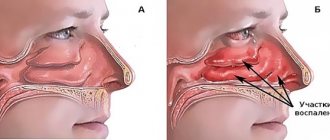
Why is this complication dangerous?
The maxillary sinuses located above our upper jaw (their area extends from the inner corner of the eye to the outer) perform important functions. They can warm the air and thereby protect the respiratory tract from hypothermia and foreign particles. The sinuses are located under the bone tissue and if its thickness is too small, when cleaning the dental canals, filling masses can fall into these cavities. Once the filling is completed, it is no longer possible to remove the foreign material on your own, since this procedure can only be carried out by a specialized specialist who has the necessary tools. The doctor can perform this procedure without difficulty and it will not take much time. It is numbed with local anesthesia and after removing the foreign body from the maxillary sinus, the patient will need to stay in the clinic for several hours. In some cases, discharge occurs the day after this minimally invasive procedure.
Errors when filling
Endodontic treatment is a rather complex procedure. For successful implementation, you should remember three principles: proper processing, high-quality asepsis, reliable sealing.
At each stage, the doctor is capable of making a considerable number of mistakes:
Tooth perforation - in the absence of proper instrumentation and expansion, there is a risk of damaging the wall or bottom of the root canal. This happens, in most cases, due to a poor understanding of the anatomical structure of the roots and cavity of the tooth. Poor machining is the result of incorrect tool size selection. If the diameter of the file or reamer does not match the diameter of the canal, it can damage the apical foramen or leave an accumulation of dentinal filings on the walls.
Perforation of a tooth with a tool
Breakage of an endodontic instrument - this complication occurs when the technique and sequence of using files and reamers is violated, or when a blunt, damaged instrument is used. Breakage can occur during both manual and machine processing. To prevent this type of complication, the doctor should check all instruments before the appointment and make sure they are functional.
A piece of instrument in the channel
Incorrect expansion of the canal and its filling. To achieve high-quality obturation, the canal must be expanded to the optimal diameter. To avoid the formation of voids and further infection, the canal must be given a shape that is convenient for filling with material. Do not forget that canals filled with one paste will not have sufficient sealing, and over time, pores will form in the material.
Why does this complication occur?
Some patients find it difficult to imagine why dental material gets into the maxillary sinuses, and they often blame the doctor for this. However, the reasons for the appearance of this complication during treatment are usually completely different. Foreign material entering the maxillary sinuses occurs during the following dental procedures:
- Canal filling;
- Some methods of dental prosthetics.
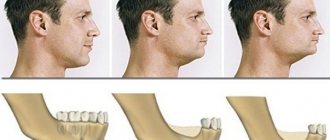
To better understand the essence of the treatment process and see possible ways of penetration of dental material into the maxillary cavities, it is necessary to study the tooth filling scheme. Such a clear example will help you understand that if the layer of bone tissue between the gum and sinus is too thin, damage to the wall of the jawbone can occur. Dental material passes through this small hole. A similar complication usually occurs during dental treatment by a dentist. Another way for filling material to penetrate into the sinuses can be a hole formed when drilling the root canal of a tooth and jaw bone. A similar complication during root canal treatment occurs if the roots and paranasal sinuses are very close to each other. The third option for dental materials to enter the maxillary sinuses is bone tissue augmentation, which is carried out during dental prosthetics. Such additional intervention is necessary for high-quality tooth restoration, and when introducing materials for bone building, damage to the bone tissue may occur, through which pieces of dental preparations will fall.
How does damage to bone tissue in the maxillary sinuses occur?
Looking at the diagram of the anatomical location of the maxillary sinuses and upper teeth, you will notice that there is only a small area of tissue between them. The bones of the upper jaw are especially easily injured during the treatment of second premolars and first and second molars. The likelihood that such damage will occur increases in various pathological conditions and diseases:
- formation and suppuration of cysts in the upper jaw;
- osteomyelitis;
- dental injuries;
- periodontal acute inflammation of the maxillary sinus;
- process of installing prostheses;
- removal of a tooth in the upper jaw, complicated by a suppurative process of the tissues of the upper jaw;
- augmentation of bone tissue of the upper jaw;
- caries complicated by pulpitis.
