Oral tuberculosis is an infectious disease that, like other types of tuberculosis, is caused by mycobacteria. This pathology is classified as chronic. As a rule, the inflammation characteristic of tuberculosis, affecting the lining of the mouth and the red border around the lips, is secondary: that is, it occurs as a consequence or the most characteristic manifestation of other forms of tuberculosis. For example, these include tuberculous lesions of the lymph nodes and bones.
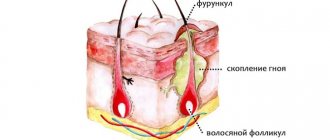
The mucous membrane of the oral cavity is far from the most favorable environment for the development and reproduction of mycobacteria that cause tuberculosis. As a rule, when entering this environment, mycobacteria die. However, in the presence of favorable circumstances (microtraumas, mechanical damage in the oral cavity, opening the gates for infection), bacteria penetrate inside and provoke the formation of a tuberculosis ulcer.
Oral tuberculosis is a relatively rare form of tuberculosis, usually diagnosed only in children. This is due to the characteristics of teething in children.
In an infant, such a disease can be extremely severe and includes the generalization of tuberculosis infection. Secondary tuberculosis infection begins to develop as tuberculous lupus or miliary ulcerative tuberculosis.
Tuberculosis is transmitted by airborne droplets. The incubation period lasts from eight to thirty days, and after this the formation of an uneven, blurred ulcer begins, which is severely painful. After a few days it begins to gradually increase. At the same time, the adjacent lymph nodes swell. There are no other signs of inflammation yet
Classification of types of oral tuberculosis
Oral tuberculosis is a disease that appears and develops mainly in patients with reduced immunity. The disease is caused by Koch's bacillus. The source of inflammation located in the patients' oral cavity is secondary in most cases. It develops as a result of the spread of infection from the main focus, and spreads through the circulatory or lymphatic systems. In the case when the patient is affected by the pulmonary form of tuberculosis, the infection spreads to the oral cavity due to the penetration of mycobacteria contained in the sputum.
There are four forms of oral tuberculosis. Among them:
- Primary tuberculosis of the oral cavity. Transmitted by the respiratory or fecal-oral route, this disease almost never occurs in adults. Most patients with this diagnosis are infants.
- Tuberculous lupus. It is the lupus form of oral tuberculosis that is most often encountered in dental practice. Erosive elements are localized on the mucous membrane of the gums. If treatment is not started on time, these tumors can develop into a malignant form.
- Miliary-ulcerative form. This form usually develops in patients who have already been weakened by tuberculosis. Along with their cough, they produce sputum, which is a source of bacteria that cause oral tuberculosis. The lesions are on the palate and tongue, in rare cases - in the area of marginal gums or on the side of the cheek.
- Scrofuloderma. This form of the disease is diagnosed in most cases in children. The clinical signs of scrofuloderma are somewhat different from those of other forms of oral tuberculosis. In the first stages - the appearance of not a tubercle, but a rather large nodule. After its softening and necrosis occurs, the stage of formation of fistula tracts begins. The healing process of the surface of the resulting ulcers takes a long time, and after it characteristic fringed scars form.
Tuberculosis of the maxillofacial area
- Primary tuberculous lesion
Primary tuberculosis is characteristic of childhood and usually occurs in children who have had contact with tuberculosis patients.
The disease can also develop from consuming infected milk from infected cows. Infection can occur through trauma and inflammation of the mucous membrane, pharynx, skin and marginal periodontium, the presence of marginal pockets, carious teeth, holes after extracted teeth. Tuberculous lesions are most often localized on the mucous membrane, skin or jaw bones. Regional lymph nodes may be involved in the process. In such cases, a primary complex arises, similar to the primary complex in the lungs and other organs. At the site of penetration into the skin, after incubation, which lasts 1-3 weeks, limited swelling occurs. A papular, vesicular or pustular formation gradually forms. After ulceration, suppuration and rejection of the crust, an ulcer with irregular, undermined edges remains, the bottom of which is made of granulations and small yellowish nodules. After 1-2 months, the primary tuberculous ulcer scars or, which is less common, tends to spread to neighboring areas, and a separate ulcer transforms into an extensive ulcerative surface. In the oral cavity in children, tuberculosis lesions develop most often in the tonsils, gums, and less often in the nasopharynx. Yaroslav Toman describes damage to the mucous membrane in the gum area as a granulomatous process. Tuberculous granulations, according to his observations, are soft, spongy, bleed easily and are characterized by flat growth. Teeth in the affected area may become loose and fall out. The sockets of fallen teeth are filled with specific granulations containing tuberculous tubercles.
