Children's dental prosthetics is an opportunity to quickly restore a damaged, lost or missing primary or permanent bite unit. The dental procedure takes 20-40 minutes and is suitable for children of almost any age.
Any tooth loss before the child reaches 6 years of age is considered abnormal and requires urgent solution to the problem.
The lack of timely prosthetics leads to problems with chewing and speech, and provokes the development of bite pathologies.
Why does a child need dentures?
Many parents think that there is nothing wrong with a child missing several teeth until the permanent ones appear. However, ignoring the problem leads to dysfunctions of the child’s body:
- difficulties in sound pronunciation. The teeth are involved in the formation of sounds, the child will adapt and after the radical elements grow, he will begin to pronounce words incorrectly - a speech defect is obvious;
- gastrointestinal diseases - poorly chewed food, injures the mucous membrane of the organs of the system, leads to the development of local diseases, poor absorption of useful components;
- malocclusion - when a child loses a tooth early, other chewing units take its place, the molar has nowhere to grow - it grows out of the row. The result is that a malocclusion is formed, an aesthetic defect and psychological discomfort appear.
A dental prosthesis for a child is designed to temporarily replace the missing element and help avoid unpleasant consequences.
Crowns
Like all children's orthopedic structures, they can be of two types:
- Permanent.
- Temporary.
The latter can be fixative or preventive. They are used when a corner or cutting edge of a tooth is broken off as a result of trauma, to fix the therapeutic material. They are also used to fix devices for various dental defects to prevent tooth displacement.
Important! When performing prosthetics with temporary crowns, tooth preparation is not performed.
Crowns are used in the following cases:
- Bruxism (teeth grinding at night).
- Restoration of permanent teeth after enamel damage.
- Restoration of carious teeth.
- Tooth restoration after pulp removal.
- Complete destruction of the tooth by caries.
- Dental injuries, etc.
When is prosthetics indicated?
Dental prosthetics in children is carried out under the following circumstances:
- the tooth is affected by caries and cannot be restored;
- the element has broken off at the level of the base, root;
- tissues affected by fluorosis;
- bone inflammation has been diagnosed, in which tooth extraction is inevitable;
- periodontitis has been identified as the cause of unit mobility;
- the child has bruxism;
- the patient has underdeveloped enamel or other local congenital pathologies.
Cases in which pediatric prosthetics are necessary
So, pediatric orthopedics is used in the following cases:
- Teeth destroyed by caries cannot be restored.
- Premature loss of baby teeth occurs. If this happened more than a year before the appearance of permanent teeth, then prosthetics are mandatory.
- If it is necessary to remove a tooth when an inflammatory process has begun in the periosteum (periostitis).
- If teeth are destroyed by fluorosis and cannot be restored.
- If after treatment of caries the tooth has an unaesthetic appearance. This is especially true for those teeth that are part of the smile zone.
Modern children's dental prosthetics has the following goals:
- Promoting proper development of the dentition.
- Normalization of breathing.
- Stabilization of proper growth and development of the jaw bones.
- Preventing jaw deformation.
- Restoring the functions of the digestive tract.
- Normalization of chewing and speech functions.
Types of children's dentures
Depending on the transferred functions (purpose), a children's denture for baby teeth can be removable or non-removable.
Removable prosthetics
The defining characteristic of the products is the ability to remove the structure without the help of a doctor, if circumstances so require. They are made from a homogeneous material or several are combined. In the practice of pediatric dentistry the following is used:
- bridge prosthesis. Needed to replace defects of considerable extent (3 or more). Typically, the product is made from different types of plastics. It is possible to use metal to create fixing elements or individual parts of the structure;
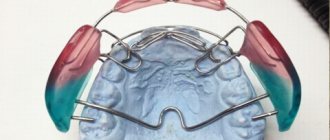
- plate prosthesis. The product consists of a plastic base and fasteners. It can be stationary or sliding. The same type of structures is effective in orthodontic therapy in correcting bite pathologies and aligning individual elements in a row;
- immediate prosthesis or “butterfly”. One-piece thermoplastic nylon base structure. This is a crown, complemented by clasps that “cling” to adjacent units and fix the prosthesis in place. Typically, such a design is installed if a child has lost one “milk jug” due to injury.