The severity of the complication associated with the entry of dental material into the maxillary sinuses is increased by the fact that bacteria from the oral cavity can also penetrate through the damaged opening. As a result, some microorganisms can provoke the development of severe purulent inflammation, which will lead to an even greater deterioration in the patient’s well-being and an increased risk of developing even more dangerous complications.
Extension of filling material beyond the apex: endodontic failure versus clinical success
Tags: Errors and complications
Many dentists believe that procedural errors in daily practice, such as extrusion beyond the apical foramen and contact of filling material (most often gutta-percha and zinc oxide eugenol sealer) with periapical tissues after treatment, are a direct cause of endodontic failure.
Some authors show the negative impact of extending the filling material beyond the apex on the predictability of endodontic treatment and emphasize the following:
- High incidence of postoperative pain with exacerbation of inflammation
- Toxicity of materials
- Constant irritation of the periapical tissues with manifestations ranging from mild inflammation to a general reaction of the body.
In contrast, other authors have argued that apex extrusion in itself does not directly contribute to endodontic failure, although it should be avoided. Ingle says that endodontic treatment can be successful despite extrusion of material beyond the root apex. Schilder notes that he has not encountered complications specifically associated with excessive filling of the canal. Weine states that periapical tissues, fortunately, tolerate contact with gutta-percha well and therefore endodontic failure due to its removal beyond the apex is rare. In most cases, there is no pathological radiological evidence, and sometimes there is even a decrease in the amount of excreted material due to phagocytosis.
Image 1 – Mandibular first molar with amalgam filling and insufficient root canal obturation.
After retreatment, the radiograph shows three-dimensional filling of the root canals with a slight extension beyond the apex in the mesial canals obturated with Thermafil #25 and in the distal canal obturated by vertical condensation of heated gutta-percha.
After 5 years, the excess material had disappeared and the periapical tissue remained healthy.
These contradictory results can be explained by differences in research methodology and different composition of the derived materials. In general, the most common causes of discrepancy are related to differences in apical anatomy, limiting the effectiveness of endodontic treatment in various clinical situations.
Image 2 - The main factors leading to the removal of material beyond the root apex:
External inflammatory apical root resorption associated with apical damage to a previously treated tooth.
Incompletely formed root.
Excessive instrumentation with deviation from the natural course of the canal and apical perforation.
Inadequate handling of plasticized or unplasticized gutta-percha and sealants during obturation.
It is extremely important to identify and distinguish between the removal of filling material in three-dimensionally cleaned, formed and obturated root canals and in canals with obstructive overflow in combination with incomplete internal obturation.
Image 3 – Typical view of an exposed gutta-percha point: note the scratches on the point.
Image 4 – The apical foramen is completely filled.
Image 5 – Proper expansion for obturation, but insufficient filling of the canal. Note the transport of the apex during canal formation. (Courtesy of Dr. M. Vitullo).
Image 6 - Postoperative radiograph of the mandibular first molar showing a large apical lesion of endodontic origin. The mesial canals were obturated with Thermafil. A follow-up examination after 4 years shows osteoreparation. Excess filling material did not interfere with bone restoration.
Image 7 – Thermafil carrier extended beyond the apex in the distal root. Thermafil is a good method of obturation if the protocol is followed. The media was removed and the canals were refilled. After 6 months, the lesion was smaller than on the preoperative radiograph, and the patient noted the disappearance of pain when chewing.
Image 8 - These images show that even MTA can be released into the periapical tissue. In this case, the rule is the same as in the previous examples: if the canal is well cleaned, excess MTA cannot interfere with tissue restoration. 6-year follow-up kindly provided by Dr. R. Tonini.