The jaw bones in children are rarely involved in the process by contact during the primary lesion. Primary damage to the maxillofacial area is accompanied by involvement of regional lymph nodes in the process. Usually one group of nodes is affected. The lymph nodes enlarge, become fused together into bags, and soften. Cheesy necrosis ends with the melting of the nodes, opening and formation of fistulas. Fibrosis and calcification of the nodes may be noted.
- Secondary tuberculous lesion
Secondary damage to the maxillofacial area occurs in children with tuberculosis, and thus serves as a manifestation of the generalization of the process by hematogenous or lymphogenous routes. Secondary lesions are most often localized in the jaws or zygomatic bones. In the upper jaw, the process involves the anterior wall, the lower orbital margin, as well as the zygomatic and alveolar processes. In the lower jaw, the process is most often localized in the area of the angle, ramus and alveolar process. At the beginning of the disease, moderate swelling appears, which slowly increases. Within 1-2 months, the skin acquires a bluish tint, sometimes with mild hyperemia. The process is developing slowly. Subsequently, tissue infiltration in the affected area is observed, followed by softening and the formation of a “cold” abscess, which can spontaneously open through the fistula tracts. A long-term tuberculous process in the bone is sometimes accompanied by multiple fistulas, leaving disfiguring scars. In recent years, more benign forms of the tuberculosis process in the jaws have been observed. The disease occurs as an osteitis with a pronounced periosteal reaction. This option is typical for damage to the upper jaw and zygomatic bone.
X-ray examination reveals one or another degree of destruction in the form of foci or zones of osteoporosis. With an active process, destruction begins to spread from a fairly local primary site of the lesion. A periosteal reaction is detected on the lower jaw. Sequestrations are rarely formed. With secondary damage to the jaws, regional lymph nodes are involved in the process.
- Tuberculous lymphadenitis
Tuberculous lymphadenitis (tuberculous lesions of the lymph nodes of the cervical and maxillofacial region) in children occupies one of the first places among all other tuberculous lymphadenitis. R.A. Kalmakhelidze noted tuberculous lesions of the lymph nodes of the maxillofacial region in 7.1% of patients with lymphadenitis.
Submitted by M.Ya. Zazulevskaya, tuberculous lymphadenitis accounts for 13.8% of the total number of perimandibular lymphadenitis.
There are two possibilities for the occurrence of tuberculosis of the lymph nodes of the maxillofacial area. In the first case, the “entry gate” for tuberculosis infection is inflammatory foci and damage to the mucous membrane, nasal cavity, adenoids and tonsils, and affected teeth. If mycobacteria tuberculosis in the nodes do not die (phagocytosis and lysis-lymphocytes), then they are fixed and give rise to a local focus of the disease. Tuberculosis of peripheral lymph nodes can also occur as a secondary manifestation in the presence of specific changes in other organs (lungs, joints, bones, etc.). But often, with any route of penetration of tuberculosis infection into the body, the lymph nodes, primarily the submandibular and cervical ones, are affected first of all.
The acute onset of tuberculous lymphadenitis in the maxillofacial area is not typical, although it does occur. Local manifestations at the onset of the disease in such cases are similar to nonspecific acute lymphadenitis. Characteristic is sharp hyperplasia of the affected node. The lymph node can enlarge to the size of a “chicken egg”. Often abscess formation of the affected nodes with subsequent formation of a fistula. After the acute inflammatory phenomena subside, the node remains enlarged, mobile, elastic, slightly fused with the surrounding tissues for a long time. General manifestations of acute tuberculous lymphadenitis resemble those of acute nonspecific lymphadenitis.