Fixed prosthetics
Fixed dental prosthetics for children is important in cases where partial defects need to be restored (the child’s tooth remains in place). We are talking about products such as:
- tab. Fixed orthopedic structures help to “resurrect” the destroyed tooth crown while preserving the pulp and tooth root. In other words, this is a volumetric filling that replaces the destroyed part of the tooth, preserving the anatomical shape of the unit;
- pin tab. Installation of a prosthesis is indicated when the nerve is damaged and its resection is necessary, as well as when the crown is almost completely destroyed and the root is preserved. The doctor fixes the pin carefully, without damaging the thin root walls. The pins are made of chromium-nickel or gold alloys, the crown is “finished” with porcelain or plastic facets;
- crown. A metal structure that replaces the crown part of a decayed tooth. In this case, chromium-nickel alloy or medical steel is used;
- Strip crown is a transparent product. It is used for injuries, carious lesions, and bruxism. The “cap” is made of transparent acrylic; the filling composition plays a secondary role.
Dental prosthetics with crowns for children: indications
Children's dental prosthetics in Moscow are performed according to indications. Each situation is considered by the doctor individually, taking into account the patient’s age, health characteristics and other criteria.
Indications for prosthetics are:
- Destruction of the coronal part by half or even more - due to injuries, caries, pulpitis.
- Non-carious lesions, problems with tooth enamel in children - hypoplasia, aplasia, fluorosis.
- Removal of a baby tooth long before the start of a change in bite or permanent one.
- Gum and periodontal diseases - loosening and loss of teeth due to periodontitis, periodontitis.
- Injuries to the teeth and maxillofacial region - severe damage, chipped enamel, complete dislocation.
- Bruxism is involuntary grinding of teeth, causing deformation, destruction, and tooth loss.
- Anomalies and malformations - absence of primordia of mammary and permanent units, cleft lip and palate and other genetic abnormalities.
- Adentia - complete or partial, caused by hereditary or objective factors.
Prosthetic dental crowns for a child will help solve the problem of missing one or more units.
What should prostheses be like for children?
Children's dental prostheses must meet increased requirements, namely:
- do not interfere with the formation of children's speech and diction;
- be aesthetically pleasing and extremely easy to use;
- do not cause allergies, do not have a toxic effect on the child’s body;
- do not injure the oral mucosa;
- have minimal shrinkage and swelling;
- be resistant to plaque formation.
It is not always possible to eliminate all the negative effects of prostheses on the child’s body. In such cases, they make a choice in favor of those products that cause minimal damage.
Partial congenital or acquired adentia is a fairly common pathology of the dental system, both in adults and in children and adolescents.
The number of young people with lost permanent teeth is significant. According to some data, the frequency of dental defects due to premature removal of permanent teeth in people aged 13-15 years is 12.7%, and at the age of 15-19 years it reaches 25%.
The incidence of congenital adentia, excluding third molars, varies from 1.5% to 28.5%.
Against this background, the problem of the effectiveness of dental implantation is relevant.
Consequences of dental defects
It is known that the presence of even a single defect in the dentition is an etiological factor in deformations of the dentofacial complex and morphofunctional changes in the dentofacial system. First, these changes occur near the defect, and then spread to the entire dentition.
Among the pathological changes caused by adentia are the vertical movement and inclination of the teeth limiting the defect and antagonist teeth, their overload, corpus movement and occlusion disorders, the appearance of diastemas and three, which are most noticeable on the upper jaw.
Removal of the first permanent molars inevitably leads to shortening of the dentition, and in 39% of cases the midline shifts and vertical deformations are observed.
According to V.V. Gordova and a number of other researchers, early tooth loss negatively affects the tone of the masticatory muscles (decreased electrical potential, impaired contractility), complicating their further physiological development, contributing to changes in the articular disc of the TMJ.
In the absence of a tooth, the growth of the alveolar process slows down due to the cessation of mechanical stimulation and the weakening of the activity of reflex arcs coming from the periodontium of the teeth. The absence of a molar in the lower jaw negatively affects the stress-strain state of the jaw bone tissue and promotes resorptive processes in the area of the extracted tooth.
Premature loss of even one permanent tooth leads to disruption of the formation of a permanent bite, the correct growth of the jaw bones and facial skeleton, the formation of interocclusal relationships and bite height, the size and shape of the dental arches. In addition, there is a tendency towards distal displacement of the lower jaw, the occurrence of TMJ dysfunction and a decrease in chewing efficiency.
Often these disorders become irreversible, which is typical for people of any age, but most of all this applies to young patients. This is due, first of all, to the growth and development of organs and tissues, including the jaw bones.
