A quick review of dental content on the internet reveals a grossly inequitable distribution of useful information about dental implant restoration.
Many people write about implantation, implants, various surgical techniques for restoring gums and bone tissue, but there is very little information about implant prosthetics, making crowns, and stages of prosthetics. We decided to correct this injustice. Therefore, today we will tell you about what happens to implants from the moment of integration and the stages of their prosthetics. Important note! The purpose of this article is to show all aspects of prosthetics as a stage of dental rehabilitation using dental implants. It’s a no brainer that this cannot be done within the framework of one clinical case and one implantation system. Therefore, to create this publication, we took the most important and revealing stages from different clinical cases with different implantation systems. Please be understanding about this.
– NO ONE NEEDS IMPLANTS WITHOUT CROWNS.
The purpose of implantation is to create a durable, most physiological and reliable support for a denture. In order to achieve this goal, two points must be completed:
1. Have an idea about future prosthetics and its plan.
2. Based on the prosthetic plan, place implants of the required size in the desired position (implantological rule #2).
The tasks for the first point are performed by an orthopedic surgeon: he selects the optimal prosthetic scheme for you, taking into account a number of physiological parameters and, of course, your wishes. In good clinics and in the presence of a well-coordinated and competent team of dentists, the orthopedist is not concerned about the very possibility of installing implants, the presence/absence of bone tissue volumes, etc., since all this can be recreated using various methods of bone and gum augmentation. Which is already the task of the implantologist.
In general terms and depending on the clinical situation, you may be offered the following prosthetic schemes:
Based on the prosthetic plan, an implantation scheme is formed, the sizes of the implants and the places for their installation are determined. This requires good and clear communication between the prosthodontist and the implantologist, plus adherence to positioning rules (see Recommendations for implantation, part V). In our clinic, orthopedists also help you choose an implant system that is suitable for your clinical case, since a correctly selected macro-design of an implant can significantly facilitate and reduce the cost of prosthetics. It is for this reason that we have set a fixed price for the installation of any implants.
The easiest (but not the cheapest) way to avoid mistakes when positioning is to use surgical templates:
They are also made by an orthopedic doctor and, in fact, repeat the future prosthetic design.
Surgical templates are either bone or supragingival. The first, more accurate ones, are often used to “bypass” some anatomical obstacles - maxillary sinuses, nerve trunks, etc. The second simply orient the implant along the axis with a known error, which allows osteoplasty, tooth extraction, etc. simultaneously with implantation.
Thus, dear friends, when planning and carrying out implantation
An orthopedic doctor is the most important and most necessary doctor.
Implantological treatment, dental rehabilitation using dental implants, begins with a consultation with an orthopedist . And not an implantologist, as many people think.
The easiest way to imagine this stage of preparation for implantation is to compare it with building a house.
Imagine that you have a plot of land and lots and lots of extra money. You want to build a house. Where do you start?
Probably, for starters, you will invite a surveyor and some geological topographical engineer. They will mark your site, determine the nature of the soil, the groundwater level and give you a conclusion whether it is possible to build something on it at all. And, if possible, what size? In fact, this is the diagnosis and examination that we conduct at the very beginning of any treatment.
Then, you will invite an architect who, using the data received from surveyors and geologists, will design your future home. When planning the number of storeys, the number of bedrooms and bathrooms, he will be based, among other things, on your wishes, lifestyle, etc. And, if you are dealing with a good architect, he will never provide you with an uncontested project - you will always have a choice and the ability to make adjustments. This is exactly how prosthetics are planned.
At the next stage, the project of the future house is transferred to an engineer, whose task is to calculate and construct the foundation. It can be completely different, but it must be reliable and technologically related to the design of your home. If you are planning to build a wooden country house, a simple pile or strip foundation will be enough, but if you plan to build a skyscraper, then the support of your modest Trump Tower should be appropriate. In our case, this is the implantation planning stage.
We do not know a single person who, having first poured the foundation, would call an architect and demand that he build the house of his dreams on this foundation. We do not know of a single construction organization that would start building a house without a design and the necessary geodetic and geological surveys. But, alas, in implantology and prosthetics this approach is very common, and a violation of the sequence of decision-making is one of the main causes of errors, complications and subsequent disappointment for patients.
