What is a dental cyst?
Tooth cyst - what is it? An odontogenic cyst is a pathological neoplasm that occurs in the upper part of the tooth root. The internal cavity of the cyst is filled with liquid or mushy purulent contents; it is enveloped by a dense layer of epithelium.
The size of the cyst starts from a few millimeters, with rapid development reaching several centimeters in circumference. Most often, the pathological process affects the upper jaw, since the roots of its teeth have a more porous structure.
In order to understand what a dental cyst is and how to treat it, you need to know why such a phenomenon occurs. The formation of cysts occurs as a result of inflammation, thus the body restricts healthy tissue from the affected areas, clogging them along with bacteria into bubbles.
Causes
There are several reasons why a dental cyst develops. The main reason is the activity of pathogenic microorganisms in a closed dental space; the following risk factors contribute to this:
- severe pathology, lack of timely treatment and incorrect treatment of dental diseases - caries, periodontitis, pulpitis;
- infectious complications after tooth filling, implantation procedures - in such cases, the doctor removes not only the cyst, but also the crown or implant, this avoids relapse;
- complications during teething, especially when wisdom teeth erupt - dental tissues injure the gums, bacteria get into microcracks,
- microorganisms also enter wounds that form due to mechanical damage to teeth;
- Nasopharyngeal diseases – infections in the nose and throat can spread to the oral cavity.
To provide adequate treatment, it is necessary to accurately determine the cause of the development of a dental cyst; based on it, the dentist will prescribe suitable therapy. So, in cases of injury, treatment consists of removing the cyst and tissue regeneration, but if the cyst is a complication of another disease, then in addition to removing the vesicle, the patient will be prescribed treatment for the underlying disease.
2. Reasons
The most common cause of a hilar cyst is the aforementioned periodontitis. Turning again to statistics, we note the predominance of patients aged 20 to 45 years: this age category most often suffers from caries and its inflammatory complications.
Other risk factors for radicular cysts include trauma, careless or illiterate canal filling (alas), as well as hereditary or idiopathic predisposition.
Visit our Microsurgery page
Types of dental cysts
Tooth cysts have different classifications, each of which is formed according to certain characteristic parameters of the pathology.
According to the nature of the disease, they are distinguished:
- residual cysts – occur after tooth resection (removal) surgery; this is the most common type of cyst;
- retromolar – formed during severe eruption of wisdom teeth;
- radicular - cysts are located on or near the tooth root;
- follicular – at the heart of such cysts is the germ of a permanent tooth; follicular neoplasms arise as a result of poor quality care of baby teeth.
Classification of neoplasms according to their origin:
- odontogenic – arise as a result of the transition of the inflammatory process from other dental diseases;
- non-odontogenic - the causes of the development of such cysts include problems not related to the teeth and oral cavity.
Locations of cystic formation:
- anterior teeth;
- teeth that are adjacent to the nasal sinuses with their roots;
- wisdom teeth.
Timofeev 1-3 volume / volume 3 / 25. JAW CYSTS / 25.1. RADICULAR CYSTS
25.1. RADICULAR CYSTS
Radicular cysts of the jaws are the most common and occur with the development of a chronic inflammatory process around the root of the tooth. When analyzing our own clinical observations (1000 jaw cysts), it was revealed that radicular cysts occurred in 85% of cases. They are found almost equally often in both men and women. The largest number of cysts are found between the ages of 20 and 45 years. This is due to the fact that in this age period, teeth are most often affected by the carious process, complicated by inflammatory changes in the periapical tissues. Radicular cysts on the upper jaw are somewhat more common than on the lower jaw, respectively: 56% (on the upper jaw) and 44% (on the lower jaw).
