Crossbite
It can occur in both children and adults. It is a horizontal intersection of the dentition or jaws.
It is strongly expressed visually, which brings moral discomfort. Occurs when there is a discrepancy in the development of the lateral parts of the jaws. There are both one-sided and two-sided.
Transversal malocclusions (crossover) are divided into lingual, palatal and buccal.
- Lingual bite is characterized by a displacement of the jaw towards the tongue.
- Palatinal - the jaw is shifted towards the palate.
- Buccal - displacement is observed towards the cheek.
This anomaly occurs for a number of reasons. Among the main ones it is worth noting: traumatic factors, lack of teeth in the dentition, pathologies of the temporomandibular joint, disruption of the teething process.
The most common complaints with crossbite include:
- aesthetic defect;
- problems with chewing food;
- slurred speech;
- frequent gum injury.
How to identify malocclusion
In most cases, malocclusions are easily recognized by an experienced doctor during a routine visual examination. But there are situations when part of the row has not yet been cut through. In this case, additional examination may be required to find incorrect teeth and determine whether there is any risk of developing serious pathologies.
Teeth that have not fully erupted are called impacted. Read in detail about them in our article: “What are impacted teeth, why do they appear and how to treat them...”
Malocclusion in adults and children is diagnosed using the following research methods:
- panoramic photograph of the jaw;
- CT scan of the jaw;
- teleroentgenogram (TRG image).
The listed materials provide an experienced doctor with enough information to identify bite problems and create an up-to-date treatment plan.
Different types of bite studies
Sagittal bite
Sagittal malocclusions are often combined with transverse ones. They are characterized by displacement of the jaws in relation to each other. This may be an overdeveloped lower jaw and an underdeveloped upper jaw and vice versa. Such pathologies are divided into mesial and prognathic.
In the first case, a noticeable protrusion of the upper jaw can be observed. The lower one is noticeably underdeveloped, which causes significant deformation of the face in the form of a sloping chin.
In the second case, the lower jaw is noticeably protruded, which causes a significant disproportion.
Such anomalies arise due to a different number of teeth in the jaws, pathology of the development of the alveolar processes, or pathologies of another similar type.
With such defects, the patient experiences difficulty in eating and there is blurred speech. Due to the incorrect position of the jaws, a constantly tense facial expression occurs.
The defect is eliminated in childhood (up to 11 years) with the help of modern technologies, in adults, especially in advanced cases, through surgical intervention.
What kind of bite should a person have?
Physiological or normal occlusion has the following characteristics:
- all teeth of the upper and lower jaws are in contact with each other, with each tooth intersecting with two antagonists. The exception is the third upper molar and the first lower incisor;
- the midline of the face passes between the central incisors;
- there are no gaps between individual elements of the rows;
- The upper dental arch has the shape of a semi-ellipse, the lower - a parabola.
Correct bite on the sides and front
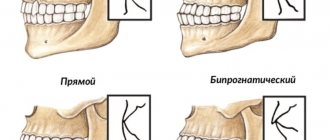
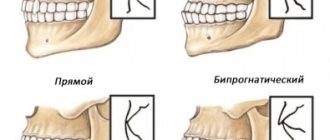
There are also several types of slight changes in the ideal bite, which, although different from each other, do not require correction:
- orthognathic. The upper incisors overlap the lower ones by a third;
- progenic. The lower jaw is slightly protruded;
- straight. The incisors meet with cutting edges;
- biprognathic. The incisors are inclined towards the vestibule of the mouth, but continue to close.
There are three types of normal occlusion, which replace each other over time:
- Temporary. This is what dentists call baby teeth in children.
- Removable. This is a condition of occlusion when some of the baby teeth have been replaced by permanent teeth, and some are still present.
- Constant. All teeth changed from baby teeth to molars.
Problems with a person’s bite can appear at any stage, but baby teeth are much more susceptible to influence: both negative and positive. That is why the process of treating abnormalities in childhood is faster and easier.
Children's bite defects
According to statistics, approximately 70% of children have malocclusions. Most of them require treatment using complex techniques. Specialists experience significant difficulties when working with children. This is due to the attitude of young patients towards the event. They do not always follow doctors' recommendations, which is why treatment is ineffective.