When all the plans have been drawn up, the decisions have been agreed upon, and you have no questions left - you can begin installing the implants.
Advantages of orthopedic structures on implants
Prostheses that are installed on artificial roots are characterized by several advantages:
- lightweight, compact in size;
- provide a highly aesthetic smile;
- restore the proper functioning of the maxillo-oral apparatus;
- are securely attached and do not fall out of the mouth;
- do not require the use of fixing creams and daily removal;
- relieve complete edentia;
- evenly distribute the chewing load, thereby preventing atrophic processes in bone tissue;
- have a reduced palatal overlap, due to which they promote rapid addiction, do not provoke a gag reflex, and do not distort the taste of food;
- last twice as long as conventional structures (7–10 years);
- are inexpensive.
Implantation stage
Dental implantation is one of the main specializations of our dental center CLINIC IN. Every year we install about a thousand implants in a wide variety of clinical situations, from simple to incredibly complex, including, for example, bone tissue augmentation. Our doctors are mentors at Dentsply Sirona Implants; they teach other doctors how to work with implants and help them solve problems that arise in practice.
It's no surprise that we write a lot about implantation, implants and implant systems. There are even more of them on the website www.implant-in.com, which is mainly intended for doctors. In other words, you always have something to read, so we will skip this step.
Perhaps the only participation of the orthopedist at this stage is the so-called. “immediate prosthetics” – situations when the patient simply cannot be left without a tooth, even for a day. This regularly occurs with the so-called. “immediate implantation” in an aesthetically significant area - we remove the tooth, install an implant and immediately fix a temporary crown to it.
If you don’t delve too deeply into the nuances, then to implement such a treatment plan you need to fulfill a number of conditions:
– implant of the correct size and in the correct position
– sufficient, at least 15 Ncm, primary stability. If several implants are combined into a temporary prosthetic structure, the moment of force can be reduced to 10 Ncm.
– availability of necessary components for temporary prosthetics:
– sufficient and easily predictable volumes of soft tissue surrounding the implant.
– free time with an orthopedic doctor.
The decision to provide temporary prosthetics for a newly installed implant is made only after the implant has been installed.
In general, immediate implantation and, especially, prosthetics are an equation with a large number of variables that are not so easy to solve. Therefore, we will return to this topic later. For now, you just need to know that such a technique exists, and we actively use it:
Examples of work “Before” and “After”
Basal implantology with immediate loading
Case: The patient complained of an uncomfortable removable denture.
Simultaneous implantation in the lateral sections of the upper and lower jaw
Case: tooth decay under crowns in the lateral sections of the upper and lower jaws.
Restoration of all teeth in 4 days - basal implantation
Case: Absence of all healthy teeth on both jaws.
Single-stage removal and basal implantation (September 2012)
Case: destruction of the chewing group of teeth in the lower jaw.
Methods of prosthetics supported by dental implants.
Unfortunately, temporary prosthetics of newly installed implants is not always possible.
Much more often, we choose a longer and more conservative treatment plan that does not involve rapid restoration of missing teeth. Therefore, after implantation, you need to wait 3-4 months (the period required for the integration of implants), the gums will form, and you can go to an orthopedist.
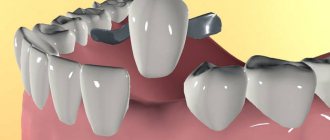
Before we look at what happens next, we suggest getting acquainted with the types of prosthetic structures that rely on an implant.
There are several types and options for permanent implant-supported prosthetics. In some cases, it is preceded by the so-called. “temporary prosthetics.
Temporary prosthetics
This is a very important step and is necessary for approximately 95 patients out of 100. And here’s why:
– unfortunately, we cannot imagine how the implant behaves under load. In a state of “rest” we don’t see any problems, the pictures are excellent, but as soon as he starts “working”, due to the load around him, tissue restructuring begins, hemodynamics change, etc. Structural changes in the tissues surrounding the implant can be either positive (when everything is fine) or negative (when the chewing load causes rapid loss of bone and a change in the shape of the gum). It also happens that the implant simply becomes loose under load and falls out - as a rule, this is a lack of osseointegration due to medical errors. Temporary crowns are a great way to test how an implant works.