If there is a defect in the dentition in childhood, the question of its restoration always arises. The problem of rehabilitation of children and adolescents with missing permanent teeth is widely discussed in the scientific literature, but studies indicate that prosthetic treatment in childhood is episodic.
Methods of dental prosthetics in children and adolescents
It is well known that dentures must maintain articulatory balance, not interfere with growth and stimulate the development of edentulous areas of the jaw. However, there is no consensus among researchers about treatment methods for children and adolescents with missing permanent teeth.
Bridges are practically unsuitable for replacing missing teeth in early ages, as they can retard the growth of the jaws. The use of sliding prostheses is labor-intensive; they are cantilever, non-physiological and ineffective.
Therefore, most often, dental defects are replaced with removable dentures, which are accessible and easy to manufacture. However, these structures are also unphysiological, and children are sensitive to the need to use removable structures and are often irresponsible in their approach to hygienic measures for the care of dentures, which negatively affects the ecosystem of the oral cavity.
Due to the widespread use of prosthetic techniques based on intraosseous dental implants in adults, scientific publications actively discuss the issues of such prosthetics in children and adolescents with dentition defects.
Research in this area began in the 80s of the last century.
The main problem that has worried and continues to worry researchers is the potential dependence of implants on conditions that change in the maxillofacial area during the process of growth and restructuring of the child’s body.
Features of dental implantation in childhood: a review of studies
Significant progress has been made and the effectiveness of the dental implantation method has been proven for the dental rehabilitation of children with ectodermal dysplasia.
Studies of the dependence of jaw growth on the presence of implants in children with hypohidrotic ectodermal dysplasia and congenital adentia have not found any disturbances in the growth of the jaw bones either in the sagittal or transversal directions.
Thus, in the works of Filius, Sharma, Kearns and other authors, 40 implants were installed in children aged 6-11 years with ectodermal dysplasia. Over the course of 6 years, in all clinical observations, dental implants installed in the frontal region of the lower and upper jaws did not limit their growth in the sagittal and transversal directions, and no violation of osseointegration was observed.
During clinical observations, one implant in the lower jaw and 4 in the upper jaw were partially immersed in the bone, which required orthopedic correction.
Research by O.B. Nenadova, who performed prosthetics on such children aged 3 to 18 years, confirmed their results. The survival rate of dental implants was 97.2%, and control examinations after 3, 6, 12, 18 months did not reveal any significant disturbances in the development of the jaws.
Some patients underwent correction of orthopedic structures.
As for children with normal jaw development and missing teeth, in 1989 the German Association of Implantologists recommended that they should not undergo implantation until they reach 13-15 years of age due to possible bone development disorders.
An exception, according to German experts, may be children with congenital diseases accompanied by multiple edentia.
Sharma and Vargervik do not recommend using this method of orthopedic rehabilitation before puberty due to disruption of the processes of growth and formation of the jaw complex, however, they note that not all patients experience such disturbances.
The authors emphasize that the use of dental implantation must be planned in close connection with the age, number and location of lost teeth, as well as the gender of the patients.
Researchers believe that the use of implants to replace dental defects in growing children allows them to maintain bone volume and has virtually no effect on jaw growth.
The alveolar process of the upper jaw and the alveolar part of the lower jaw grow synchronously with the development and eruption of teeth. The number and degree of formation of teeth determine the age-related sizes of the corresponding sections of the jaws.
The formation of the roots of permanent teeth ends in the following periods:
- incisors - at 10-11 years old;
- fangs - 14-15 years;
- premolars - 12 years;
- first molar - at 10 years;
- second molar - at 15 years.
The final closure of the periodontal fissure ends one year after the end of root formation. This shows that in most children under 12-14 years of age, the formation of the alveolar process of the upper and alveolar parts of the lower jaw ends.
Fundamental studies of the development of the craniofacial complex by Bjork and modern authors prove that after the eruption of all permanent teeth (with the exception of the third molars), the jaw bones stop growing in the sagittal and transversal directions.
From this moment on, only a slight growth of the alveolar process continues in the vertical direction, and therefore the use of dental implants in childhood and adolescence is recommended.
Brahmin, Rakhan and other authors believe that the use of implants during the growth period allows maintaining bone volume and has virtually no effect on the growth of the jaw bones, and those minor changes in the vertical direction are compensated by replacing the orthopedic structure.
Thilander's studies showed that during a 10-year follow-up of adolescent patients with single dental implants, infraocclusion was observed in 7 out of 17 patients, most often in the area of the lateral incisors.