About a third of children do not receive the necessary therapy, which subsequently causes a relapse of the disease. Bite pathologies in school-age children are in most cases accompanied by numerous carious lesions of the teeth, as well as various concomitant diseases, such as periodontal disease. Therefore, treatment must be carried out on time.
Important! Orthodontic diseases in children require long-term treatment. On average, it lasts from 10 months to one and a half years. During this period, you must carefully follow the doctor’s recommendations and come for scheduled examinations on time. They are necessary to evaluate treatment results and correct methods.
Malocclusions in children are classified into 5 types:
- cross;
- deep;
- open;
- mesial;
- distal.
Cross occurs due to unilateral or bilateral underdevelopment of the jaws. As a result, the dentition overlaps.
A deep bite appears due to underdevelopment of the lower jaw. As a result, the upper row of teeth significantly overlaps the lower one.
An open bite is characterized by non-occlusion of the dentition over a significant segment. This pathology can appear both in the front and side of the jaw.
Mesial occlusion is characterized by an overly protruded lower jaw, which causes significant overlap of the upper dentition.
With a distal bite, the upper jaw is pushed forward, which causes the effect of a slanted chin.
All these types of malocclusion in preschoolers have certain causes. The main factors influencing the development of the jaws and the formation of the dentition are:
- Genetic factor.
- The presence of chronic diseases accompanied by difficulty in nasal breathing.
- Habit of thumb sucking and lip or tongue biting.
- Late weaning from the pacifier.
- Lack of calcium in the body.
- Injuries and damage to teeth and jaws.
- Numerous carious lesions.
- Extracting baby teeth too early or too late.
Important! Bite pathologies in children should be treated as early as possible. An advanced disease can lead to significant complications, as well as problems with chewing and speech.
What is the impact of malocclusion in childhood?
As a rule, children are more relaxed about their appearance than adults, so the aesthetic side of the issue worries them to a lesser extent. However, there are a number of other points that are affected by problems of the dental system. For example, incorrect positioning of teeth and jaws at a very early age inevitably affects the formation of a permanent bite. If measures are not taken in time to solve the problem, in the future the child may experience disruption of the functioning of the masticatory-speech apparatus. All this, in turn, leads to malfunctions of the digestive, respiratory and cardiovascular systems, as well as other equally serious consequences.
Tests to determine malocclusion
When diagnosing bite pathologies, specialists use various research methods. There are already developed tables with which you can identify even minimal deviations and prevent its development at an early stage.
Tests for malocclusion are performed both by direct examination and by dental impressions. In the process, measurements are taken in various planes, and attention is paid not only to the dentition as a whole, but to the presence and location of each tooth, as well as their general condition.
Important! Even if there is no visually noticeable bite pathology, it is imperative to visit a specialist and undergo testing. It will help identify the development of anomalies at the initial stage, when deviations are minimal.
Consequences of malocclusion
Each age has its own critical effects that incorrect teeth can have on the human body. But while in an adult the influence is often unnoticeable, in a child it can lead to developmental anomalies in many systems and organs. That is why it is important to remember what will happen if the bite is not corrected, and to deal with the problem in a timely manner.
Temporary
The temporary bite is formed from 6 months to 6 years. The process usually takes place in two stages: first, the primary teeth erupt. With proper development of the child, this stage ends around 3 years, after which active growth of the jaws begins. This period is a kind of preparation for the eruption of permanent teeth.
Abnormal development of the upper and lower jaw
Incorrect temporary bite usually occurs due to disturbances during pregnancy, birth injuries and poor heredity. Problems also appear if the child does not want to give up the pacifier, replaces it with a finger in the mouth, or has breathing problems.
The most important consequence of malocclusion of primary teeth is underdevelopment of the jaws. The child's body simply does not understand what size they should be and stops jaw growth too early. There is also the opposite case, when the oral apparatus turns out to be overly developed and massive. If left untreated, the problem will cause permanent teeth to erupt improperly.