Radicular cysts occur
as a result of the presence of a chronic inflammatory process in the periodontium. It is known that Malyasse (1885) and N.A. Astakhov (1908) discovered epithelial cell islands on the inner surface of the periodontium in almost every tooth, which persist throughout the entire period of life. As a result of the irritating effect of the inflammatory process, in some cases, proliferation of epithelial cells occurs, which can line the cavity of the perihilar granuloma, followed by the formation of a cyst. In other cases, under the influence of chemicals formed during inflammation, epithelial cells multiply and grow, forming microscopic cavities. The latter gradually fill with cystic contents, increase in size, burst and merge into a single cystic formation.
Rice. 25.1.1.
Development of a radicular cyst. Stage of cystogranuloma (a, b).
Cyst growth occurs slowly, due to an increase in the volume of cystic contents, which causes pressure on the surrounding bone and leads to atrophy of the latter (Fig. 25.1.1).
A bone defect may form in the jaw and the cyst continues to grow under the periosteum
(subperiosteal
cyst). The cyst grows due to the higher pressure of the cystic fluid than in the bone.
Pathomorphology.
The cyst shell is represented by connective tissue, which is directly adjacent to the surrounding bone, and from the inside it is lined with epithelium. The epithelial lining is most often built according to the type of multilayered squamous epithelium of the oral cavity without its complete keratinization. In rare cases, cysts may be lined by columnar, cuboidal, or ciliated epithelium. In the shell of a radicular cyst, microscopically it is always possible to detect inflammatory changes that are expressed to varying degrees. Inflammatory phenomena lead to erosion of the epithelium followed by necrosis of part or all of the membrane. When morphologically studying the cyst shell, in some cases, it is possible to detect the epithelial lining only in certain areas.
Characteristic features of the structure of radicular cysts include the presence of cholesterol in their contents and walls. Its appearance is associated with the breakdown of cellular structures rich in lipids. With repeated exacerbations (suppuration) of the cysts, inflammatory changes are observed in the bone surrounding the cystic membrane.
Clinic.
Complaints from patients with radicular cysts may be absent, because
are asymptomatic, and its detection is often an accidental finding during dental radiography during treatment. In other cases, complaints boil down to the presence of jaw deformation or fistulas on the alveolar process. When cysts suppurate, the general condition worsens, symptoms of intoxication and other signs of the inflammatory process (pain, etc.) appear. Therefore, cysts are often detected during suppuration. Compression of the neurovascular bundle in the lower jaw can cause Vincent's symptom
(paresthesia of the lower lip).
Jaw cysts rarely cause facial deformity. This largely depends on their location. More often, facial asymmetry can occur in the presence of cysts in the frontal region of the upper and lower jaws. When a cyst grows from the central incisors of the upper jaw towards the nasal cavity, a Gerber's ridge
- protrusion in the lower nasal meatus, detected during rhinoscopy.
Rice. 25.1.2.
Appearance of a patient with a radicular cyst of the upper jaw on the left.
When examining the oral cavity, a smoothness or bulging of the rounded shape of the anterior wall of the jaw in the area of the transitional fold is determined. Palpation of the deformity is painless, the boundaries of the bulge are clear. When a cyst develops from a tooth whose root faces the palate (lateral incisor, second premolar, first molar), thinning and sometimes resorption of the palatal plate of the upper jaw is observed. A limited hemispherical protrusion is palpable on the palate (Fig. 25.1.2).
Rice. 25.1.3.
Radiographs of patients with radicular cysts localized on the lower jaw (a, b, c, d).
Cysts in the area of large molars often grow towards the maxillary sinus without causing visible deformation of the jaw. When cysts are localized in the area of the angle and ramus of the lower jaw, deformation of the latter is observed only when the tumor-like formation is very large. If the cyst comes from the roots of the second or third molar of the mandible, then it may be located closer to the lingual surface, because on the other side there is a thick layer of compact and spongy bone. The neurovascular bundle on the lower jaw is pushed aside by the cyst as it grows and is not involved in the pathological process.
On palpation, the bone tissue above the cyst may bend and crack when pressed, i.e. a “parchment crunch” appears (Dupuytren’s symptom).