The chronic course of the disease is more common than acute. The process begins with an enlargement of a lymph node or groups of nodes in a particular area. The affected nodes have a densely elastic consistency with clear contours and a somewhat bumpy surface, painless or slightly painful on palpation, in most cases mobile, sometimes fused with surrounding tissues and skin. The color of the skin over the nodes is not changed, it folds freely or with some difficulty. This condition of the lymph node or nodes persists for a long time. As the disease develops, neighboring nodes are also involved in the process, forming “packages” of lymph nodes welded together. Along with “packages” of nodes fixedly fused to the skin, individual moving nodes are observed without the phenomena of periadenitis and skin changes. The tendency to cheesy disintegration and suppuration leads to the formation of fistulas with copious purulent discharge and inflammatory changes in the skin circumference. Fistulas do not heal for a long time, periodically closing and opening. Tuberculosis damage to the lymph nodes can be unilateral or bilateral, affecting one or more groups. With secondary lymphadenitis, perifocal infiltration is insignificant, signs of hyperplasia of the affected nodes predominate.
In some cases, foci of softening are identified; sometimes the softened nodes cover the entire “package” of lymph nodes tightly fused to each other and to the skin. When lymphadenitis begins with damage to several nodes at once, the process of formation of “packets” and the further development of the disease are characterized by a more rapid course. In the later stages of the disease, especially in cases where the patient is examined for the first time, 1-2 years after the onset of the disease, slightly enlarged but sharply compacted lymph nodes can be detected, which may indicate previous caseous decay and subsequent calcification of the affected node.
Along with damage to the submandibular and cervical lymph nodes, almost all children experience micropolyadenitis. The general condition of children with isolated primary lesions of the lymph nodes almost does not worsen.
- Colliquatic tuberculosis (scorfuloderma)
Colliquatic tuberculosis, or scorpuloderma, is a secondary skin lesion. Children are characterized by hematogenous forms that develop in connection with tuberculous lymphadenitis and osteoarticular tuberculosis, or skin lesions near the tuberculosis focus in the underlying tissues (lymph node, bone).
A nodular or gummous infiltrate appears in the subcutaneous adipose tissue and dermis. Subsequently, it fuses with the skin, softens, the surface acquires a purplish-red color, and the infiltrate is opened. One or more fistulas and ulcers are formed, located in the area of purplish-red edematous tissue, permeated with purulent passages. In other cases, the affected surface is represented by an extensive irregular ulcer. , with thin red edges, a granulating bottom and copious purulent discharge. The ulcerative surface can spread to large parts of the face. With a long course of the disease, typical rough scars rising above the surface are visible along the edges of the ulcer.
- Tuberculous lupus
Tuberculous lupus is classified as a secondary lesion of the face. The pathological process is localized mainly in the nasal and oral cavity. First, separate and then merging tubercles appear on the skin - lupomas. They have a typical yellowish-pink or purple color. The surface of the affected area is slightly raised, at first smooth, then it ulcerates. Merged lupomas form an infiltrate of a very soft consistency, into which the finger seems to be immersed (“probe symptom”) The soft consistency of the infiltrate is the result of the breakdown of connective tissue and elastic fibers The coloring of lupomas and their softness serve as pathognomonic symptoms of tuberculous lupus
Tissue damage in lupus can remain superficial, without ulceration, and end in self-healing with an atrophic scar. In other cases, the resulting ulcers expand and deepen into the underlying tissue, which leads to severe disfigurement of the face. The process can develop according to the hypertrophic type. In this case, on the face in the area of the nose or earlobe, conglomerates of edematous, granulating, ulcerated soft tissues of a purple color are formed. New nodules are formed on the periphery, which ulcerate and merge with the main lesion. A characteristic sign of lupus is the appearance of new elements on the scars. The disease lasts for years.
With lupus of the skin, lesions of the oral mucosa are often found. Lupus can also develop primarily on the mucous membrane with localization on the red border of the lips, cheeks and gums, uvula, soft palate, palatine arches. The evolution of the disease involves three phases: initial lupous infiltration, lupous granulation and tuberculous ulcer. At the height of the disease, all three manifestations are determined. The general condition of children with secondary manifestations of tuberculosis in the maxillofacial area changes little. Body temperature remains normal. Symptoms of severe intoxication are observed only with primary damage. The temperature rises to 39-40 ° C.
The diagnosis of tuberculosis is made on the basis of anamnesis, clinical picture, dynamics of the process and a number of laboratory tests. Tuberculosis of various organs in a child gives reason to think about secondary manifestations of the process in the maxillofacial area. Contact with patients, consumption of milk from infected livestock, damage to the integumentary tissues may be prerequisites for primary damage to the tissues of the maxillofacial area.