Infraocclusion ranged from 0.13 to 0.98 mm, in the premolar area from 0.1 to 0.6 mm, in the canine area no infraocclusion was found in any of the described cases.
The results showed that dental implantation is indicated in adolescence to replace defects in the dentition and does not significantly affect the development of the dentofacial complex.
Ledermann believes that the bone segment with the implant does not lag behind in growth from the neighboring sections of the jaw bones.
Based on the results of prosthetics for children aged 9 to 14 years with the absence of permanent teeth using intraosseous implants A.V. Kuznetsov concluded that there were no disturbances in the development of the maxillofacial region of the patients.
Some researchers are inclined to think that the younger the child’s age, the greater the likelihood that the implant will influence the growth of the jaw bones.
However, there is no consensus in the literature about the age restrictions for implantation and its possible consequences on the development of the jaw bones.
D.S. Dmitrienko studied 1,744 children aged 9 to 17 years with single dental implants and found no significant differences in the size of the dental arches in the sagittal and transversal directions. However, in the vertical direction some changes were noted in the gnathic part.
In this regard, the author concludes that single dentition defects are indications for dental implantation in childhood and adolescence.
Dmitrienko recommends that the orthopedic part of rehabilitation during the period of incomplete growth of the craniofacial complex be carried out in two stages: first, make temporary structures, and upon completion of physiological gum retraction, replace them with permanent metal-ceramic structures.
The author notes the positive effect of intraosseous dental implants on slowing down the atrophy of bone tissue of the alveolar process.
Heuberer, Dvorak et al followed 18 edentulous children (mean age 12.5 ± 2.6 years) who had 71 dental implants for 11 years. During this time, no significant bone tissue damage was detected in the implantation areas.
The survival rate of dental implants was 89%; correction of the orthopedic structure was carried out in half of the examined patients, on average after 7.8 ± 4.5 years.
An interesting study is by Liu and Behrents, who published the results of experiments in beagle dogs on the relationship between implants and bone during growth.
3 months after implantation, an assessment of radiographs showed that all implants were well integrated with the bone, the implantation was local, and did not inhibit the growth and development of the jaw bone.
Another study on dental implants in children, conducted at the University of Colorado Health Sciences Center, found that after dental implants, jaw formation is disrupted in all directions during bone growth (ages 6-8).
These conflicting data showed that the implant is able to remain in the bone at the point of its formation and retards jawbone growth because it can neither move nor adapt to bone remodeling.
Increasing discrepancy between the implant and bone can lead to implant failure, so the authors do not recommend implantation during the active growth period. It should be started no earlier than puberty (12-14 years), since implantation during this period has more predictable results.
The authors recommend that implantation be carried out under strict clinical supervision.
If any signs of impaired jaw growth are detected, immediate removal of the implants should be insisted on.
Bergendal published a statistical analysis of implant use in children under 16 years of age in Sweden. The purpose of the study was to compare the effectiveness of the use of dental implants in children with congenital non-syndromic edentia, secondary edentia due to trauma and hypohidrotic ectodermal dysplasia.
Research results show that among 5 children with ectodermal dysplasia, who had 14 implants installed, 9 were lost due to unfavorable anatomical conditions, and not due to impaired osseointegration due to somatic pathology.
In the group of children 14-15 years old without somatic pathology (21 patients), only two had problems with osseointegration of dental implants. The authors note that implant treatment in growing children should be done with caution.
No less interesting is the study by Zachrisson, which examined the long-term results of aesthetic rehabilitation of patients with implants. The author studied infraocclusion of implants in the frontal region of both jaws in individuals of all ages.
When studying vertical changes in implant prosthetics in a group of young patients (from 15 to 21 years old) in the long-term period (about 4.2 years), there was a decrease in the occlusion of crowns on implants by an average of 0.7 mm (from 0.1 to 1.4 mm).
Similar results were obtained in studies in a group of mature patients (40-55 years old) - a decrease of 0.9 mm on average (from 0.1 to 1.8 mm).
These data indicate that changes in crown height and individual differences among patients were independent of age.
Dental implantation in the context of the development of the dentofacial system
When choosing a method for replacing teeth, the dentist must have a clear knowledge and understanding of the growth and development of the maxillofacial region in children and adolescents.
When planning and conducting dental rehabilitation, especially orthodontic and orthopedic, the doctor intervenes in the development processes of not only the dentition, but also the maxillofacial complex, and manipulation of this process should only be for the benefit of the patient.