A prerequisite for its appearance is the presence of a bone defect on the opposite side to the area of the bone being pressed. Dupuytren's sign is possible when the cyst grows into the maxillary sinus (nasal cavity). The fluid that fills the cystic cavity with this symptom must change its volume inside the bone tissue, and this is only possible if it is displaced. The symptom of “parchment crunch” was described by Dupuytren as one of the signs of bone sarcoma. It occurs not only with cysts, but also with cystic forms of benign tumors of the jaws (ameloblastoma, osteoblastoma).
If there is a defect in the jaw bone, a bone window is palpated under the mucous membrane, and a fluctuation is determined in its center. The mucous membrane in the area of the perforated area of the bone is not changed in color. The causative tooth usually has a carious cavity and dead pulp. Convergence may be observed
(convergence, rapprochement) of the crowns of adjacent teeth. Other teeth located in the cyst area have reduced electrical excitability. During tooth treatment, the pulp extractor can penetrate beyond the root apex and a clear, straw-yellow liquid is released through the root canal. When a tooth is removed, this fluid is released through the socket. By probing (with a button probe), the doctor penetrates into the cavity of the cyst.
Rice. 25.1.4.
Radiographs of the lower jaw of children with radicular cysts from baby teeth (a, b, c). Residual cysts of the jaws (d, e).
Rice. 25.1.5.
Radiographs of the upper jaw of patients with
radicular cysts (a, b, c, d, e).
Rice. 25.1.5.
(continued - f, g).
Rice. 25.1.6.
X-ray of the upper jaw of a patient with multiple radicular cysts of the upper jaw.
Suppuration of a radicular cyst is accompanied by signs of inflammation: increased body temperature, pain, swelling, hyperemia of the mucous membrane in the area of the cyst and other symptoms. Periostitis, osteomyelitis, regional lymphadenitis, fistulas, purulent-inflammatory processes in soft tissues, and sinusitis may occur.
X-ray picture
cysts are characterized by the presence of a homogeneous area of rarefied bone tissue of a rounded shape with clear boundaries - a rim of cortical bone tissue
(Fig. 25.1.3-25.1.6).
The boundaries of the cyst (radiologically) are less clear in the presence (history) of periodic exacerbations of inflammatory phenomena in the area of the cyst, i.e.
the presence of osteomyelitic bone lesions. The root of the causative tooth faces the cystic cavity; its periodontal fissure on the side of the cyst is not contoured (absent). The root of the causative tooth located in the cyst cavity does not undergo resorption. The roots of adjacent teeth may diverge
(diverge). The relationship between tooth roots and cysts can be very different.
If the root of the causative tooth is located close to the outer surface of the jaw, then as the cystogranuloma grows, the latter grows into the bone and grows under the periosteum, i.e. subperiosteal (subperiosteal) occurs
cyst.
Rice. 25.1.7.
Radiographs of the lower jaw of patients with residual cysts (a, b, c, d).
Rice. 25.1.8.
Radiographs of the upper jaw of patients with residual cysts (a, b).
Rice. 25.1.9.
Radiographs of a patient with a radicular cyst of the upper jaw that has grown into the maxillary sinus. Sighting (a) and paranasal sinuses (b).
When a cyst grows under the periosteum, it is determined in the form of a painless protrusion, covered with unchanged mucous membrane. When palpating the cyst, fluctuation is detected. When performing an X-ray of the jaw, with a subperiosteal cyst, it is not possible to detect the characteristic X-ray picture of the cyst. An x-ray often reveals changes in the area of the apex of the tooth root, which are typical for chronic periodontitis (granulomas), and a rim of sclerotic bone is sometimes visible along the boundaries of the cyst.