Significant assistance in diagnosis is provided by microscopic examination of smears of pus, the contents of ulcers, cytological examination of punctates, biopsy of material
Tuberculosis tests are positive in a state of well-defined allergy, that is, with secondary lesions. With primary lesions, especially at the beginning of the process, they are of less importance.
Diagnostics
Primary tuberculosis of the oral cavity is diagnosed during an external examination. Thus, it is characterized by the presence of lacerations and ulcers in the corners of the mouth with yellow, gray and bluish layers. Areas with ulcers tend to gradually enlarge.
At the same time, the lymph nodes begin to enlarge.
Diagnosis is carried out on the basis of the collected anamnesis, as well as using histological and bacterioscopic studies. During examination, dense painful lumps or ulcers are found on the mucous membrane, depending on the severity of the condition.
There is minor inflammation. The process of formation of adhesions begins between the lymph nodes and the surrounding surface.
Symptoms
Characteristics of tuberculous lupus are the apple jelly symptom and the probe test. When pressing on the lupoma with a glass slide, the red color, caused by the perifocal dilatation of the vessels, disappears, and the primary elements of the lupoma become visible - yellowish-brown or waxy nodules, reminiscent in color of apple jelly (symptom of apple jelly). If you press on the lupoma with a button probe, it easily falls through (Pospelov's symptom), which is mainly explained by the destruction of elastic and collagen fibers in the tubercle.
In the clinical course of tuberculous lupus of the oral mucosa, four stages are distinguished: infiltrative, tubercular, ulcerative and cicatricial.
In the infiltrative stage, infiltrative processes predominate. The oral mucosa in the affected area is swollen and hyperemic. The primary elements of tuberculous lupus - tubercles - are not yet expressed.
The second stage is characterized by the appearance of small tubercles, which, merging, resemble warty growths.
In stage III, ulceration of the tubercles occurs with the formation of deep ulcers. Against the background of ulcerative tubercular lesions, papillomatous growths often appear, characteristic of the localization of the process on the hard and soft palate.
The fourth, final stage of the process is characterized by the formation of scars. In the absence of a stage of ulceration of the tubercles, smooth, shiny, atrophic scars are formed. After epithelization of ulcerative surfaces in tuberculous lupus, the scars are dense, rough, welding the oral mucosa to the underlying tissues.
Clinical manifestations of tuberculous lupus in various parts of the oral cavity have some features.
When lupus is localized on the gum, the latter infiltrates, becomes bright red, bleeds easily, and is painless. Subsequently, tubercle-ulcerative lesions appear on the gums. In this case, the bone tissue of the alveolar process is quite often affected. A picture of rapidly progressing periodontitis develops. Teeth become loose and fall out. On the red border of the lips, ulcers become covered with bloody purulent crusts. The affected lip swells greatly, increases in size, and painful cracks appear on it. After the process is resolved, a scar remains. If the process proceeded without ulceration, a smooth atrophic scar is formed. In places of ulceration, the scars are dense, rough, and weld the mucous membrane to the underlying tissues. Repeated formation of a lump on the scar is typical. Localization of the lupus lesion on the lip subsequently leads to its deformation, as a result of which eating becomes difficult and speech is distorted. If both lips are affected, microstoma may develop. The course of tuberculous lupus is chronic. Without treatment, the process can continue indefinitely, and fresh bumps appear on the scars. Regional lymph nodes enlarge and become denser.
Tuberculous lupus can be complicated by erysipelas and candidiasis. Malignancy of lupus ulcers on the oral mucosa occurs in 1 - 10% of cases (lupuscarcinoma).
- Miliary ulcerative tuberculosis (tuberculosis miliaris ulcerosa)
Treatment of oral tuberculosis
Treatment of this form, like all others, is carried out in specialized institutions - tuberculosis dispensaries. First of all, the underlying disease is treated. To prevent the bacterial infection from spreading further, antiseptic baths are prescribed.
After the acute condition has been relieved, it is necessary to take care of timely and high-quality sanitation of the oral cavity. It is important to promptly consult a specialist at the first symptoms: advanced oral tuberculosis leads to serious consequences for the patient’s health.