Conclusion
Obturation is the last stage of endodontic treatment. Bringing either sealer or gutta-percha beyond the apical foramen will not necessarily be a mistake when performing obturation. However, this may result in an error in canal formation when parallel canal walls were created instead of conical ones, apical resorption or expansion of the apex.
Therefore, it is necessary to determine the direct causes of excessive root canal filling. “Is the excess material remaining after a complete three-dimensional obturation or is the material brought beyond the apex in combination with incomplete internal obturation of the canal?” Excess material beyond the apex is clearly not the goal of endodontic treatment, but rather the result of safely generated hydraulic forces in achieving three-dimensional obturation of the root canal system.
Numerous cases of root apex removal that have been successful, as evidenced by clinical and radiological signs of long-term restoration of periapical tissues, should reassure patients, doctors and insure against any legal charges.
Source: forum.stomatologija.su, styleitaliano.org
Similar articles:
Ibrahim El Naggar
Huge perforation
Cancellation
The physician must be able to assess the current situation from diagnosis, treatment to prognosis, and be able to cope with various clinical surprises.
Ibrahim El Naggar Read
Jaya Srivastava, Manoj Kumar Hans, Rohit Paul, Amit Kumar Garg, Rhitu Shekhar
Clinical case of perforation treatment using calcium silicate cement and internal matrix
Cancellation
Perforations of the pulp chamber floor can occur due to caries, iatrogenic trauma during access creation, orifice preparation, pin space preparation, or during removal of broken instruments.
Jaya Srivastava, Manoj Kumar Hans, Rohit Paul, Amit Kumar Garg, Rhitu Shekhar Read Giovarruscio Massimo
Lower second molar: obturation with a canal filler... through the bifurcation
Cancellation
The prognosis for closure of perforations has improved significantly over the past two decades, with the use of MTA and similar cements becoming the gold standard.
Giovarruscio Massimo Read Solomonov Mikhail
Broken Instruments - Clinical Decision Making Algorithm
Cancellation
Breakage of endodontic instruments during root canal treatment is a complication that every endodontist faces. The incidence of broken instruments is reported to range from 0.7% to 6% of cases.
Mikhail Solomonov Read Yoshitsugu Terauchi
Retrieving Broken Files
Cancellation
Ni-Ti files break preferentially in curved or narrow canals of the apical third due to their superelastic properties.
Yoshitsugu Terauchi Read
Solomonov Mikhail
The author's view on the problem of broken tools
Cancel
This article presents the author's view of Dr. M. Solomonov on the problem of broken instruments from a biological point of view.
Mikhail Solomonov Read
Belograd Maxim
Endodontics without rules
Cancel
Looking at such “endodontics”, you ask the question: what had to be done to get such a final result? Let's deal with this dilemma.
Belograd Maxim Read Marc Kaloustian
Finding and bypassing a step using Explora tools after removing pieces of a broken tool
Cancellation
This clinical case will describe in detail the technique of restoring tooth 1.7 with a broken instrument in the mesiobuccal canal and a step in the middle of the root canal.
Marc Kaloustian Read Viresh Chopra
Endodontic treatment of the second lower molar
Cancellation
The article presents a case of irreversible pulpitis with symptomatic apical periodontitis of the mandibular second molar.
Viresh Chopra Read Daniel Flynn
Repeated endodontic root canal treatment: pros and cons
Withdrawal
Repeat root canal treatment is a predictable endodontic procedure. In the past, when telling patients about the prospects of retreatment, doctors often pointed to the possibility of failure.
Daniel Flynn Read L. Stephen Buchanan
Obturation using the continuous wave method for greater precision of the procedure
Cancel
I invented the Continuous Wave Obturation Technique (CWOT) in 1986 and continued through the winter of 1988-1989. I used it in combination with the Touch'n Heat device (SybronEndo).
L. Stephen Buchanan Read Mohamad Zaafrany
MB2: The Most Famous Missed Channel
Cancellation
Missed canal is one of the main causes of endodontic failure. During root canal treatment, MB2 is most often not found among the maxillary molars.