Quite often, pneumatization of the maxillary sinus can simulate a maxillary cyst on an x-ray. In this case, it is first necessary to identify the clinical signs of a subperiosteal cyst, and in their absence, the condition of the periodontium of the teeth projecting onto the maxillary sinus is determined. In the absence of a radicular cyst, the periodontium of these teeth is not changed. It should be remembered that on a radiograph the borders of the maxillary sinus are always intense and are presented in the form of bays.
If, after the removal of the causative tooth, the cyst remains unrecognized and its growth continues, then these cysts are called residual.
Residual cysts can be on both the upper and lower jaws
(Fig. 25.1.7 - 25.1.8).
Residual cysts sometimes reach large sizes and reduce bone strength, contributing to the development of a fracture at the slightest trauma to the lower jaw. The roots of the teeth projecting onto the area of such a cyst retain an intact periodontal gap.
When a radicular cyst grows into the maxillary sinus or into the nasal cavity, its clinical symptoms change. In the lower nasal meatus, you can find a protrusion called Gerber's cushion.
There is a feeling of heaviness in the area of the corresponding maxillary bone, nasal congestion, decreased sense of smell or difficulty in nasal breathing on the affected side. The last symptom appears only when the cyst grows into the nasal cavity. The cyst can grow from the side of the hard palate. Then the protrusion can be detected from the bottom of the right or left nasal passage.
On an x-ray of the paranasal sinuses, you can see a dome-shaped stretching, which is projected onto the area of the maxillary cavity; there is a displacement of the bone floor of the sinus (Fig. 25.1.9).
To clarify the diagnosis, it is contrasted with radiopaque substances (iodolipol, verografin, urografin, etc.) or a computed tomography scan of the maxillary bone is performed
(Fig. 25.1.10).
Rice. 25.1.10.
Computed tomogram of a patient with a radicular cyst of the upper jaw (tomogram was made at different levels - a, b, c).
In children
Most often, radicular cysts are localized on the lower jaw.
Their clinical symptoms are typical, but they appear in children earlier than in adults. The most common cause of the development of cysts is the primary
molars of the lower jaw.
Cysts emanating from these teeth, in the process of growing in the thickness of the jaw, “grab” the rudiments of permanent premolars, the follicles of which are formed already at the age of 2-3 years. Thus, on an x-ray of the lower jaw, you can see how the cyst shell “envelops” the coronal part or the entire tooth germ (in some cases, two tooth germs), i.e. the follicle is located, as it were, in a cystic cavity (Fig. 25.1.4).
The rudiments of permanent premolars, as the cyst grows, are shifted to the side (pushed to the periphery of the jaw) due to the pressure that exists in the cystic cavity. All this resembles the symptoms of a follicular cyst. The definitive diagnosis of a radicular cyst is made during its removal. When the cavity of the cyst is opened, the crown of the tooth is not found in it, but only the reliefs of the rudiments of permanent teeth, which are covered with a cystic membrane, are visible. During puncture of the cyst, an opalescent clear liquid (with cholesterol crystals) may be obtained.
A radicular cyst in children can also form from constant
(destroyed) tooth. Clinical signs are common in children and adults. As the cyst grows, the mandibular canal is pushed toward the lower edge of the jaw, the roots of the teeth move apart, and jaw deformation appears. In some cases, due to painless growth, cysts in children remain unrecognized for a long time. They are often detected only when facial asymmetry appears, as well as accidentally during dental treatment or radiography.
Rice. 25.1.11.
X-ray of the lower jaw of a patient with recurrent periostitis.
In old age,
in people who use removable dentures, opaque or amber-colored liquid can be found in the punctate of the radicular cyst, and the contents are brown. The brown color of the cyst fluid is due to hemosiderin crystals, which are formed due to repeated hemorrhages into the cyst cavity. These hemorrhages occur as a result of tissue trauma caused by a removable denture. When the cyst suppurates, pus appears in the punctate, and cholesterol crystals dissolve.
Differential diagnosis
carried out with other types of jaw cysts and with cystic forms of tumors of the jaw bones.
First, let's focus on the so-called non-sheathed (traumatic)
cysts.