Removable
A mixed bite is called a removable bite, in which some of the baby teeth have not yet been replaced by permanent ones. There is an early mixed dentition, which is formed at 6-9 years of age. The first to be replaced are the molars, and behind the baby teeth the first permanent molars, the “sixes,” appear. Late mixed dentition begins to form at 10 years of age. At this age, premolars and canines grow. With a correct change of bite, the permanent teeth do not come into contact with the milk teeth and quickly take their place.
Irregular eruption of permanent teeth
Dental disorders in the mixed dentition are caused by elements that fall out or are removed too early: they leave cavities and gaps, which is why the formed permanent teeth grow without the correct orientation. This can cause twisting, incorrect placement of teeth in space and other problems. This is why baby teeth need to be treated rather than removed.
Constant
At the age of 12-15, a person’s milk teeth are replaced by permanent ones, and most of the molars, except for the “eights,” also grow. At this age we can talk about a fully formed permanent dentition. If baby teeth grow correctly, we can hope that the molars will also be positioned correctly. Although this is not a guarantee, this is often the case. But, if a person has developed an incorrect bite, the consequences cannot be avoided.
Decreased chewing activity
Malocclusion almost always leads to a decrease in chewing activity. The teeth do not touch each other, so a person simply cannot provide sufficient force to chew food. He makes a lot of movements without getting the desired result, and as a result, he often refuses to chew properly at all. Because of this, large pieces of food enter the stomach, which are difficult for the body to process; a person does not receive enough nutrients from food.
Temporomandibular joint disease
The temporomandibular joint is one of the most mobile in the human body. But it also cannot withstand too much stress. If the teeth are positioned incorrectly and the chewing function is impaired, overload cannot be avoided. Also, improper bite of the teeth causes disturbances in movement in the joint, the appearance of clicks, and pain. In the most negative version, the TMJ becomes completely stuck: the person opens his mouth, but cannot close it.
Uneven chewing load on teeth
One of the signs of a correct bite is an even load on the teeth. When chewing, each molar and premolar performs its function by cutting or grinding food particles. The absence of an element in the dentition or their weak contact leads to the fact that one tooth “works” and the other does not. This is especially noticeable in an open bite.
Increased enamel wear
Uneven loading invariably leads to frequent use of the same tooth surfaces. Because of this, the enamel suffers, which is damaged in certain places and begins to wear off faster. Weakening and abrasion of enamel almost always causes tooth disease.
Damage to bone tissue
Damage to bone tissue is almost always caused by the absence of one of the elements in the bite. If there is no tooth, the load that it took upon itself falls on the bone. Due to the formation of the cavity, chewing mainly occurs with adjacent molars or canines, but such disorders also have a great impact on bone tissue.
Periodontitis
Gum inflammation is almost always associated with a malocclusion. And the stronger the disorder, the more often inflammation will occur. They are especially familiar to people who have crooked teeth. Periodontitis can also occur due to constant damage to the gums by food or adjacent elements of the dentition.
Early tooth loss
It is possible to lose teeth early even with a normal bite, but due to increased wear of the enamel, the risk of developing caries and other diseases increases. This leads to early destruction of the crown, and even to inflammation of the pulp.
Impaired diction
Diction disorders due to malocclusion are usually associated with the fact that a person cannot ensure the necessary passage of air through the oral cavity. But it is precisely this action that makes it possible to pronounce some sounds correctly. If there is no barrier in the form of teeth, speech sounds incorrect.
Aesthetic violations
While a small deep bite may not be noticeable, a cross bite is immediately visible and looks very unaesthetic. Violations extend not only to the teeth hidden in the mouth, but also to the facial skeleton. Facial asymmetry is a common consequence of malocclusion.
Gastrointestinal diseases
Gastrointestinal diseases most often occur after a long life with dental disorders. The problem is related to insufficient chewing of food. The gastrointestinal tract has to take on the function of teeth, processing too large pieces of food. This leads to rapid wear and tear of organs.
Difficult oral hygiene
Uneven teeth are very difficult to clean. Due to the appearance of too small or too large gaps between the teeth, cavities appear that are inaccessible to the brush, where bacteria accumulate. Only an irrigator or dentist can help ensure an adequate level of hygiene.