Mohamad Zaafrany Read
- ‹
- 1
What symptoms may indicate a foreign body in the maxillary sinuses?
After dental treatment, a person may suspect the development of this complication if the following signs appear:
- the appearance of pain when performing light taps on the facial bone under the eyes near the nose;
- severe, aching headache;
- prolonged and persistent runny nose;
- aching pain in the upper jaw, aggravated by chewing.
One of these symptoms or a combination of several may indicate that dental medications have entered the maxillary sinus cavity. This condition is a reason for mandatory consultation with a doctor and the visit should not be postponed. If the patient does not see a doctor on time or has a weakened immune system, the disease becomes more complicated. Because of this, a person develops thick, purulent and profuse nasal discharge with a specific odor. In addition, the progression of the inflammatory process causes an increase in temperature and a deterioration in general health. In some cases, immediately after dental mixtures enter the sinuses, inflammation does not develop. However, this condition is also unsafe for his health in the future, since various negative factors (for example, hypothermia, stress, injury or hypovitaminosis) can provoke the development of inflammation and a deterioration in general well-being.
The cause of toothache is defects in canal filling
The most common cause of toothache after nerve removal is defects in filling the tooth canals. It is not always possible for a dentist to completely fill the cleaned canals of a tooth. Often, the desire not to leave voids in the tooth canals leads to squeezing out the filling material beyond the root.
Correct canal fillingA normally filled tooth canal during the treatment of pulpitis | Underfillingtooth canalThe filling material does not reach the root apex (to the end of the canal) | Refilling a tooth canalFilling material extends beyond the root of the tooth |
Why does a tooth hurt when it is not filled?
Underfilling does not cause pain immediately. The pain may appear after a month or even several months. A focus of infection forms in an empty, unfilled canal. Over time, the infection extends beyond the root tip and causes periodontitis (inflammation of the periodontium - the tissue behind the root tip). Then a cyst grows in this place. This, of course, can cause aching and even acute toothache and swelling.
Why does a tooth hurt during refilling?
More often, pain occurs during prefilling. The filling material rests on the bone tissue, puts pressure on it and causes pain.
What to do if a tooth hurts after nerve removal?
If the pin goes beyond the root of the tooth, you need to open the filling, clean the canal again and refill it.
If root cement has escaped beyond the tooth root, it is necessary to estimate how much material has escaped. If a lot of material has come out, then you will also have to unseal everything, expand the top of the canal and wash out the old cement, and then refill the canal and seal it. If a little material comes out, then it makes sense to wait - most likely the dental material will resolve.
Features of the immune system and toothache
The reaction to the shortcomings of root canal filling is very individual and depends on the characteristics of the person’s immune system.
Many patients come to our center. And in some photographs, the canals are half sealed, but no inflammation occurs. The human immune system copes 100%. For others, the slightest underfilling of the canal causes inflammation and pain.
The cement that comes out of the canal in some patients quickly resolves and does not cause problems, while in others it comes out just a little and immediately hurts.
How can a complication be identified?
External signs of dental materials getting into the maxillary cavities and patient interview data may not be enough to make a correct diagnosis, and additional studies are carried out to confirm complications of the dental procedure:
- x-ray of the maxillary sinus;
- MRI;
- CT;
- puncture.
The diagnostic plan may include several procedures. Their number is determined by each doctor individually.
What dangerous consequences does a foreign body lead to?
A foreign object in the maxillary sinuses can lead to the following complications:
- bacterial or fungal sinusitis;
- encapsulation in the form of a cyst or other benign disease;
- granuloma formation.
In more complex cases, suppurative processes in the maxillary sinuses cause the development of the following complications:
- frequent colds and inflammation of the nasal cavity and sinuses;
- meningitis;
- hypertrophy of the mucous membrane;
- damage by coccal flora to other organs and systems (for example, heart muscle).