In my opinion, this is not an entirely accurate definition, because... the cavity is more often formed as a result of pressure on the bone due to the organized subperiosteal hematoma that occurs after injury. In this case, more correctly, this formation should be called rarefied periostitis.
The latter is more often found in the mental part of the lower jaw, although it can also be detected in other parts of it,
as
well as in the upper jaw.
The radiograph of the lower jaw shows a homogeneous loss of bone tissue in the mental region (Fig. 25.1.11)
with fairly clear boundaries. Intact teeth face the rarefaction zone.
When performing surgery, after detachment of the mucoperiosteal flap, in the rarefaction projection on the deformed area of the bone, the formation of a conglomerate of fibrous (scar) tissue is detected. The contents of this formation are always represented by connective tissue with a small amount of serous fluid and clotted blood. Intact teeth face the cavity. There is no intraosseous cavity, but there is a defect in the outer cortical plate with exposure of the roots of intact teeth.
It is extremely rare to encounter intraosseous hemorrhages,
which did not manifest themselves clinically and were an accidental finding during dental x-rays.
X-ray is determined by a homogeneous rarefaction of bone tissue with intact teeth located in it. Detachment of the mucoperiosteal flap exposes unchanged bone, and after its perforation one can find an intraosseous cavity filled with serous fluid, disintegrated or organized hematoma. The wall of the formation is represented by connective tissue. In the latter case, we can talk about a traumatic (non-shelled)
cyst.
Follicular
cysts are much more often detected in children and young adults. They are not associated with gangrenous teeth. On the radiograph, the cyst cavity contains the crown of an impacted formed or unformed permanent tooth. There is no permanent tooth in the dental arch or its place is taken by a baby tooth. When the cystic membrane is removed, it is discovered that it is attached strictly along the neck of an unerupted and atypically located tooth.
Paradental cysts are most often associated with difficult eruption of the lower wisdom tooth, although in rare cases they can be associated with any tooth.
Epidermoid
jaw cysts can manifest themselves either as polycysts, which are located in the area of the body and branches of the lower jaw, or as single-cavity cysts. The shell of these cysts is thin; upon puncture, pasty contents can be detected.
Fissural
cysts are not associated with gangrenous teeth and have a characteristic location.
Nasolabial (incisive canal)
cysts are located strictly along the midline (in any part of the incisive canal),
nasolabial cysts
- in the area of the nasolabial groove under the base of the nasal wing,
globulomaxillary cysts
- between the erupted lateral incisor and the maxillary canine.
For ameloblastoma
Characterized by localization in the area of the angle and body of the lower jaw, lack of connection with the periodontitis tooth. On X-ray it is revealed both as a polycystoma and as a single-chamber cystic formation. An unerupted wisdom tooth may be present in the ameloblastoma cavity. During puncture, you can often get a whitish, cloudy and viscous fluid, but occasionally its contents can resemble cystic fluid with the presence of cholesterol crystals. The final diagnosis is established only on the basis of a pathohistological examination.
Osteoblastoma may resemble a cyst, but unlike it, it has a bumpy surface. On an x-ray, the tumor often has a cellular structure (in the form of “soap foam” or “honeycomb”). The boundaries of the formation are less clear than those of a cyst. The roots of teeth located in the tumor zone are more likely to undergo resorption. In some cases, osteoblastoma appears as a single-chamber cystic formation with clear boundaries. During puncture, a small amount of bloody-brown fluid that does not contain cholesterol may be obtained. Macroscopically, the tumor is brown in color and bleeds profusely.
Differential diagnosis of cysts with other, more rare benign neoplasms, as well as with malignant tumors of the jaws, will be discussed in the relevant sections of this manual.