Symptoms and first signs of tuberculosis in children
First of all, tuberculosis in children is manifested by such clinical signs as:
- weakness;
- stopping weight gain;
- irritability;
- fatigue during school hours;
- absent-mindedness;
- lagging behind peers in studies;
- body temperature – up to 37.5°C;
- enlarged lymph nodes;
- sweating;
- chills.Source: N.M. Koretskaya Tuberculosis in children and adolescents in modern conditions // Siberian Medical Review, 2010
Forms of tuberculosis and early signs
| Form | Symptoms |
| Tuberculosis of the bronchial glands | Cough, elevated body temperature for a long time, lethargy, fatigue, pallor, thinness. |
| Pulmonary form | Cough, shortness of breath, weakness after sleep, apathy, decreased performance, absent-mindedness, unhealthy blush, thinness, pale skin, sweating, chills, dry (and then “wet”) cough for more than 3 weeks, sputum with blood. |
| Lymph node involvement | An increase in the size of the lymph nodes, their softening, suppuration (the contents leak out), the formation of fistulas in places where pus comes out, scrofuloderma (skin lesions in the form of tumors with subsequent release of the contents). |
| Involvement of bones and joints in the process | Slow development, pain when moving, changes in gait, lameness. |
| Damage to the meninges (tuberculous meningitis) | Anxiety, lethargy, loss of appetite, bad mood, headaches, fever, vomiting, convulsions. |
| With damage to the gastrointestinal tract | Constipation or diarrhea, increased body temperature, blood in the stool, pain. Source: A.V. Mordyk, E.A. Tsygankova, L.V. Puzyreva, A.A. Turitsa Tuberculosis in children of the Russian Federation at the present stage // Pediatric pharmacology, 2014, v. 11, no. 3, pp. 27-30 |
Clinical manifestations by age of children
| Age | Symptoms |
| Infancy (up to one year) | Low mobility, apathy, weakness, attacks of suffocation or coughing, retraction of part of the chest, weight loss (including muscle mass), loss of appetite, cessation of crying, insomnia. Early detection and diagnosis are extremely important, because at this age this pathology is most dangerous. |
| 5-8 years | Decreased activity, weakness, lack of sleep and appetite, loss of body weight, cough, condensation of the chest. |
| 8-15 years | Rapid appearance of pain in the lungs against a background of apathy and weakness, active urge to cough, shortness of breath even at rest, thinning or discoloration of the skin, the appearance of cracks, wounds, hemoptysis, changes in lymph nodes in size and structure, intoxication of the lungs (at the last stage) . |
Manifestations of the chronic form:
- sleep disorders;
- liver enlargement;
- lagging behind peers in physiological development;
- dry and pale skin;
- mild euphoria.
Treatment
Chemotherapy, antibiotics
Bactericidal and bacteriostatic drugs are used to achieve complete recovery. In this case, the correct combination of drugs is important, taking into account the resistance of some bacteria to this type of therapy. First, treatment is aimed at suppressing the growth of bacteria and eliminating their resistance to medications. Residual infection in the cells is then eliminated. Duration of therapy is 6-12 months.
Surgery
Pulmonary resection is practiced as a radical technique. The operation is performed for bronchial stenosis, fibrous-cavernous lesions, pleural empyema, abscesses in the lungs, tuberculomas prone to progression, etc. In addition, decortication is used, that is, removal of fibrous layers, and cavernotomy - cleansing of the opened cavity.
DOTS
A treatment system consisting of several levels: bacterioscopic examination, chemotherapy, anti-tuberculosis treatment.
Sources:
- N.M. Koretskaya. Tuberculosis in children and adolescents in modern conditions // Siberian Medical Review, 2010.
- A.V. Mordyk, E.A. Tsygankova, L.V. Puzyreva, A.A. Turitsa. Tuberculosis in children of the Russian Federation at the present stage // Pediatric pharmacology, 2014, v. 11, no. 3, pp. 27-30.
- https://www.ncbi.nlm.nih.gov/pubmed/24548085 Marais BJ. Tuberculosis in children // J Paediatr Child Health. 2014 Oct;50(10):759-67. doi: 10.1111/jpc.12503. Epub 2014 Feb 19.
- V.N. Krivohizh. Modern methods of early detection of tuberculosis among children and adolescents // Health is the basis of human potential: problems and solutions, 2013, pp. 570-585.
The information in this article is provided for reference purposes and does not replace advice from a qualified professional. Don't self-medicate! At the first signs of illness, you should consult a doctor.