A particularly dangerous complication is inflammation of the meninges. When meningitis develops, the patient develops the following symptoms:
- significant increase in temperature;
- headache in the forehead;
- frequent vomiting that does not bring relief;
- rash on palms and soles.
If these symptoms appear, you should immediately consult a doctor!
And the possible consequences of getting filling materials can only be prevented by timely consultation with a doctor and regular preventive examinations in the mode prescribed by the doctor.
Available information about root canal treatment…
In one of the previous posts, I tried to talk about what caries treatment should look like at the modern level. Now it’s time to talk about another most common procedure - root canal treatment.
The need for such treatment arises when an infection from a carious cavity reaches the dental pulp, causing its irreversible inflammation - pulpitis. In this case, the only treatment option is its removal from the root canals - depulpation. The second diagnosis that forces the doctor to go so deep is periodontitis. This inflammatory process no longer occurs inside the root canals, but around the roots of the tooth, in the periodontium, causing destruction of bone tissue (and the consequences of this are clearly visible on x-rays). I deliberately do not dwell in detail on the terms, because... On the Internet you can find quite a lot of reference articles of varying degrees of abstruseness about these diseases, their causes, symptoms, varieties, methods of treating these varieties.
It is enough to make a request using the keywords “pulpitis” and “periodontitis”. And I would like to dwell in more detail on the main manipulation that a dentist has to perform in case of these diseases - canal treatment (endodontic treatment). At the same time, I will try to briefly highlight the general principles and methods of treatment that will help you see how competently and modernly your dentist carries out this treatment. This is important, since the consequences of poor-quality manipulations in the root canals directly lead to tooth loss ahead of time.
If you try to outline the standard modern protocol for any endodontic treatment, then in abbreviated form it will look something like this...
First, the doctor makes access to the canal(s) of the tooth. In different teeth there are usually from 1 to 4...sometimes more. In this photo there are two holes in the corners of the tooth cavity - these are the entrances to the root canals
Then the canal is gradually expanded with thin flexible instruments and simultaneous mechanical removal of pulp residues
At the same time, the canal is washed generously with various preparations, primarily with bleach (sodium hypochlorite in a concentration of 3 to 5%)
The canal is also cleaned with ultrasound
After the canal has been sufficiently washed and expanded, it is filled with gutta-percha and a small amount of special paste.
Next, the tooth is restored using the method that is best suited for the specific clinical situation.
So, the main markers of high-quality root canal treatment.
1. Use of rubber dam.
The rubber dam helps the dentist to reliably and hermetically isolate the oral cavity from the tooth being manipulated. Why is it important? During the expansion of the canals, the doctor must rinse the canal abundantly with bleach (I will write why and why below). This is a fairly strong caustic drug and if it comes into contact with the oral mucosa, it can cause a serious chemical burn. In addition, one of the goals of tooth canal treatment is to reduce the amount of microflora in the tooth canal to a slight minimum. If the tooth is poorly isolated from the oral cavity, then it is possible that infected saliva will get there during treatment, which means that the effectiveness of treatment will greatly decrease and complications are possible in the future. For this reason, it is especially difficult to do without a rubber dam when treating the canals of the lower lateral teeth .
Without a rubber dam, it is very difficult to practically treat canals according to all the rules.
2. Copious rinsing of the canals with bleach.
This process can always be felt by the characteristic smell of this drug. Why is this point important? The essence of any endotherapy is to clean the canal system from organic residues (i.e., pulp residues) as efficiently as possible. Because they are the substrate for microflora nutrition. If organic “dirt” remains in the channel and then becomes clogged, then ideal conditions are created for the development of “bad microbes” - there is food, there is no destructive oxygen, which means prosperity for the “microworms”. But the body is forced to react to this with inflammation. This is how granulomas and cysts develop over time. So about bleach and the importance of its use... Large fragments of pulp are removed by mechanically expanding the canal with metal “needles” - files. Small fragments are removed just when the canal is washed. In addition, it is sodium hypochlorite that “knows” how to dissolve the smallest fragments of organic residues. Not immediately, not instantly... but within 40-60 minutes of constant use of “bleach” in one channel, everything completely dissolves without a trace. If the dentist does not do this, then “minced meat” will remain on the walls of even a well-expanded canal, which the microflora will happily feed on, causing a chronic inflammatory process in the bone around the tooth.