Symptoms
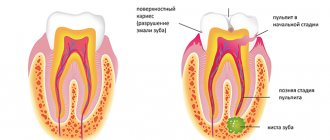
The danger of a dental cyst lies in the fact that signs of pathology appear only when the neoplasm reaches a relatively large size. In the early stages, small cysts do not manifest themselves in any way, meanwhile the infectious process covers an increasingly larger area of healthy tissue. In the initial development of pathology, cysts are discovered by chance during routine examinations or treatment of other diseases.
The duration of the formation of a dental cyst takes only 1-2 days; as it develops, the following symptoms may occur:
- unpleasant and even painful sensations in the tooth, which intensify when chewing solid food;
- protrusion of the gum of a tooth, in the area of the root of which a cyst forms, the growth of the gum becomes larger over time, redness is observed;
- the formation of a fistula in the area above the root of the tooth, the release of serous or purulent accumulations from it;
- general weakness and malaise;
- increase in body temperature.
Note! When a dental cyst occurs, the symptoms are not immediately visible; they appear in the later stages of development. The pain when a tumor appears is aching in nature, but it is less pronounced than the pain caused by caries and pulpitis.
If a clinical picture occurs and you suspect a pathological process, be sure to consult a doctor. Under no circumstances should you resort to self-treatment - the dental cyst must be removed. In addition, taking the wrong medications can worsen the patient’s overall well-being.
Sometimes there is no pain in the oral cavity; instead, the basis of the clinical picture is intense headaches. The cause of this phenomenon may be a cystic formation in the maxillary sinus.
Why do jaw cysts form?
Odontogenic cysts (developing or inflammatory) get their name from the nature of their origin. Most jaw cysts are lined by epithelium, which is derived from odontogenic epithelium.
The occurrence of such cysts is usually associated with unerupted teeth (third molars of the lower or upper jaw, second premolars of the lower jaw, and canines of the upper jaw). They can also form near additional teeth and in combination with odontomas. The occurrence of odontogenic cysts is rarely associated with baby teeth.
Most often, jaw cysts are discovered between the ages of 10 and 30 years. Men, especially white-skinned men, suffer from them more often.
In most cases, dental cysts do not manifest themselves in any way and are an accidental finding obtained during an X-ray examination. But, in some cases, they can reach significant sizes, which lead to the expansion of bone tissue, but even they may not give pronounced symptoms until a secondary infection occurs.
Consequences
Without adequate treatment, the dental cyst continues to grow and develop; in advanced stages, large neoplasms destroy the bone tissue of the skull, as a result it is replaced by connective tissue formations, which leads to the development of the following complications:
- dissolution of the jaw bone, which depends on the growth of the cyst;
- the formation of pus in the cyst, further purulent inflammation can lead to the development of an abscess;
- inflammatory process of lymph nodes located near the source of infection;
- development of osteomyelitis or periostitis;
- development of chronic sinusitis when the cyst grows in the maxillary sinus;
- pathological fracture of the jaw bones when the cyst reaches a large size;
- development of phlegmon due to a long-term purulent inflammatory process in the cyst;
- sepsis – blood poisoning;
- degeneration of a cyst into a malignant tumor without timely treatment.
Many patients are interested in why a dental cyst appears in the maxillary sinus, how dangerous it is and its symptoms. The formation of a cyst of this type occurs as a result of untreated inflammation of the tooth root in the upper jaw. A granuloma forms at the root of the tooth, which increases in size and becomes a peri-radicular cyst, then takes a position in the maxillary sinus. The volume of such a cyst can reach 9-12 cubic centimeters.
The symptomatic picture includes painful sensations, the nature of which is similar to trigeminal neuralgia, pain in the occipital, temporal and parietal regions of the head. Externally, a dental cyst can be identified by the asymmetry of the face. Tooth cyst - photo shows a cyst in the maxillary sinus.