This is especially true in childhood and adolescence, when it is important to be able to distinguish developmental anomalies within the physiological norm from a pathological process.
The choice of method of orthopedic treatment of dentition defects in childhood and adolescence is based on the principles of development of teeth and jaws, as well as on the mechanisms of craniofacial growth. The growth and development of the upper and lower jaws are very different.
This also applies to specific areas of each jaw.
The development of the maxilla in early life is closely related to the base of the skull, implying "growth from under the skull." Two processes are observed here: a significant displacement of the anterior and lower parts relative to the base of the skull and reconstruction of its anterior surface. Later, the size of the upper jaw only increases.
There are vertical, transverse and anteroposterior growth of the jaw.
Transverse growth occurs mainly in the area of the middle palatal suture.
The vertical growth of the upper jaw is due to its passive displacement. It is development in the vertical direction that influences the stability and effectiveness of dental implants at an early age.
The growth of the mandible mainly occurs downward and forward due to both intracranial growths during growth and apposition and resorption of bone on its surfaces.
The growth of the jaw is not only linear, it is combined with rotation and depends on the orientation of the sprout. As a site of growth, the anterior region of the jaw is practically inactive.
It is carried downwards and forwards, the main development of the mandible extending along the posterior surface of the ramus by the overlay of new bone.
In parallel with the growth of the lower jaw in length, it also increases in width due to expansion in the lateral regions.
Mandibular growth may also have some influence on the stabilization and displacement of dental implants, especially in the posterior regions due to vertical growth and resorption processes.
In adolescence, accelerated skeletal growth is observed in girls from 10 to 12 years old and boys from 12 to 14 years old. Peak growth begins approximately 2 years after puberty. The cumulative growth curve of the facial skeleton is parallel to the somatic growth curve.
Behrents' research has shown that facial growth continues beyond adolescence. However, it is correct to believe that growth processes slow down significantly after puberty. It is also important to assess growth rates in three dimensions.
Width growth is one of the first to stop, reaching its practical completion at the beginning of ripening. Significant anteroposterior growth of the maxillary skeleton lasts longer and ends at the end of puberty.
Vertical growth, which stops after puberty, is observed at a moderate level throughout adult life.
Therefore, despite studies conducted by domestic and foreign authors, there is no opinion on the use of dental implants in growing patients.
In the last decade, an increasing number of literature sources have suggested the possibility of implantation in adolescence.
However, there are no clear indications for the use of dental implants depending on the age of the child, the location of the defect, and its length.
The authors differ on the types of implants, suggesting that patients under 15 years of age can be either permanent or temporary, with subsequent replacement.
Particularly noteworthy is Sharma's conclusion about the possibility of installing a dental implant at an age when the formation of the root of the replaced tooth has been completed.
Progress of prosthetics
Regardless of the type of prosthetic structure, the procedure includes the following steps:
- examination, consultation;
- diagnostics - conduct a survey, examine the child (take an x-ray);
- preparation for fixation of the prosthesis. If necessary, treat the tooth;
- taking impressions;
- product production;
- fitting and installation of the prosthesis.
Before fixing any type of product, general preparation of the unit is required - organizing professional cleaning of the enamel layer.
Children's orthodontic dentures
Wearing dentures in childhood is necessary to prevent orthodontic problems. A well-chosen design contributes to the correct development of the bite and the formation of tissues of the dental system.
Adentia, premature loss of teeth, creates not only psychological discomfort for the child, but also affects his physical development, creating problems of the following nature:
– adjacent milk teeth fill the space of the fallen unit, leaving no room for the eruption of permanent teeth. This leads to pathological occlusion, traumatic occlusion, damage to both dentitions;
– diseases of the gastrointestinal tract. Poor chewing of food also causes weight loss, decreased immunity, and general physiological retardation;
– respiratory dysfunction;
– change in the shape of the palate.
Mixed dentition teeth are lost prematurely due to tooth decay or trauma. In the latter case, the frontal units, on which dental aesthetics depend, are affected. This is fraught with disruption of bone tissue development and distortion of the growth of permanent dental units.
Why is it safe to install children’s prostheses in Stokos?
The Stokos Clinic in St. Petersburg works tirelessly to ensure that young patients and their parents feel calm and comfortable within our walls. Our doctors are trusted because with us:
- reliable. Stokos Dentistry employs experienced, certified doctors who approach business wisely and never act according to a template;
- calmly. Our dentists know how to make the child comfortable with themselves and the process - parents do not have to worry about their child;
- comfortable. Our staff is always polite to those who contact us, smiling and prompt in taking action;
- inexpensive. We set fair prices for services.