Abundant and frequent rinsing of the canals with sodium hypochlorite for 40-60 minutes guarantees complete removal of organic residues, and therefore a good long-term prognosis for the tooth.
3. Ultrasonic cleaning of canals.
This process occurs in parallel with washing the canal with bleach. Using a special tip, the dentist periodically activates the solution directly in the tooth canal. The ultrasonic tip vibrates at high frequencies, creating turbulence in the solution, which is much better at removing organic debris from the dental canals. In fact, it all works on the principle of an ultrasonic cleaner. Thus, working with ultrasound makes it possible to reduce the exposure of the solution in the tooth canal to completely clean it of organic matter to 30-40 minutes. At the same time, the importance of using ultrasound is also due to the fact that the canals in teeth have a complex structure. From the main large canal, which can be washed and cleaned instrumentally, many smaller ones (like branches on a tree), sometimes microscopic, branch off. No tool can get through there. The only way to clean them is to drive “bleach” there with ultrasound to wash out even the microscopic remains of the pulp.
| This is a photo of a river delta taken from space. Very often, an identical picture can be seen if you examine the root tip under a microscope - many small branches extending from the main canal. They can be cleaned of pulp residues only through the combined use of bleach and ultrasound for at least 30-40 minutes per channel. Otherwise, the risk of developing chronic inflammation (granulomas, cysts) over time increases significantly | This three-dimensional model of the structure of the canals of a multi-channel tooth shows that at different levels there are small branches that cannot be cleaned only mechanically using instruments | 4. Control of work using x-rays and apex locator. The final goal of the doctor during endotherapy is to expand, clean and fill the entire length of the tooth canal, exactly to the apex. At the same time, it’s bad if there is an “overshoot” or “undershoot.” How to correctly determine the exact length of the channel and why is it important? “Overshooting” or penetration of the filling material beyond the top of the tooth into the surrounding bone is undesirable, because can lead to various complications. An “undershoot,” a tooth that is not filled to the top, most often leads to the appearance of granulomas and cysts, because an untreated zone remains in which “bad” microflora settles. How to accurately determine the length of the channel? To do this, the dentist uses X-rays and/or (preferably “and” is definitely better) an apex locator. I think everything is clear with x-rays; many have encountered it. The dentist inserts an instrument into the canal, marks the length on it and takes a picture. After that, he can objectively adjust this length. An apex locator is a very convenient device, a sort of endodontic parking sensor. It is connected to an instrument with which the doctor expands the canal, and when the tip of the instrument approaches the apex of the root, it begins to squeak, the closer, the more intense... just like the parking sensors in a car. In this way, the dentist can control the immersion depth of the instrument in real time with an accuracy of fractions of a millimeter. Moreover, the first apex locators lied quite strongly, especially if the canal was not dry... Modern devices give very accurate results, practically minimizing the need for constant use of x-rays. However, the gold standard of endodontics is the use of an apex locator throughout the entire treatment, plus 3 x-rays for each tooth: status before treatment, during (usually with instruments or pins immersed throughout the entire length of all canals), after completion of canal treatment and tooth restoration. Moreover, the role of these photographs is rather documentary. |
How is a foreign body removed from the maxillary sinus?