Diagnostic methods
After the patient contacts the dentist, a planned additional examination is prescribed, which will help identify the dental cyst in the upper jaw from other maxillofacial tumors and pathological changes. Among the main ones it is worth highlighting the following:
X-ray examination. On an x-ray, the cyst appears as a small oval or spherical shadow with clear outlines. The shadow is located at the top of the tooth root closer to its side. The periodontal gap is not displayed on the image, but significant destruction of the bone structure in the affected area is detected. Electroodontometry. The method is used when it is impossible to differentiate a radicular cyst on an x-ray. The excitability threshold of the affected tooth varies from 90 to 120 μA. Such indicators correspond to necrotic development of the pulp. Puncture. A puncture with a thick needle is performed to reliably exclude the malignancy of the cystic component. The contents of the cyst are sent for cytological examination.
A radicular cyst of the lower jaw bone is almost no different from the flow in the upper segments of the jaw. Often a radicular cyst is similar to osteoblastoma, but the main difference between a cyst is the absence of a cellular structure and the presence of clear contours of shadows in the projection image. Differential diagnosis allows you to reliably identify the disease and treat it according to accepted medical tactics.
Diagnosis of tooth root cyst
To make a diagnosis and carry out appropriate treatment, the dentist collects and analyzes the medical history. During the initial diagnosis, many patients report the fact of endodontic treatment performed to eliminate periodontitis or pulpitis. Some patients indicate an exacerbation of the disease after intraoral dissection.
Radiography is used as the main diagnostic method. Below is a photo and x-ray of a dental cyst.
To obtain an x-ray, several methods are used, the first method is based on contact intraoral x-ray, the advantages of this technique:
- determining the degree of destruction of the jaw bones;
- assessment of the condition of the tooth root and tooth canal;
- assessment of the quality of canal filling;
- identifying the presence of perforations and fragments of instruments and materials in the tooth canal;
- determination of the relationship between the cyst and the roots located near the teeth.
The second method of performing radiography is an orthopantogram; the procedure is a panoramic photograph of both jaws and the maxillary sinuses of the upper jaw.
Another method of the procedure is a survey X-ray in the nasomental projection; the X-ray covers the bones of the skull from the nose to the chin; using the image, the doctor assesses the condition of the maxillary sinuses and detects cysts that have grown into the nasal cavity.
In addition to radiography, to detect a tumor, the patient may be prescribed an electroodontic diagnostic procedure. This technique helps to assess the degree of such an indicator as the electrical excitability of the teeth that are located next to the cystic tooth. If the value exceeds 60 microamps, the dentist prescribes endodontic treatment to the patient.
For diagnostic purposes, histological and cytological studies are used to determine whether the neoplasm is benign or malignant.
Diagnosing a dental cyst is not difficult, but only qualified dentists can carry it out in a hospital setting; under no circumstances try to independently determine the presence of a cyst and do not take therapeutic measures; strictly follow the doctor’s recommendations.
Treatment
Treatment of dental cysts is carried out through surgery, laser treatment and conservative therapy. The latter has a positive effect only in the initial stages of the disease; overgrown cysts must be removed.
Surgery
To eliminate the pathology, it is not necessary to remove the entire tooth; only the tooth root on which the cyst is located is subject to resection. After removing the affected area, the dentist seals the remaining root, treats the surgical canal through which he removed the bladder with its contents, and stitches it up.
After a few days, the doctor removes the stitches and monitors the wound healing process. It is important to make sure that there are no cyst particles left in the dental canal; to achieve this goal, repeat radiography is performed.
Note! Sometimes it is impossible to remove the root along with the cyst; in these cases, the doctor completely removes the tooth. Indications for complete tooth resection are a difficult-to-reach location of the cyst and a severe course of the disease.
After surgical removal of a cyst, the patient must regularly visit the dentist and follow the recommendations prescribed by the doctor.
Conservative therapy
Tooth cyst - treatment of the disease with conservative methods is possible only in the early stages of its development. In order to eliminate the tumor, the patient is prescribed injections and rinses.
During therapeutic treatment, the dentist opens the dental canal, which leads to a cystic neoplasm, and pumps out exudate from it. The doctor does not fill the canal for ten days; during this period, the patient uses antiseptic solutions and tinctures to rinse the mouth.