Difficult prosthetics and restoration
Most orthodontic surgeries are simply not performed for malocclusions, as there is no point in them. Tooth restoration is available, but chewing disorders and excessive stress will lead to rapid wear of the prosthesis. That is why most dentists first recommend correcting the bite, and then doing restoration.
Breathing problems
The airways are located in the lower jaw area. If it is displaced, then the person cannot breathe fully. This can cause snoring and even nighttime breathing apnea.
Bruxism
Bruxism is excessive clenching of teeth and grinding. It occurs due to problems with the temporomandibular joint, as well as if the dentition is positioned incorrectly. Bruxism is a complex problem and can occur for other reasons, but malocclusions cause it quite often.
ENT diseases
The appearance of various ENT diseases is usually associated with constant inflammation in the oral cavity. Both systems are nearby, so inflammatory processes in the mouth quickly spread to the nasopharynx. And they appear in the mouth due to lack of care and a good environment for the development of bacteria.
Traumatization of soft tissues of the oral cavity
Soft tissue injury usually occurs if one of the teeth is positioned incorrectly. It can be moved forward or to the side. The sharp edge often scratches the mucous membrane, causing non-healing abscesses to appear on it. The problem can be solved locally: just sharpen the tooth.
Gum recession
Gum recession is the exposure of the root portion of the tooth. It usually occurs due to improperly distributed chewing load. Because of this, the teeth themselves become much more sensitive, and inflammation occurs.
How to prevent bite pathologies
To prevent the development of anomalies, you need to follow a number of simple rules:
- During pregnancy, you need to carefully monitor your health and eat foods rich in calcium.
- After the birth of a child, do not transfer him to artificial feeding unless necessary. Bottle feeding affects the formation of the bite.
- After teething, monitor their condition and visit the dentist on time.
- Do therapeutic exercises that provide the necessary load on the facial muscles.
Prevention of malocclusion is necessary for both children and adults. Pathology can manifest at any age if appropriate factors are present. Therefore, regular examinations are necessary. If a specialist identifies a predisposition to the development of a certain disorder, he will recommend appropriate means of preventing malocclusion.
To prevent the disease, more complex measures may be needed than therapeutic exercises and compliance with a number of the rules described above. In some cases, you will need a set of devices for the prevention of malocclusions, which the doctor will select depending on the situation.
You cannot use devices to prevent malocclusions on your own, only on the recommendation of a specialist. Their unsystematic use can significantly worsen the current condition and provoke the development of pathology.
How to correct an overbite
Modern dentistry has come up with dozens of ways to correct malocclusion. Most often, braces are used, followed by retainers to prevent teeth from moving apart. Other adjustment methods:
- wearing trainers;
- use of records;
- aligners and aligners;
- surgical intervention.
An orthodontist is involved in the treatment of malocclusion, about whose work we wrote a separate article. Read more about treatment and diagnostics here: “What an orthodontist treats: what diseases does this doctor treat…”
Advantages of treatment with us
| Traditional approach | Our (integrated) approach |
| The goal of treatment is “to turn a malocclusion into a correct one” | The goal of treatment is not simply to “correct the bite.” The art of an orthodontist is to correctly close the “aligned” teeth, taking into account all the characteristics of the patient’s body (posture, etc.). After all, a bite (closing of teeth) is essentially a kind of “lock”. And in this regard, it is important - which patient (with what posture, for example) we will “clog” with a new bite.” |
| Relying on the fact that the device (for example, braces) will correct the bite itself | We don't rely only on equipment. It is not she who treats, but the doctor (braces are just a tool). |
| The work is most often done “by eye”, without proper diagnostics. And without a diagnosis (“bad bite” is not a diagnosis, it is a consequence of the problem). | We always find out the cause; we have a well-established diagnostic algorithm. And we always know what we are ultimately treating (there is a clearly formulated diagnosis). |
| Often there is no treatment plan. | Treatment planning. |
| Working according to the “template”: “put braces on, wear them for a year or two, get results”, in essence, work with the investigation (bad bite). | We work not with the consequence, but with the cause of the problem (anomaly). The cause is always insufficient jaw size. Insufficient jaw size is a consequence of problems with the skull. |