To prevent the development of complications in the presence of foreign objects in the maxillary sinus, minimally invasive surgical intervention is performed. Its main purpose is to remove filling material. The operation can be performed using optical instruments such as an endoscope or laparoscope. When carrying out such interventions, significant trauma to bone tissue and incisions is not required. These minimally invasive operations are pain-relieved with local anesthesia and take no more than half an hour. Traditionally, endoscopic techniques are used to remove foreign bodies from the maxillary sinuses. To perform the operation, a small incision is made above the upper lip through which an endoscope is inserted. This optical device helps the surgeon detect a foreign body. The dental material is then removed. When performing laparoscopic surgery, tissue puncture is performed in the place where the bone tissue is thinnest. A special instrument is inserted into the laparoscope, which captures and removes the foreign particle. This technique is used in cases where endoscopic intervention cannot be performed for some reason. Sometimes operations are supplemented by such manipulation as curettage. This method is necessary in cases where, due to the filling material, a granuloma has formed on the tissues of the cavity. After surgical removal of a foreign particle, the patient is prescribed anti-inflammatory drugs to prevent inflammatory and purulent processes. To achieve the desired result, antibiotics, immunostimulants and other drugs may be prescribed. In addition, the affected sinus is washed with antibacterial, antiseptic and anti-inflammatory solutions. To increase the protective functions of the body, the patient is prescribed vitamin and mineral complexes. The best prevention of such complications is regular visits to the dentist. In addition, it is necessary to exclude facial injuries, try to avoid stress, eat right and lead an active lifestyle.
Endodontic sealers brought out beyond the apex: their fate and impact on the outcome of treatment
Author: Domenico Ricucci
Keywords:
endodontic sealers, endodontic treatment, excess filling, treatment result
Introduction:
This retrospective study examines unintentional leakage of filling material and its impact on treatment outcome.
Methodology:
The study included 105 teeth treated by one specialist and showing signs of removal of the filling material on post-obstruction radiographs. Sealers used: Pulp Canal Sealer (Sybron Dental, Orange, CA), PCS Extended WorkingTime EWT (Sybron Dental), Tubli-Seal (Sybron Endo), Endomethasone (Septodont, Saint-Maur-des-Fosses, France), AH Plus ( DeTrey GmbH, Konstanz, Germany), and Apexit (Ivoclar Vivadent, Schaan, Lichtenstein). Control radiographs were compared with radiographs after immediate obturation, assessing the removal of excreted material and the condition of the periradicular tissues.
Data were divided into 1-year, 2-year and 4-year follow-up groups and statistically analyzed using the chi-square test and Fisher's exact test.
Results:
statistically significant differences were found only in the 1-year follow-up group when comparing Tubli-Seal with AH PlusApexit and Endomethasone (P < .05). Complete resolution rates of AH Plus and Apexit were significantly lower compared with other sealers (P < .05) at two-year and four-year follow-up. No other significant differences were found between groups. When examining the effect on treatment outcomes, there were no statistically significant differences between sealers in all study periods (P > .05). The 4-year follow-up results show that 79% of teeth with apical periodontitis were treated compared with 100% of teeth without apical periodontitis (P < .01).
Conclusions:
not all sealers are predictably removed from periradicular tissues. The treatment result does not significantly depend on the type of sealer produced. A significantly better result was obtained when treating teeth without signs of damage compared to teeth with apical periodontitis.
The main purpose of root canal obturation is to prevent fluid from the periradicular tissues or saliva from entering the canal, as well as bacteria with their virulence factors and antigens from the canal into the periradicular tissues. Ideally, the filling material should be limited to the intra-root space. Research shows that the greatest success of endodontic treatment is achieved in teeth with a root canal filling 0–2 mm shorter than the radiographic apex, and cases with underfilling or overfilling show significantly poorer results.
However, in some circumstances it is not possible to control the filling material and little extrusion of the material occurs. In addition, the use of filling techniques using thermoplastic gutta-percha is also associated with a high rate of removal of the filling material. Once excreted, the fate of the material depends on its solubility and ability to phagocytose, while the effect of the material on treatment outcome depends on its biocompatibility. It is assumed that the lower treatment success rates associated with the removal of the filling material are the result of its cytotoxicity or the body's reaction to certain substances in its composition.
However, the data shows that