– over time, we develop the habit of not using the side of the jaw where teeth are missing. Compensation occurs, among other things, at the level of reflexes, which are not so easy to defeat. Therefore, newly installed crowns on implants can be extremely uncomfortable, and their use can be quite unusual. Unlike ceramic crowns, temporary composite crowns can be easily and quickly adjusted, selecting the most comfortable shape of the chewing surface. In addition, they wear down slowly and similarly to natural teeth. Therefore, their achievement of “full function” is faster, and getting used to them is much easier.
– due to the characteristics of the dental system and the lack of habit of chewing normally, crowns on implants can break or fly off the abutments. Sometimes, under the influence of load, they unscrew and begin to dangle. So, repairing and adjusting temporary composite crowns is much easier, faster and cheaper than permanent ceramic ones.
– with rare exceptions, the gum contour after using formers does not correspond to the natural one. From the point of view of geometry, it is simply a plane with round recesses that open orthopedic platforms; interdental papillae are absent, in principle. In addition, the contour of the gum can change, and it is much easier to correct the shape of the changed gum with a composite temporary crown, but not with a permanent ceramic crown.
– sometimes the treatment is extended, includes orthodontic stages, preparation of natural teeth, changing the height of the bite, etc. If you make ceramic crowns every time and at every stage, you get a variety of shapes and colors, not to mention the need for constant “adjustment” of the chewing teeth surfaces, contacts, etc. In such cases, we first completely restore the bite, function and shape of the dentition on temporary crowns, and only after everything has “worked” as it should, we change the temporary crowns to permanent ceramic ones.
Previously, temporary crowns were made in much the same way as fillings - manually, by layering a composite material on an abutment or plaster stump of a tooth, similar to how teeth are filled or restored. Everything would be fine, but the strength, durability and appearance of such crowns left much to be desired.
Modern temporary crowns are made according to the same principles as permanent ones - they are milled from a solid composite block (or blank) on a special digitally controlled machine. A three-dimensional virtual model of the tooth is used as a “drawing”. Then they are finalized, an abutment is inserted (if there was none beforehand) - and they are transferred to the clinic for installation on the patient. We will talk more about the laboratory stages of making dentures in the next article.
Permanent prosthetics.
It can be removable or non-removable.
Removable structures include various options for total (for a completely toothless jaw) dentures, which can rest either on implants, using special locks, or on a beam fixed to the implants.
The first option uses special locks, very similar to clothing buttons, or special telescopic abutments.
In fact, this method of prosthetics is not the most reliable and convenient, however, its advantage is its ease of implementation and low cost. Therefore, we sometimes use it as a temporary measure to stabilize existing dentures.
The main method of permanent removable prosthetics using implants is the use of a special locking beam (or beams) firmly fixed to the implants to support the prosthesis.
The advantages of this technique are that it is very convenient, very durable and very reliable. In addition, the base height can compensate for any loss of alveolar ridge height - something that is sometimes impossible to achieve using popular methods such as “all-on-four” or “all-on-six”.
The denture can be removed, it is easy to clean, and oral hygiene is very easy to maintain - this explains the popularity of this technique among older patients.
But there are also disadvantages. This is, after all, a removable prosthesis. Not everyone likes it, even purely psychologically. And some types of beam locks require a key, and, as you know, it is periodically lost.
This is where the options for removable prosthetics using dental implants end. And we move on to the most common non-removable prosthetic structures.
Fundamentally, the crown (or crowns) can be fixed to the implant in two ways.
Cement
The first, popular ten years ago and almost never used in modern dentistry, involves the use of a special abutment adapter.
The abutment is fixed to the implant using a screw, and the crown is glued to it using cement.
This is the so-called. “cement fixation”.
The variety of abutments for cement fixation in some systems is simply off the charts. There are standard (straight and angled), cast-in (custom), solid and composite zirconium oxide abutments for cement fixation.
Depending on the task at hand, the doctor and/or dental technician selects the type of abutment that is best suited to solve a specific clinical problem.
Cement fixation, within certain limits, allows you to compensate for the incorrect position of the implant. For example, if its axis and, accordingly, the shaft extend to the front surface of the “visible” teeth:
Important note. In ancient books on implantology, the priority of cement fixation over screw fixation was noted.