Make an appointment with our doctor right now - because here, with us, sincere smiles are born!
Prescription of prophylactic prostheses
Artificial structures are installed to solve the following orthopedic and surgical problems:
– immobilization of mandibular joint mobility;
– correction and strengthening of the dental arch;
– functional replacement of lost teeth, psychological comfort of the patient;
– compensation of articulatory balance;
– prevention of the development of pathologies of the dental system, atrophy of the alveolar processes;
– stimulation of jaw bone growth;
– therapy of mandibular dislocation or subluxation caused by trauma, malocclusion, rheumatism, arthrosis, arthritis and other pathologies;
– prevention of occlusal disorders during the rehabilitation period after installation of osteoplastic structures, implants, periodontal surgery, treatment of injuries, etc.
How long do you wear a dental plate?
Typically, teeth straightening plates are worn for 6 months to 1 year. It all depends on the individual characteristics of the bite, as well as the regularity and duration of wearing the product.
The period of getting used to the plate lasts about 2 weeks. First, the orthodontist makes the product according to individual measurements and shows the little patient where her clasp feet are located and how to use them. Children should learn to put on and take off the plate themselves from the very beginning. However, the less they wear it and the more often they take it off, the longer the treatment will last. Parents should explain to the child that removing the plate is only allowed for a short time.
Under no circumstances should the plate compress or injure the teeth. The force exerted by it remains minimal throughout its wearing. The child should never experience pain or suffer from constricted circulation inside the mouth. The duration of wearing is primarily due to the fact that the teeth move into the correct positions smoothly and gradually. They will then need some time to “get used to” their new places.
ATTENTION:
During the course of treatment, the child will need to be brought to the clinic for examination once every 1-2 months.
Why do children have malocclusion?
Malocclusion in children is very common and should not cause increased concern among parents. This is not a disease, but a developmental feature, and it can be corrected quite easily. Most often, the bite is crooked for the following reasons:
- the child inherited an atypically small jaw from his parents;
- teeth erupted faster than the jaw grew;
- the baby quickly developed caries, so he had to have his baby teeth removed;
- the child often bites his lip, sucks his finger, or has other bad habits that negatively affect his bite.
Also, problems with bite occur in boys and girls who often catch colds and cannot breathe through their nose. If nasal breathing is difficult due to enlarged adenoids, the small patient has to breathe through the mouth willy-nilly, which can affect the bite.
While the teeth are still baby, you can still come to terms with the curvature of the bite. But as soon as they begin to change to permanent ones, you need to start visiting the orthodontist to prevent possible problems. The sooner you start correcting your bite, the easier and cheaper it will be to get your teeth into the correct position. Most likely, for this, the doctor will put plates on the child’s teeth.
ATTENTION:
For the manufacture of children's orthodontic plates, hypoallergenic materials that are completely safe for health are used.
Correct your bite or dental defect with invisible aligners Find out what it is
Why do we need plates on teeth?
Plates for correcting malocclusion in children are orthodontic devices with plastic bases. They reproduce the shape of the palate and the inner surface of the teeth as accurately as possible. This creates the correct conditions for the positioning of incisors, canines and molars when they change from baby to permanent.
Plates on teeth are designed to perform the following functions:
- expand the dental arch;
- correct the tilt or rotation of teeth;
- provide free space for growing permanent teeth;
- prevent displacement of the dentition;
- correct the size of the sky;
- regulate the growth of bone and jaw tissue;
- model the shape of the upper and lower jaw.
To carry out these tasks, screw mechanisms are built into the plate on the teeth. Their number and location depend on the individual characteristics of the bite. Also, the orthodontist can provide separate elements that will improve the position of individual teeth (that is, straighten their rotations or inclinations). The more such mechanisms and elements in the plate, the higher its cost.
Turning the screw one step frees up ¼ mm of space in the dentition. The child does not experience pain - he feels only slight pressure, which completely disappears after a maximum of 20 minutes.
For the sake of the child’s psychological comfort, the plates are usually made bright and cute, sometimes fairy tale and cartoon characters are drawn on them. Let the child think that this is a toy or decoration, and not a medical item - this way he will be more willing to wear it.
ATTENTION:
Such devices are most often prescribed to children under 12 years of age. However, adults also sometimes wear plates - usually non-removable.