| The root cause remains unidentified and unresolved. High percentage of relapse (the anomaly returns). | Before correcting the bite, we always eliminate the root cause of the problem - we work with the skull and jaws. Therefore, there are no relapses (the problem is eliminated at the root). |
| Work with one device: either a plate or braces. | We are not limited by any limits in the field of hardware treatment. We have a full range of the most modern orthodontic devices in our arsenal. We practice multi-stage treatment. And for each stage there is its own apparatus. |
| Treatment involves the removal of teeth (usually premolars), which often leads to complications. | We do not correct bites with tooth extraction (the percentage of treatment with tooth extraction in our clinic is 0.01%). And not because we are “kind”, we just know how to find an alternative to treatment that involves removing teeth. |
| A large percentage of patients are sent for surgery (orthodontists often do not see a “way out”). | We know how to look for an alternative to surgery (success in 99% of cases). |
| If surgical treatment is necessary, the patient often undergoes surgery without proper preparation, which is fraught with complications. | If surgical intervention is necessary, careful preparation for it (stabilization of the TMJ, development of dentition, support after surgery, etc.). |
| Large prepayments for treatment (the popular scheme is 50% prepayment). No installment payments. | Small prepayments. Each stage (the entire treatment is divided into stages) is paid in installments. A successful treatment access program. |
| Lack of differentiation based on treatment complexity. The cost of treatment depends only on the type of equipment (for example, what kind of braces to treat - metal or aesthetic). | Different amounts of work (treatment) cannot cost the same. Clear differentiation of the cost of treatment depending on the complexity of the treatment and the type of device. |
| Providing “one-time services”: gluing and removing braces, changing the arch, etc. For this reason, it is difficult to predict the cost (no one knows how many and what services will be provided during treatment). | We do not provide “one-off” services. Therefore, do not ask us “how much does it cost to put braces on your teeth” or “how much does it cost to correct a bite in adults?” We don’t “install” - we treat. From and to. We have “package” offers. And the patient always knows the cost of treatment (treatment stage), which is convenient for budget planning. |
| Often there is a lack of prevention: “Come when your teeth grow in, we’ll put on braces and fix it.” And wasting time can be costly. | Prevention (it’s easier to prevent than to fix later). We don’t have a goal to “deliver” anything. We identify the cause of malocclusion and eliminate it at any age. |
Open bite
An overbite is called this way if, during central occlusion, the dentition, it is important to note, not the extreme ones, but the frontal ones, do not close. The cause is shortened central teeth and dentoalveolar long teeth on the sides. This bite can also be horizontal.
Externally it manifests itself in lengthening and tension of the face, increasing the length of the chin and lower section of the face. Usually there is no closure of the lips or closure is difficult and is given with effort. The gap between the teeth obscures the large tongue.
Dental defects
The teeth may have an incorrect position relative to three mutually perpendicular directions. That is, move forward or backward, up or down, and also rotate around its axis.
The following anomalies occur:
- Rotation. This means a change in the orientation and position of the dental unit in the arch. The degree of rotation can be different - in severe cases, reversion of the cervical and lingual surfaces is observed. But most often there is a slight rotation, which can be noticed with crowded teeth. As a result, some teeth may turn to the side.
- Axis change. Normally, all teeth have a certain inclination. For example, the front teeth are slightly tilted outward to provide convexity to the surface of the lips and the correct profile of the face. However, often the units have an abnormal inward slope (oral position) or a strong outward slope (vestibular position).
- Ectopia (ectopic eruption). This term refers to the eruption of one or more teeth outside the line of the dental arch. This usually occurs due to lack of sufficient space. As a result, the teeth form a “double” row. The picture is especially often observed when baby teeth are retained (that is, when they have not completely erupted). As a result, molars begin to grow from the lingual edge of the arch.
- Migration. This type of dental anomaly is characterized by the displacement of an unerupted unit into an incorrect position within the jaw. And, as a rule, migrated teeth do not erupt, but even in this case they cause a number of problems.
- Transposition. As a result of such a defect, two adjacent teeth change places. That is, one of them occupies the normal position of the other on the dental arch. Often transposition indicates the presence of any obstacles to the normal eruption of a tooth. For example, a canine tooth changes with an adjacent premolar.
- Translocation. In this case, the tooth erupts in an unusual place, but remains within the dental arch. This may occur due to the absence of congenital rudiments of some teeth, as a result of which the free spaces are occupied by other units of the row.
- Distal displacement. This type of anomaly is characterized by displacement of one or more units in the distal direction. That is, the teeth “slide” into the back of the arch. This often happens when molars are removed.
- Partial eruption (infraocclusion). In this case, the tooth does not reach the required occlusal plane, that is, it appears incompletely. This is often due to an obstruction (such as insufficient space). Also, the cause of the defect may be underdevelopment of the root structure.
- Pushing out teeth (supraocclusion). The situation is the opposite of infraocclusion. The erupted tooth is located above the line of the entire row. Most often this is caused by the absence of an antagonist tooth, that is, a unit on the opposite jaw. Moreover, both upper and lower units can be pushed out. Often the problem is caused by root caries or periodontal defects.
Various dental anomalies are often combined with each other, resulting in the formation of complex pathologies. Severe crowding of teeth occurs, which makes normal oral hygiene impossible. Additionally, problems arise with tartar, caries and blood supply to the gums.
Possible consequences
Malocclusions often cause psychological discomfort to a person. Many experience embarrassment, problems with communication, and often anomalies lead to facial asymmetry and changes in profile. But, as you understand, the negative consequences of pathologies do not end there.
Bite and dental defects affect health in the following ways:
- The risk of developing periodontitis and periodontal disease increases.
- Plaque and tartar form, which leads to caries and other oral diseases.
- Inflammation of soft tissue occurs.
- Improper distribution of load on teeth leads to increased wear and increases the risk of chips and cracks.
- Speech defects and serious speech therapy problems appear.
- Chronic headaches occur, which are caused by impaired tone of the masticatory muscles.
- Metabolism is disrupted, which leads to gastrointestinal diseases.
This is why experts recommend correcting malocclusions and teeth, and it is best to treat the problem in childhood/adolescence. However, it is worth noting that modern techniques can solve the problem even in adults.
Diagnostic methods
Most bite and dentition defects are noticeable even during a visual examination of the patient. In the future, the orthodontist can only confirm or refute his assumptions. As for hidden anomalies (associated with unerupted teeth), their diagnosis will require the use of X-ray diagnostic methods.
All patients are required to undergo an orthopantomogram - a detailed x-ray of both jaws. An additional computed tomography scan is also performed, which is necessary to draw up a treatment plan. To visualize local disorders, targeted intraoral photographs are taken.
Correction methods
In modern dental practice, several treatment options for dental and jaw abnormalities are used. These include the following:
- Hardware techniques. This therapy involves the use of special correction systems. These are well-known brace systems, as well as various non-removable devices. The treatment period can be up to 3–4 years, but it is possible to achieve complete correction of the bite and displacement of the teeth into the correct position in the row.
- Surgical methods. Some severe and combined pathologies can only be treated surgically. However, this is required extremely rarely, only when treatment with devices is impossible.
- Gymnastics and exercises. Preventive and additional measures that allow you to consolidate the results of treatment, get rid of speech therapy difficulties, etc.
In any case, the necessary treatment option is determined only after consultation with an orthodontist and a full diagnosis.
Remember that proper bite is the key to your overall health, so do not delay treatment. The sooner you take the necessary measures, the faster you will be able to get the desired result.
Still have questions? Consult with the orthodontists of our Clarimed clinic - use the appointment on the website or call us at the numbers provided!
Kinds
In dentistry, such anomalies are usually classified in detail. Orthognathic closure of the teeth allows the chewing pressure to be evenly distributed; in this position, the upper units overlap the lower ones by 1/3 of the coronal part, which is the norm.
Malocclusion is divided into types:
- Distal. It is determined by a strongly advanced high frequency or underdeveloped (pushed back) low frequency.
- Mesial. The LF has a forward position, surpassing the HF in development.
- Deep. A pathology in which the frontal group of the upper units, overlapping the lower ones, injures the gingival tissue.
- Open. Most of the dental units of the HF and LF do not close.
- Cross. An anomaly in which several LF units overlap HF sections and vice versa.
- Dystopia. Teeth are out of place.
Causes
Due to the natural structure of the maxillofacial bones in newborns, the upper jaw is always slightly larger than the lower jaw. With normal development, this nuance is corrected during the growth process and due to the active work of the lower jaw during breastfeeding. If the child is bottle-fed, there is a risk of developing malocclusion.
There are five main causes of malocclusion.
Artificial feeding
This is more likely due to ignorance or oversight on the part of the parents. If the nipple on the bottle has too large a hole, then during feeding the baby’s lower jaw practically does not work and, as a result, does not develop in the desired manner, depriving the baby of the opportunity to naturally correct the malocclusion. To avoid this, it is necessary to select special nipples with a small hole so that the lower jaw actively develops during feeding.
Head position during sleep and feeding
Sometimes the same position of the baby's head during feeding or sleeping can cause the formation of an incorrect bite. Parents need to ensure that this position is changed regularly and allows the jaws to develop normally, preventing the bones from becoming accustomed.
Head position during sleep and feeding
Sometimes the same position of the baby's head during feeding or sleeping can cause the formation of an incorrect bite. Parents need to ensure that this position is changed regularly and allows the jaws to develop normally, preventing the bones from becoming accustomed.
Bad habits
If a child is used to a pacifier or constantly sucks a finger, then over time a space or gap may form between the teeth and jaws. The same problem can arise if the child’s body is incorrectly positioned due to poor posture. If this cannot be corrected, you should consult a doctor who will recommend a set of devices for the prevention of malocclusions, guided by the age of the baby and his individual characteristics.
Consequences of diseases
If your child is often susceptible to rhinitis or suffers from sinusitis, then due to nasal congestion, he usually breathes through his mouth. A permanently open lower jaw also interferes with the normal development of the maxillofacial bones, forms an abnormal bite and contributes to the development of the characteristic “adenoid” type of face.
Heredity
A genetic tendency towards jaw malalignment should also be taken into account (even if only one of the parents has such a defect). Moreover, in each subsequent generation the anomaly intensifies.
Content
- Anomalies of teeth and bite
- Other types of malocclusions
Anomalies of dental bite are different. We are talking about incorrect positioning of the jaws relative to each other and pathological closure, incorrect placement of individual teeth in a row.
Dentists distinguish different degrees of severity of the problem - the first second or third degree of malocclusion. It is important to understand that even a minor defect significantly affects the attractiveness of a smile.
However, the aesthetic component in this case is not the only one. Treatment of malocclusions is mandatory. Since they contribute to the incorrect distribution of the chewing load, which means that some teeth will constantly be subject to greater pressure, contributing to their rapid destruction. Also, these problems are associated with dysfunction of the jaw joints and changes in facial proportions.
PROMOTION
Inexpensive tooth extraction
from 1000 rub.
Prices
| Name of service | price, rub. |
| Preliminary orthodontic analysis: taking an impression from one row of teeth, making a working model, orthopantomogram analysis, photographic examination | from 4000 |
| Correction of malocclusions and tooth position using a simple plate | from 19600 |
| Fixed appliance (braces) for correcting the position of the front teeth | from 40000 |
| Standardized positioners (Myobrace, LM-activator) | from 14000 |
| Vestibular plates (Dr. Hinz Dental) | from 7000 |
| Repeated (control) visits during treatment with removable devices | from 890 |
| Repeated (control) visits during treatment with fixed devices | from 1740 |
| Repairing a removable device | from 2620 |
Deep bite
Expressed in the relative position of the lower and upper jaw rows along the anterior segment so that the upper teeth protrude in front of the lower ones by at least a third of the length of the crowns of the latter. During anterior occlusion, the cutting parts of the lower anterior incisors pass the dental cusps of the upper anterior teeth and touch their palatal parts at the base.
The most advanced forms manifest themselves painfully - the lower central incisors come into contact with the mucous membrane of the palate and, as a result, damage it (this is the degree of deep and traumatic interaction).