The authors saw the reason for preferring cement fixation in the fact that the screws and the precision of manufacturing the components did not make it possible to completely eliminate micromobility of the crown relative to the abutment. But times have changed. And now, fixation of a crown with a screw is the technique of paramount importance in terms of frequency of use and importance, while cement fixation is a compromise. Despite all the aesthetics (the absence of a shaft in the crown), cement fixation has many disadvantages that negate all its advantages:
– impossibility of disassembling and servicing the restored tooth . If a problem suddenly arises, the cement-fixed crown can only be removed by completely destroying it.
– basically, cement fixation is carried out on individual abutments , which need to be made separately and which cost about the same as the crown itself.
– there is always a danger of pushing excess cement under the gum. This can cause inflammation, bone loss and implant loss.
For these reasons, we at CLINIC IN extremely rarely use cement fixation, preferring screw fixation. Fortunately, our implantologists have clear heads and good hands - therefore, we do not have such problems as crookedly installed implants in our clinic.
99% of modern implant crowns are secured with screws.
Screw
For screw fixation of crowns, special adapter abutments are also used. They come in three types.
The first is the so-called. multi-purpose abutments (MP, Multi-Purpose, Multi-Unit, etc.), in the jargon of orthopedists - “cartoons”. Their main task is to transfer the orthopedic interface to a supragingival position, and their purpose is to fix prosthetic structures supported by several implants.
In some implant systems, multi-purpose abutments allow you to quite significantly change the angle of inclination of the prosthetic platform.
This property is used in such prosthetic schemes as “all-on-four”. In our opinion, the “all-on-four” technique is a compromise; there are a huge number of nuances and a lot of contraindications in its implementation. We will bring this up for discussion in future articles.
The second type of abutment is nothing more than a blank for a crown. It is, in fact, “glued” into a cylinder made of zirconium dioxide, ceramics or other material already in the factory; it is impossible to separate it from the frame of the future crown.
To make a crown, this blank is processed on a special milling machine - and the frame of the future crown is created using a digital model.
The third type of abutment is a simple titanium base, the reverse part of the prosthetic interface, to which you can glue anything - individual crowns or a large six-unit ceramic prosthesis.
Due to their convenience, relatively low cost and versatility, we use them quite often.
In other words, dear friends, prosthetics supported by implants differs significantly from prosthetics supported by natural teeth. First of all, the need to use special components selected individually for each case.
Types of fastening structures
There are two ways to fix a removable denture on an implant:
- Beam connection.
Pins (at least four) are screwed into the jaw bone and a metal beam is placed on them. Thanks to it, it is possible to unite and stabilize artificial roots, avoid loosening and falling out of the structure, which ensures long-term operation. In addition, this method allows you to evenly distribute the load and restore the jaw.
On the inside of the beam, metal locks are installed that secure the removable device. If necessary, it can be easily removed.
- Ball-shaped fixation
Holes are made at the base of the structure, with the help of which it is secured to an abutment with a round head. This option, despite its lower reliability, is in high demand among patients due to its low price. A removable denture of this type gradually loosens and becomes mobile, and therefore requires frequent replacement. In addition, it unevenly distributes the chewing load, which can cause discomfort and restrictions in food choice (due to the inability to chew hard foods).
Stages of prosthetics.
At some point, usually 3-4 months after the implant surgery, we check the integration of the implants, take control photographs and create the primary gingival contour using special components called abutments.
And, if everything is in order, after a week or two, the patient is sent to an orthopedic doctor to have dentures made.
At this stage, the main task for the doctor is to transfer the exact position of the patient’s implant to the model. This is done using the so-called. “transfers”. The transfer is fixed to the implant instead of the gum former. Then, an impression is made using silicone mass, and the transfer remains inside it.
The usual impressions are sometimes replaced with 3D scanning of the oral cavity, and instead of transfers, special scan heads are used.
This does not change the essence - the exact position of the implant is transmitted to the dental technician through an impression or a three-dimensional virtual model. All other stages of making your new teeth take place not in the clinic, but in a dental laboratory.
We will talk about them in the next article. The most interesting things are ahead, and this is a reason to subscribe to our website and pages on social networks.
Best regards, CLINIC IN.