stryer, Lubert. Biochemistry (Fourth ed.). New York: W. H. Freeman and Company, 1995. pp. 510–515, 581–613, 775–778.
- Murray R., Grenner D., Mayes P., Rodwell V. Human biochemistry. Per. from English M.: Mir, 1993. T. I. 381 p.
- Zaichik A. Sh., Churilov L. P. Fundamentals of pathochemistry. St. Petersburg: Elbi-SPb, 2000. 687 p.
- Endocrinology and metabolism. In 2 volumes / Ed. Felinga F. et al. Per. from English Kandrora V.I., Starkova N.T.M.: Medicine, 1985. T. 2. 416 p.
- Endocrinology: national guide / Ed. Dedova I. I., Melnichenko G. A. M.: GEOTAR-Media, 2008.
- Treatment of diabetic coma in children. Guidelines. M., 2006. 14 p.
- Brown LM, Corrado MM, van der Ende RM et al. Evaluation of glycogen storage disease as a cause of ketotic hypoglycemia in children // J Inherit Metab Dis. 2015, May; 38(3):489–493.
- Chibiras P. P. Hypoglycemic ketonemia as a cause of neurotoxicosis in children // Issues of maternal and childhood protection. 1982. No. 2. P. 30–33.
- Genes S.G. Hypoglycemia. Hypoglycemic symptom complex. M.: Medicine, 1970. 236 p.
- Kronenberg G. M. et al. Obesity and lipid metabolism disorders. Per. from English edited by I. I. Dedova, G. A. Melnichenko. M.: Read Elsiver LLC, 2010. 264 p.
- Lukyanchikov V.S. Ketosis and ketoacidosis. Pathochemical and clinical aspect // RMJ, 2004, v. 12, no. 23, p. 1301.
- Maslovskaya A. A. The mechanism of development of ketosis in diabetes mellitus and fasting // Journal of the Grodno State Medical University. 2012, no. 3 (39), 8–10.
- Emergency medical care. Per. from English / Ed. J. E. Tintinally, R. L. Crome, E. Ruiz. M.: Medicine, 2001. 1000 p.
- Ryabchuk F.N., Pirogova Z.I. Coenzyme acetylation and the level of free fatty acids in the blood in children with acetonemia and biliary insufficiency // Treating Doctor. 2012, no. 8, p. 42–46.
- Li BUK: Cyclic vomiting: new understanding of an old disorder // Contemporary Ped. 1996, 13(7): 48–62.
- Krakowczyk H., Machura E., Rusek-Zychma M., Chrobak E., Ziora K. Assessment of the natural history and clinical presentation of acetonemic vomiting. 2014, 71 (6): 323–327.
- Boles R. et al. Cyclic vomiting syndrome and mitochondrial DNA mutations // Lancet. 1997, 350: 1299–1300.
- Salpietro CD, Briuglia S, Merlino MV et al. A mitochondrial DNA mutation (A3243 G mtDNA) in a family with cyclic vomiting // Am. J. Pediatr. 2003. 162. 727–728.
- Marushko Yu. V., Shev G. G., Polkovnichenko L. N., Moshkina T. V. Therapeutic approaches for acetone syndrome in children // Child’s Health. 2012, No. 1, p. 61–65.
V. V. Smirnov1, Doctor of Medical Sciences, Professor A. V. Simakov
Federal State Budgetary Educational Institution of Russian National Research University named after. N. I. Pirogova Ministry of Health of the Russian Federation, Moscow
1 Contact information
Prevention and treatment
Blood and urine analysis - with elevated acetone
Suspicion of ketoacidosis requires immediate hospitalization. The first treatment measure is the administration of insulin, which normalizes the chemical state of the blood. Insulin administration also prevents the development of coma and other dangerous complications.
Additional measures to treat the condition:
- Replenishing fluid in the body. If the child is unconscious, fluid is administered intravenously.
- Compensation for lack of electrolytes. Also via intravenous administration.
- Therapy of infectious and inflammatory diseases that provoke ketoacidosis.
To treat ketoacidosis, your doctor may prescribe a different dosage of insulin. The following types of drug may be prescribed:
- Fast acting insulin.
- Long acting insulin.
Prescribing different types of insulin allows you to monitor the patient’s condition on a long-term basis and prevent relapses of the disease.
Preventive measures: