Odontogenic sinusitis is an inflammation of the maxillary sinuses that develops from infected teeth of the upper jaw. The penetration of infection is also facilitated by dental manipulations in the area of the maxillary sinuses - treatment and extraction of teeth, implantation and sinus lifting. Without identifying and eliminating the cause, standard treatment by an ENT doctor in a clinic does not bring results. Treatment of odontogenic infections must be comprehensive!
Doctor Levin Center has been specializing in the treatment of patients with combined ENT and dental pathologies for more than 20 years. Comprehensive rehabilitation programs are carried out by maxillofacial surgeons with otolaryngological training.
Causes of odontogenic sinusitis
The maxillary sinuses (maxillary sinuses) are separated from the oral cavity by a thin layer of bone in which the roots of the upper chewing teeth are located. Such close proximity poses a threat of sinus infection. In 15% of cases, the apices of the roots are anatomically located under the mucous membrane of the sinus, without a bone layer, which further increases the risk of developing odontogenic sinusitis.
Conventionally, the reasons can be divided into 2 categories:
Delayed dental treatment
With pulpitis and periodontitis, infection from the dental canals slowly but surely spreads to the surrounding bone tissue. Without treatment, foci of infection grow, melt the bone septum, opening the “gate” for the penetration of pathogenic microflora. In advanced situations, cysts form on the roots of teeth, and when the bone barrier is destroyed, they grow into the sinus.
Medical errors
As a result of dentist errors, mechanical damage to the sinus floor is possible (perforated form of the disease). The result is the formation of a communication with the sinus, the penetration of foreign bodies with the body’s response in the form of odontogenic sinusitis.
The most common treatment errors after which patients turn to our Center:
- Unsuccessful endodontic treatment The therapist did not calculate the effort during mechanical cleaning and filling of dental canals. There was a fracture and pushing of the instrument and/or removal of the filling material beyond the root apex into the lumen of the sinus.
- Traumatic tooth extraction The surgeon, without preliminary diagnosis, having no idea about the location of the roots, damaged the bone septum. Perforation of the sinus floor occurred, often with the tooth or its fragments falling into the sinus cavity.
- Implantation without sinus lift Experimental implantation protocols without prior bone grafting result in damage to the sinus floor by the implant. If the perforation goes unnoticed during surgery, the implant flies into the sinus.
- Sinus lift without diagnostics The surgeon did not calculate the bone tissue parameters and did not assess the condition of the mucous membrane. During the preparation of the bone septum, its perforation and rupture of the membrane occurred. Bone material ended up in the sinus cavity.
Odontogenic sinusitis: traditional and endoscopic surgical treatment methods
Errors by a dentist during endodontic treatment of maxillary teeth often lead to the removal of filling material into the maxillary sinus [1, 3, 6]. Mechanical effects, as well as the cytotoxic and sensitizing effect inherent in almost all types of modern pastes for obturation of the root canals of teeth, lead to inflammatory and purulent-necrotic changes in the mucous membrane of the maxillary sinus. As a result, an isolated chronic pathological process gradually develops, exerting a pathogenic effect not only on surrounding tissues, but also on the body as a whole [5, 7, 8].
The relevance of research
Current treatment methods for the above category of patients are often associated with surgical trauma to tissues not involved in the pathological process: bone, mucous membrane, soft tissues of the cheek. Some authors propose rather contradictory approaches. Some experts believe that the filling material in the sinus will dissolve over time, others believe that its presence does not have a harmful effect on the sinus mucosa and its functional state. This approach certainly leads to the progression and spread of the inflammatory process from the maxillary sinus to other paranasal sinuses and the orbit.
Some experts believe that the filling material in the sinus will resolve over time, others believe that it does not cause serious harm to the mucous membrane of the sinus and its functional state. A number of authors note that rhinogenic infection often exacerbates the latent odontogenic process, and this combination of sources of infection can lead to to hematogenous dissemination of infection with damage to individual organs and systems of the body [4, 5, 7, 10]. Carrying out only conservative treatment for odontogenic sinusitis caused by the removal of filling material in the maxillary sinus does not ensure complete recovery of the patient; moreover, after physiotherapeutic procedures, most patients experienced increased pain and exacerbation of clinical manifestations [1, 3, 9].
In this regard, complex treatment of patients with this pathology is impossible without surgical removal of the root sealant [1, 3, 11] as soon as possible [2, 3], however, such an intervention is associated with surgical trauma.
A number of studies analyze clinical situations with different localization of filling material in the maxillary sinus - in the cavity, near the lower, medial walls of the sinus, in the lateral corner, in the area of the lower wall of the orbit. The nature of the foreign body, its localization, volume, prevalence, as well as the severity of pathological changes in the mucous membrane of the maxillary sinus, of course, require the selection of an adequate surgical technique and tactics for surgical access to the sinus [1, 4, 9].
Purpose of the study
A comparative study of the effectiveness of various methods for removing filling material from the maxillary sinus, including the use of endoscopic techniques, depending on the location of the root sealant in the sinus.
Material and research methods
A total of 72 patients were observed, including 27 men and 45 women, aged from 26 to 54 years, who had filling material in the maxillary sinus from 1 week to 18 months.
46 people (64%) presented with clinical manifestations of exacerbation of chronic maxillary sinusitis; 26 patients (36%) had no complaints during the initial examination, but a foreign body in the maxillary sinus was determined by x-ray. Clinical examination of patients began with a detailed X-ray examination. If necessary, computed tomography (CT) was performed, which made it possible to accurately determine the location and size of the foreign body located in the sinus.
Depending on the surgical technique used to remove filling material from the sinus, patients were divided into 2 groups. In the first group (52 patients), operations were performed using standard surgical instruments and a straight saw. In the second group (20 patients), endoscopic techniques were used.
The surgical intervention using standard surgical instruments was carried out according to a method described in sufficient detail in the literature [1, 3, 4, 9, 11], and is a modification of the Caldwell-Luke operation, the essence of which is as follows: appropriate conduction anesthesia is performed, then an arcuate incision is made in the mucous membrane and periosteum from the canine to the molars (Fig. 1), after partial peeling of the mucoperiosteal flap using a straight saw, a bone window is formed in the anterior wall of the maxillary sinus, over which the mucosa and periosteum are preserved. A window measuring 1.5x1.5 cm is cut out at an angle of 45?. After opening the sinus, the filling material and polyposis-altered mucosa are removed (Fig. 2).
Rice. 1. Detachment of the mucoperiosteal flap, preserving the periosteum and soft tissues (drawing by the authors). Rice. 2. Filling material in the sinus (drawing by the authors).
Then the bone fragment with the periosteum and soft tissues attached to it is returned to its place and fixed with a 5.0 vicryl suture (Fig. 3, 4).
Rice. 3. The bone window is fixed with sutures (drawing by the authors). Rice. 4. The wound is sutured (drawing by the authors).
Depending on the changes in the sinus mucosa, a “gentle” or “radical” maxillary sinusotomy was performed with mandatory complete (under X-ray control) removal of the filling material. 33 and 19 patients were operated on using the “gentle” and “radical” maxillary sinusotomy methods, respectively. Then, over the course of a week, all patients were prescribed 5-7 sessions of physical therapy using the Optodan laser device. By the end of the week, the stitches were removed.
Research results
When performing an X-ray examination, the accumulations of filling material brought into the maxillary sinus had a different appearance: single, clearly defined round intense shadows, many round shadows, clusters of irregularly shaped bodies of various sizes. The localization of these shadows was different, they were detected near the roots of the “causal” teeth and the bottom of the maxillary sinus in 35% of cases, and in 65% of cases they were located in the projection of the roots of neighboring teeth, in the upper medial corner or center of the sinus, and also near the orbital stack.
The main indication for the use of endoscopic technology was the short period of time the foreign body was in the sinus and the absence of pronounced changes in the sinus mucosa. According to the patients, the removal of filling material into the maxillary sinus was initially not accompanied by any symptoms. Painful sensations characteristic of exacerbation of odontogenic sinusitis appeared within 3 months. up to 1 year. It should be noted that in most patients the first clinical signs of the disease were diagnosed after suffering from acute respiratory viral infection. Patients noted a feeling of heaviness, discomfort in the affected sinus area, impaired sense of smell and nasal breathing, unilateral nasal congestion, pain of varying severity, radiating to the teeth and zygomatic area.
In all these patients, the foreign body and altered areas of the mucous membrane, which were mainly hyperplastic in nature, were removed. The length of the process depended on the length of time the filling material was in the sinus. When revising the sinus, the mucous membrane was preserved completely or individual polyps were excised without exposing the bone walls; sinus tamponade was not performed. In the postoperative period, in addition to traditional antibacterial and anti-inflammatory therapy, vasoconstrictor drugs were prescribed 3 times a day into the nasal passage on the side of the operated sinus, which ensured normal drainage and aeration of the sinus.
In 19 patients, changes in the sinus mucosa were of a diffuse polypous nature, and these patients underwent radical maxillary sinusotomy with the formation of an artificial anastomosis with the nasal cavity. Thus, such pronounced changes in the mucous membrane were observed in patients with a long-term presence of a foreign body in the sinus, even with a small amount of it.
The main indications for the use of endoscopic technology were short periods of presence of a foreign body in the sinus and the absence of pronounced changes in the sinus mucosa. Patients who used this method using endoscopic technology were also divided into two groups, depending on the access.
In the first group of patients, endoscopes were inserted into the sinus through the anterior wall of the sinus (Fig. 5). Eight patients were operated on using this method. In the second group of patients (12 patients), surgical access to the maxillary sinus was carried out through the natural opening in the middle meatus (Fig. 6).
Rice. 5. Maxillary sinusoscopy using endoscopic technology (drawing by the authors). Rice. 6. Endoscopic endonasal maxillary sinusoscopy (drawing by the authors).
This access is more physiological, as it allows to reduce the amount of surgical trauma to a minimum, preserve the “causal” tooth, provide conditions for normalizing the functions of mucociliary clearance into the nasal cavity, and reduce the rehabilitation period of patients by 30% compared to patients of the first group. In the postoperative period, the maxillary sinus was washed daily through the drainage with a Miramistin solution.
During endonasal intervention, correction of intranasal structures and endoscopic monitoring of the condition of the operated area were performed (Fig. 7-8).
Rice. 7. Endoscopic view of the endonasal approach to the maxillary sinus (drawing by the authors). Rice. 8. Correction of intranasal structures and endoscopic monitoring of the condition of the operated area (drawing by the authors).
Complex therapeutic treatment included the use of desensitizing, intranasal vasoconstrictor and non-steroidal anti-inflammatory drugs. The effectiveness of the methods was assessed according to the following criteria: removal of all filling material from the maxillary sinus, absence of complications and relapses of the disease in the postoperative period at regular intervals.
conclusions
As the research results have shown, all the methods used make it possible to completely remove the filling material from the maxillary sinus. However, it is necessary to clearly differentiate the tactics of surgical intervention, based on the results of radiography and CT scans based on the location of the foreign body in the maxillary sinus and the condition of its mucous membrane, with the involvement of otorhinolaryngologists.
In case of total disruption of pneumatization of the maxillary sinus, signs of blockage of the natural anastomosis with the nasal cavity and disruption of nasal breathing functions, after removal of the filling material, the tactics of endonasal maxillary sinus are indicated with the restoration of natural communication and ventilation of the maxillary sinus through the nose.
The list of references is in the editorial office.
How to avoid
There are only two ways to prevent the development of odontogenic sinusitis:
- Treat your teeth in a timely manner, prevent infection of the dental canals and spread of inflammation beyond the apex of the tooth root.
- Contact proven clinics with experienced doctors, the opportunity to conduct a thorough diagnosis and provide for an emergency situation.
In our Center, not a single dental procedure, especially at the border with the maxillary sinuses, is performed without a thorough X-ray examination using a computed tomograph.
The study is carried out using
a high-precision Sirona device with the Galileos diagnostic software package.
Based on the results of computed tomography, we determine the location of the roots and the size of the bone septum. This makes it possible to plan treatment in such a way as to avoid risks.
Tooth extraction operations and other interventions in the area of the maxillary sinuses in our Center are performed only by maxillofacial surgeons with ENT training . Deep knowledge of the anatomy of the maxillary region allows you to avoid mistakes that a regular dentist might make. But each case is individual, and even if something goes wrong, our doctors are always ready for any turn of events and correct the situation.
Systemic antibacterial therapy for odontogenic maxillary sinusitis at the present stage
Tsarapkin G.Yu., Turovsky A.B., Zavgorodniy A.E.
Chronic sinusitis ranks first among all chronic diseases of the ENT organs. Chronic sinus inflammation usually develops against the background of a recurrent acute process. According to the international classification, sinusitis is considered chronic when the inflammatory process lasts more than 3 months. In our opinion, the most rational for clinical practice is the modified classification of chronic sinusitis according to B.S. Preobrazhensky. According to this classification, the following forms of inflammation of the paranasal sinuses are distinguished: exudative, productive, alterative, mixed, vasomotor and allergic.
A significant role in the occurrence of chronic inflammation in the maxillary sinus belongs to diseases of the teeth of the upper jaw. Odontogenic sinusitis (OG), in fact, is a complication that arises as a result of the spread of a pathological process from the periapical focus of chronic infection in the area of premolars or molars of the upper jaw (periodontitis, periostitis, osteomyelitis, suppurating radicular cysts, there are also indications of the possibility of sinusitis occurring with abscessive form of periodontitis). Patients with odontogenic sinusitis are admitted for treatment to both dental and otorhinolaryngological hospitals. According to dentists, odontogenic sinusitis is found in 12-50% of patients with chronic sinusitis. According to the observations of otorhinolaryngologists, the frequency of odontogenic sinusitis ranges on average from 2 to 25%, with its open (perforated) form being 41.2-77.2%. Such contradictory data are not due to the true ratio of odontogenic and rhinogenic sinusitis, but to the specifics of examining patients in hospitals of various profiles. Diagnosis of odontogenic sinusitis is difficult and requires synergy in the work of otorhinolaryngological and dental services. Diseases of the teeth of the upper jaw, which are practically asymptomatic, are, as a rule, not regarded as a cause of sinusitis. Unfortunately, dentists and otorhinolaryngologists often underestimate the cause-and-effect relationship between the pathology of the maxillary sinus and diseases and anomalies in dental development, which leads to diagnostic errors and a recurrent course of the disease. Treatment of odontogenic sinusitis should be comprehensive and in all cases include sanitation of the source of infection.
The difficulty of conservative treatment of odontogenic sinusitis lies in the fact that the inflammatory process in the maxillary sinus, which developed as a result of prolonged periapical inflammation of the teeth of the upper jaw, takes on a primarily chronic nature and in most cases requires surgical treatment, the extent of which depends on both the endoscopic picture and the functional state mucous membrane. Conservative treatment is effective only for the exudative form of inflammation.
Antibacterial therapy for odontogenic maxillary sinusitis is empirical in nature and is based on data on the main pathogens and their sensitivity to antimicrobial drugs in the region. It also takes into account the fact that due to the high prevalence of microbial associations, the risk of occurrence of b-lactomase-producing strains significantly increases. In this regard, antibiotic therapy for odontogenic sinusitis comes down to a choice between protected penicillins and respiratory fluoroquinolones.
The purpose of our study was to study the possibilities of increasing the effectiveness of treatment of odontogenic sinusitis.
Over the past year, we have observed 32 patients suffering from odontogenic sinusitis and undergoing inpatient treatment in the ENT department of the Moscow Clinical Hospital named after. S.P. Botkin - 13 men and 19 women (average age - 38 years).
The diagnosis of odontogenic sinusitis was established on the basis of complaints, medical history, objective examination (sinusoscopy, endoscopic examination of the nasal cavity, oroscopy), and the results of X-ray examination (radiography, panoramic zonography and CT scan of the paranasal sinuses). All patients were consulted by a dentist. All patients had mild to moderate severity of the disease.
The “causal” teeth were: 1st molar – 19 patients, 2nd molar – 9 patients, 2nd premolar – 4 patients. In one case, there was a combination of pathology of the second premolar and first molar.
Among the examined, 4 people had an open (perforated) form of odontogenic sinusitis: 3 - antroalveolar communication with the maxillary sinus due to removal of the first molar, 1 - second molar.
The group with a closed form of odontogenic sinusitis consisted of 28 people, and in four cases the process was associated with the presence of filling material in the maxillary sinus. The exudative form was registered in 9 patients.
According to the results of the examination, surgical treatment was recommended for 19 patients with a closed form of odontogenic sinusitis, 14 of them refused the proposed operation.
As a result of bacteriological studies, associations of anaerobes and aerobes were found in 17 patients with odontogenic sinusitis in the punctate of the maxillary sinus. Isolated cultures of aerobes and anaerobes were obtained in 3 and 7 cases, respectively. No flora growth was obtained in 5 studies (Fig. 3).
Aerobic flora was represented by Streptococcus spp., Staphylococcus aureus, Haemophilus influenzae, Pseudomonas aeruginosa. Anaerobic - gram-positive cocci (Streptococcus spp.), Veillonella spp., Prevotella spp., Peptostreptococcus spp., Fusobacterium spp.
Conservative treatment included antibacterial therapy with protected penicillins, puncture (washing) of the maxillary sinus with the introduction of saline, and local use of decongestants. All patients were consulted by a dentist; sanitation of the odontogenic focus of infection was carried out on the 3-4th day after the start of conservative therapy.
In our work, we compared the effectiveness of systemic antibacterial therapy for odontogenic sinusitis with amoxicillin/sulbactam, which recently appeared on the Russian market, and amoxicillin/clavulanate, which has long been used in ENT practice. Both drugs belong to the group of protected penicillins.
Trifamox IBL® (amoxicillin/sulbactam) is an antimicrobial agent from the penicillin group (registered in the fall of 2005 in Russia (Trifamox IBL®, Laboratorios Bago S.A., Argentina)), has a wide spectrum of bactericidal action against aerobic gram-positive bacteria (including strains producing b-lactamases): Staphylococcus aureus, Staphylococcus epidermidis, Staphylococcus saprophyticus, Streptococcus pyogenes, Streptococcus anthracis, Streptococcus pneumoniae, Streptococcus viridans, Enterococcus faecalis, Corynebacterium spp., Listeria monocytogenes; anaerobic gram-positive bacteria: Clostridium spp., Peptococcus spp., Peptostreptococcus spp.; aerobic gram-negative bacteria (including strains producing b-lactamases): Escherichia coli, Proteus mirabilis, Proteus vulgaris, Klebsiella spp., Salmonella spp., Shigella spp., Bordetella pertussis, Yersinia enterocolitica, Gardnerella vaginalis, Neisseria meningitidis, Neisseria gonorrhoeae, Moraxella catarrhalis, Haemophilus influenzae, Haemophilus ducreyi, Yersinia multocida, Campylobacter jejuni, Acinetobacter spp.; anaerobic gram-negative bacteria (including strains producing b-lactamases): Bacteroides spp., including Bacteroides fragilis.
Amoxicillin acts bactericidal by inhibiting the synthesis of the bacterial wall. Sulbactam is a stable, irreversible inhibitor of b-lactamases secreted by microorganisms resistant to b-lactam antibiotics. Sulbactam expands the spectrum of activity of the drug against resistant strains, without changing the activity of amoxicillin against sensitive strains, forming complexes with penicillin-binding proteins of bacteria, and exhibits synergy when used simultaneously with b-lactam antibiotics. Sulbactam does not have its own clinically significant antibacterial activity (with the exception of Neisseriaceae and Acinetobacter).
The drug is available in both tablet and injection forms, which is very convenient when carrying out step-by-step therapy. When taken orally, the drug has a large volume of distribution and reaches high concentrations in tissues and body fluids, especially in the mucous membrane of the upper respiratory tract. In terms of the rate of development of the bactericidal effect, amoxicillin/sulbactam is significantly ahead of other antibacterial drugs, since it has significantly greater resistance to changes in the pH of the solution than clavulanate or tazobactam, and from a practical point of view, this means that in the conditions of a real infectious process occurring with significant variations in the acidity of the environment, sulbactam is able to penetrate tissue more actively than other b-lactamase inhibitors.
In our work, patients who received only conservative treatment, depending on the antibiotic therapy performed, were divided into 2 groups (main and control), similar in gender, age and the nature of the process in the maxillary sinuses and dentofacial area. The main group included patients receiving amoxicillin/sulbactam; in the control group, antibacterial therapy was carried out with amoxicillin/clavulanate. All patients received an antibiotic in comparable dosages to amoxicillin (500 mg x 3 times a day per os).
Based on the results of conservative treatment, a pronounced positive dynamics of the main clinical symptoms of the disease was noted by the 7th day in both groups of patients with the exudative form of odontogenic sinusitis. In patients with purulent polyposis lesions of the maxillary sinus who received amoxicillin/sulbactam, remission was achieved on the 8th day, and in the control group on the 9th.
Antimicrobial effectiveness and high sensitivity of microorganisms to drugs are confirmed by data from microbiological studies over time.
Thus, amoxicillin/sulbactam is not inferior to traditional protected penicillins, the clinical effectiveness of which is time-tested, and also has a number of advantages:
- Sulbactam is more resistant to pH changes, due to which it is able to more actively penetrate into inflamed tissues.
- Sulbactam's high tolerance to pH fluctuations allows it to be administered intramuscularly.
- Sulbactam is more resistant to most plasmid and chromosomal type I b-lactamases.
- Amoxicillin/sulbactam is more convenient for sequential therapy, since, in addition to oral administration, it has a form for intramuscular and intravenous administration.
In conclusion, it should be noted that amoxicillin/sulbactam is an effective drug in the treatment of odontogenic sinusitis and can be recommended as initial therapy for chronic maxillary sinusitis. The optimal choice of antibacterial agents for the treatment of odontogenic processes in the maxillary sinus reduces the treatment time.
Symptoms of odontogenic sinusitis
Inflammation from infected teeth develops gradually and in the initial stages is most often asymptomatic. If dental treatment has been carried out, symptoms may also not appear immediately - it all depends on the body’s immune system and reaction to foreign bodies. There are cases that sinusitis does not make itself felt for several years.
But sooner or later the infection will make itself known. The symptoms of odontogenic sinusitis are practically no different from rhinogenic sinusitis (when the infection enters through the nose as a result of a cold, flu or acute respiratory viral infection):
- pain and swelling in the sinus area
- nasal congestion and difficulty breathing
- purulent or mucopurulent discharge
- headaches, especially when bending forward
- decreased sense of smell
- temperature up to 39o
An unsuspecting patient first turns to an ENT specialist, but he needs to see a dentist. However, there are points that indicate the odontogenic origin of sinus inflammation:
- pain in the chewing teeth of the upper jaw, especially when chewing
- there was treatment or removal of teeth at the border with the sinuses
- implants or sinus lift were installed
The most important distinguishing feature is that only one sinus is bothering you , which is associated with bad teeth or dental treatment. In this case, first of all, you need to solve dental problems. As a rule, the symptoms of sinusitis disappear within two weeks after eliminating the source of inflammation.
GBOU "NIKIO im. L.I. Sverzhevsky" of the Moscow Department of Health
Etiologically and pathogenetically, the occurrence of chronic odontogenic sinusitis is due to the spread of pathogens from infected teeth, which is facilitated by the anatomical features of the bottom of the maxillary sinus and the roots of the 2nd small and 1st and 2nd large molars. The role of odontogenic infection is especially evident in cases where granulating inflammation of the apex of the tooth root, having destroyed the bone septum between the bottom of the maxillary sinus and the periapical space, involves adjacent areas of the sinus mucosa in the inflammatory process. If a rhinogenic infection is added to this or if there is an insufficiently active function of the drainage opening of the maxillary sinus, the process spreads to the entire mucous membrane of the sinus and takes a chronic course due to the presence of a constant source of infection in the form of an odontogenic infection. In the presence of a perihilar cyst, especially if the apex of the root is located in the lumen of the sinus, the root cyst, due to the presence of free space, quickly increases, filling most of the maxillary sinus).
The spread of infection is also possible through the venous plexus system between the tissues of the alveolar process and the mucous membrane of the maxillary sinus. Odontogenic sinusitis can occur as a result of a suppurating perihilar cyst, as well as osteomyelitis of the alveolar process of the jaw.
The above topographic and anatomical data explain cases of maxillary sinus fistulas communicating with the oral cavity through the socket of an extracted tooth. Long-term non-healing of the socket after extraction of the 2nd small and 1st and 2nd large molars, and with large maxillary sinuses - the 3rd molar, indicates the presence of chronic purulent odontogenic sinusitis. The appearance of odontalgia is explained by the common innervation of part of the mucous membrane of the maxillary sinus and teeth by branches coming from the upper dental plexus, formed in the thickness of the alveolar process of the upper jaw by the anterior or middle and posterior alveolar branches of the maxillary nerve.
Odontogenic sinusitis symptoms are very similar to other types of sinusitis. The only significant difference is in the nature of the disease.
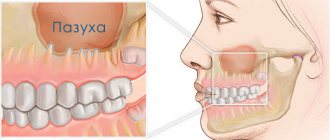
Infection of the upper molar can provoke the development of maxillary sinusitis
Odontogenic sinusitis can be either unilateral or bilateral
According to the type of course, the disease can be acute and chronic (with periodic exacerbations). In addition, odontogenic sinusitis develops either with or without perforation of the sinus floor. In the first case, there are:
- perforations after removal of teeth of the upper jaw, resection of root apices, operations for jaw cysts;
- perforations for specific lesions of the upper jaw;
- destruction of the sinus floor by a growing tumor;
- traumatic perforations.
Sinusitis with traumatic perforation can also develop with the presence of a foreign body. This could be the roots of a diseased molar or filling material. or elements of an intramaxillary implant.
Provoking factors for the development of infection of the nasal mucosa include:
- suppuration of the root cyst;
- periodontitis;
periodontitis;
- perforation of the sinus wall during removal of the upper molar;
- incorrect installation of implants;
Symptoms and signs
Symptoms of odontogenic sinusitis depend on the stage of the disease. The acute form is characterized by the following manifestations:
- moderate pain in the infraorbital region on the side where the infection develops;
- feeling of heaviness in the bridge of the nose;
- pain when pressing on the area of the maxillary sinus;
- pain when biting on the upper teeth on the affected side;
- swelling of the nasal mucosa;
- burning gums;
- purulent discharge in the mouth and nasal cavity;
Characteristic of the acute form of odontogenic sinusitis is a rapid deterioration in health. The patient complains of chills, drowsiness appears, and body temperature rises to 40°C.
The chronic stage is characterized by periodically occurring pain in the area of the inflamed maxillary sinus. In this case, the patient's general condition may remain normal. He continues to lead his usual lifestyle, but periodically complains of nasal discharge with an unpleasant odor. Swelling of the soft tissues of the cheek is usually absent. Biting the offending tooth may cause mild pain.
Exacerbation of chronic odontogenic sinusitis has a similar clinical picture to the acute form of the disease. Often, the patient’s condition worsens after hypothermia, influenza or ARVI.
Diagnostics
When pain and discharge from the sinuses appear, it is important to distinguish odontogenic sinusitis from rhinogenic sinusitis. This can only be done through differential diagnosis, including the following methods:
X-ray examination. Odontogenic sinusitis is characterized by a unilateral decrease in sinus transparency. In addition, it is possible to identify the source of infection in the oral cavity.
X-ray examination is one of the most accurate methods for diagnosing sinusitis
- Examination of the nasal sinuses. The presence of infection may be indicated by swelling of the mucous membrane and purulent discharge.
- Patient interview.
A qualified specialist should know how to distinguish acute single-gene sinusitis from periodontitis, pulpitis or trigeminal neuralgia. Examination of the nature of the symptoms, as well as x-rays of the sinuses, allows an accurate diagnosis.
Treatment
Treatment of the disease requires an integrated approach. Treatment is carried out by two specialists - an oral and maxillofacial surgeon and an ENT doctor. Initially, it is necessary to eliminate the cause of the infection.
The correct choice of sanitation of the teeth of the upper jaw is half the way to success.
The dentist removes the causative tooth, performs resection or amputation of the root, eliminates granulomas or cysts, and treats pulpitis.
Physiotherapeutic procedures will help speed up the recovery process after illness
Possible complications and consequences
The main danger of sinusitis is that the existing infection can penetrate into nearby tissues. If treatment is not done in a timely manner, the risk of developing the following pathologies increases:
- purulent lesions of soft tissues;
- meningitis;
Cancers of the nasal sinuses are often a consequence of chronic odontogenic sinusitis. The only way to protect yourself from serious consequences is to seek medical help in a timely manner .
What is the danger of the disease
Without proper treatment, a chronic inflammatory process with pathogenic microflora develops in the sinus, destroying the sinus mucosa and surrounding bone tissue. Since the maxillary sinuses are located close to anatomically important structures, severe complications can arise:
- Orbital The upper wall of the sinus is in contact with the lower wall of the eye orbit. The infection spreads into the orbit with the formation of an abscess and phlegmon. As a result, optic nerve neuritis develops, deterioration or complete loss of vision.
- Intracranial The most dangerous complications associated with the penetration and impact of infection on the brain. Meningitis, encephalitis, and abscess develop. If detected and treated untimely, irreversible consequences, including death, can occur.
Foci of infection provoked by the presence of a foreign body can cause a precancerous condition.
What are the maxillary sinuses
The maxillary sinuses (also called the maxillary sinuses) are special cavities on both sides of the nose that are filled with air. Each cavity is connected to the nasal passage by small openings called anastomoses. The cavities are covered with mucous membrane. The function of mucus is to trap bacteria and harmful particles in it, and then remove them from the body through those same anastomoses. When edema occurs, the excretory opening becomes very narrow, as a result of which mucus, along with harmful particles and bacteria, cannot come out and stagnates. At this time, the patient begins to experience bursting pain in the cheek area - this is how inflammation of the maxillary sinus begins. Treatment of the maxillary sinus should not be neglected, since inaction can provoke serious consequences, including sepsis and meningitis.
Classic sinusitis can be bilateral, when both sinuses are affected. In the odontogenic form, the inflammatory process starts in the sinus on which side the diseased tooth is located.
Why you should entrust treatment to the ENT department of dentistry
ENT dentistry is a symbiosis of two medical areas, a multidisciplinary approach to the treatment of inflammation of the maxillary sinuses of odontogenic origin. Only an experienced maxillofacial surgeon with ENT training can make an accurate diagnosis and create a sound rehabilitation plan.
As a rule, odontogenic causes of sinusitis are simply ignored during routine examination by an otolaryngologist. Treatment in a city clinic without high-quality diagnostics or in the absence of it at all turns into a multi-part series with monthly visits to an ENT doctor, dragging on for many years, causing inconvenience and worsening the quality of life.
Unified drug therapy or traumatic sinus punctures are prescribed, which, if they bring relief, are for a short time. Inflammation from the acute stage becomes chronic with periodic exacerbations. A person runs from one doctor to another to no avail, but without identifying and eliminating the cause, odontogenic sinusitis cannot be cured !
Odontogenic sinusitis. Who should treat: a dentist or an ENT doctor?
What is odontogenic sinusitis?
This is an inflammation of the mucous membrane of the maxillary sinus, which occurs as a result of the spread of infection from the affected tooth, the tissues around it, or through the communication formed between the oral cavity and the sinus after tooth extraction.
Who should treat odontogenic sinusitis?
Since inflammation of the maxillary sinus is caused by inflammation of the teeth and surrounding tissues, the source of infection must first be eliminated.
This is what dentists do. In some cases, conservative tooth treatment (canal cleaning, filling, etc.) and antibiotic therapy are sufficient. The help of an ENT doctor in such cases comes down to rinsing the sinuses, prescribing medications that ensure the restoration of the patency of the natural openings of the sinuses and their self-cleaning.
However, conservative dental treatment, even with the use of modern microscopes, is not always effective. It is known that the only way to eliminate the source of infection in a tooth 100% is by removing it. Removing the tips of the roots of teeth is currently relegated to the background. As a rule, the roots of 5-7 teeth in the upper jaw border the lower wall of the maxillary sinus. Sometimes the roots of the teeth can stand in the lumen of the maxillary sinus, and the bone plate separating them is very thin or completely absent. When inflammation spreads from the affected tooth to the sinus mucosa, the bone is very often destroyed. Therefore, the removal of such teeth leads to the formation of a communication between the sinus and the oral mucosa - an oroantal fistula.
If such a message is formed as a result of tooth extraction, some dentists recommend waiting until the inflammation subsides and then suturing it. In this case, conservative treatment, antibacterial therapy and lavage of the affected sinus are prescribed. However, in such cases, through the opening from the oral cavity, bacteria can penetrate into the maxillary sinus and maintain inflammation there.
We are of the opinion that it is necessary to simultaneously suturing or closing the communication formed after the removal of the “sick” tooth.
Are there cases when conservative treatment and removal of the causative tooth are ineffective?
Yes, if the patient has prerequisites in the structure of the nasal cavity and paranasal sinuses that interfere with the outflow of mucus from the maxillary sinus and air exchange in it through natural communication. For example, a curvature of the nasal septum, a violation of the anatomy of the middle nasal passage leads to the closure of the natural communication with the sinus and a violation of its self-cleaning.
In such cases, it is necessary for an ENT doctor to act.
We have observations of patients who, after tooth extraction and repeated courses of antibacterial therapy and rinsing of the maxillary sinuses, continued to hurt. Moreover, after restoration of outflow through the natural anastomosis, the inflammation quickly eliminated on its own.
Therefore, if the patient has causes inside the nose that block the natural anastomosis of the maxillary sinus, they must be eliminated surgically. Without this, success cannot be achieved.
Such causes can be detected using computed tomography of the paranasal sinuses or cone-beam tomography in 3 projections.
Conventional x-rays are not informative!!!!!
What should a patient do if sinusitis does not go away?
- It is necessary to do a cone beam tomography or computed tomography of the sinuses in 3 projections.
- Contact your dentist to rule out an odontogenic source of infection.
- Contact an ENT doctor who knows endoscopic techniques for operations on the paranasal sinuses.
In our clinic we use an integrated approach.
Often we simultaneously remove the causative tooth and simultaneously close the communication between the oral cavity and the maxillary sinus after its removal. We correct the causes inside the nose that block the natural anastomosis with the maxillary sinus (we eliminate the curvature of the nasal septum, restore the normal anatomy of the middle nasal passage, expand the blocked natural anastomosis with the sinus).
This operation is performed simultaneously under general anesthesia and allows you to speed up recovery and reduce the percentage of relapses of the disease.
THERE ARE CONTRAINDICATIONS, SPECIALIST CONSULTATION IS REQUIRED
Diagnostics
The odontogenic form of sinusitis often remains undetected by ENT specialists due to the lack of highly accurate diagnostics and banal ignorance of the “dental” cause of the disease. Such gaps lead to the fact that even after medical and surgical treatment the person continues to suffer.
Differential diagnosis is extremely important, which allows you to determine the form of sinusitis and select the appropriate treatment.
Only computed tomography provides informative 3D images for visualizing bone and adjacent soft tissues, the condition of the teeth, the presence of foreign bodies and neoplasms in the sinus.
In our Center, CT scans are performed on a Sirona Gallileos dental tomograph with ENT mode settings.
In some cases, it will be necessary to study the microbial composition of the sinus lining to rule out a malignant process.
How does an infection in a tooth cause the lining of the maxillary sinus to thicken?
The apices of the roots of the teeth are located under the Schneiderian membrane, that is, under the mucous membrane that lines the bottom of the maxillary sinus.
This is the normal anatomical structure of the sinus - when the tops of the teeth are located in it. Some people have the tops of the fourth, fifth, sixth, seventh there. Some people only have the sixth. Some have sixth and fifth. But, one way or another, they are almost always there.
When a tooth is affected by caries, the infection penetrates through the dentinal tubules into the pulp chamber. Through it, the infection slowly progresses further through the blood and lymphatic vessels into the periodontium of the tooth.
Pulp microvessels emerge from the periodontium directly under the mucous membrane of the sinus, and over time it begins to react with inflammation.
Immune system cells responsible for protecting against infection initiate chronic inflammation. And the mucous membrane gradually thickens. This irritation happens all the time.
Infection from the carious process, which is thus restrained by immunocytes, causes a gradual degeneration of the structure of the sinus lining in the form of polyps and cysts.
Stages of treatment
We strive to carry out all activities comprehensively in one day, so as not to delay the patient
- Sanitation of the oral cavity Preparation to maintain sterility during surgery to avoid secondary infection - retreatment of compromised teeth, hygienic cleaning.
- The operation is performed by a maxillofacial surgeon in a sterile operating room of the ENT department - “in your sleep”, according to the selected access protocol. A follow-up CT scan after surgery is required.
- Prosthetics If the protocol requires the removal of teeth, we install temporary orthopedic structures to close the aesthetic defect so as not to leave the patient without teeth.
Recovery after surgery
No hospitalization
A hospital stay for 2-3 days after surgery (as happens in city hospitals) is not required.
Gentle surgical protocols, the use of modern functional equipment and a microscope allow treatment to be carried out as delicately as possible .
All operations are performed in a controlled, drug-induced sleep - this is not general anesthesia ! Recovery from the state is easy, without dizziness, memory loss or clouding of consciousness. The drugs are absolutely safe for the body and are eliminated naturally 40 minutes after stopping the supply.
For patients with vascular and cardiac problems, a day hospital , where you can calmly recover and recover under the supervision of our anesthesiologist-resuscitator.
Accelerated rehabilitation
Recovery after the intervention occurs within a week. For those who want to speed up the process, our Center provides a set of procedures to reduce pain, resolve hematomas and swelling - carried out on the day of surgery.
Home care
Medications are prescribed - antibiotics, painkillers and decongestants. To prevent the patient from running to pharmacies in a postoperative state and to avoid purchasing counterfeit products “on the side,” the entire package of drugs is collected and given out free of charge .
The package contains all the necessary medications for taking and caring for the surgical area.
Please follow the recommendations and do not skip taking medications to avoid complications. The instructions are in the medicine package.
If you suspect a worsening condition, contact the clinic immediately. The telephone number for the 24-hour patient support service is listed in the memo.
How does maxillary sinusitis manifest?
When visiting an ENT doctor, patients usually complain of heaviness, sometimes pain or swelling of the soft tissues in the area of one maxillary sinus, prolonged runny nose, hyposmia (decreased sense of smell) or, conversely, a constant unpleasant odor in the nose. Often such patients report frequent and painful sinusitis, multiple punctures, numerous courses of antibiotics, which brought only a temporary improvement in their condition or did not help at all. And only with a detailed collection of the medical history is it possible to find out about the recent or long-standing treatment of the “causal” teeth by the dentist, namely “7s”, “6s” or “8s” of the upper jaw of the corresponding side. But it happens the other way around: the patient does not make any complaints, but when preparing for dental prosthetics or sinus lifting, the dentist identifies pathology of the maxillary sinus on a computer tomogram and refers it to an ENT specialist. The reason for such careful preparation and alertness of our colleagues is the golden rule of planned surgery - the absence of inflammatory changes in the surgical area, because otherwise there is a high risk of implant rejection, scarring and a generally worse outcome of the operation.