Upon completion of the treatment course, the dentist treats the dental canal with medications and then fills the tooth.
Laser removal
Laser treatment is a modern method of treating dental cysts. When performing the method, the doctor opens the dental canal and uses laser irradiation to treat the area where the cystic tumor is located. The laser destroys not only the epithelium of the cyst, but also hundreds of thousands of bacteria that are inside the bladder.
The advantages of laser removal are rapid tissue healing and no risk of secondary infection in the oral cavity and dental canal.
Treatment with antibiotics
In some cases, dental cysts are treated with antibiotics. Taking antibacterial drugs is an auxiliary measure to destroy an expanded infection or the main method of treatment if a dental cyst develops against the background of a primary infectious disease.
Antibacterial drugs can only be prescribed by the attending physician; the following drugs are most often used:
- amoxicillin – has a high antibacterial effect, greatly facilitates the treatment of cysts with other methods;
- Cifroploxacin is a broad-spectrum antibiotic that actively destroys bacteria and relieves inflammation;
- tetracycline - this drug is prescribed more often than others, it actively relieves the inflammatory process, pain syndrome, and facilitates other methods of treating dental cysts.
Sometimes a doctor can prescribe topical antibacterial agents to a patient, but taking such medications is not always advisable - local drugs - antibiotics are quite difficult to distribute evenly over the diseased area.
Note! Antibacterial drugs are potent drugs that also affect beneficial bacteria in the body. You can take such medications only as prescribed by a doctor, without increasing the number of doses or dosage.
Treatment at home
Treatment of dental cysts at home is possible only as an auxiliary therapy. A cyst should not be confused with a granuloma; the latter can resolve on its own, but the cystic formation must be radically removed. Home treatment is not used to remove the cyst, but to eliminate the inflammatory process and destroy harmful bacteria.
The main goal of therapy at home is to provide an antiseptic effect. Propolis tincture, calendula tincture, eucalyptus tincture have an antiseptic effect. Tinctures are used as follows: a small amount of medicine is applied to a cotton swab and applied to the affected area, held for 5-10 minutes.
Medicines with an antiseptic effect can be used before surgery to remove a cyst and after tooth root removal. The antiseptic effect allows these medications to be used in the treatment of caries and other infectious diseases of the oral cavity.
Prevention
It is always easier and faster to prevent any disease than to cure it, so one should not forget about simple preventive rules that will help avoid the development of a dental cyst. The basic rules for preventing dental cysts are based on compliance with the rules of oral care.
How to prevent the formation of pathology:
- do not trigger the course of dental diseases such as caries, periodontitis, pulpitis; if infections occur, consult a doctor immediately;
- Brush your teeth daily and prevent the appearance of plaque, which can later transform into tartar;
- monitor the condition of the teeth and oral cavity after operations and mechanical injuries;
- visit your dentist regularly;
- monitor the condition of filled teeth and dental implants;
Patients who have had their teeth filled or have dental crowns or implants placed are advised to periodically have dental x-rays taken. This will allow timely detection of pathological changes and increase the chances of successful recovery without serious consequences.
Note! All diseases must be treated in a timely manner; inflammatory processes reduce immunity, as a result of which infections move freely from one organ to another; in addition, secondary infections can be added to already developed pathologies. It is important to monitor your health and strengthen local and general immunity.
To strengthen your immune system, strengthen your body, include fresh fruits and vegetables in your diet, play sports and walk outdoors more often. It is more difficult for any infection to get into a hardened body than into a weakened body.
4.Treatment
The most common methods of treating cysts are cystotomy and cystectomy. The first is more gentle (and strictly speaking, less effective): cystotomy is aimed at depressurizing the cyst and eliminating excess pressure, which not only deforms the surrounding tissues, but also promotes the growth of the cyst itself. Special obturators are used to prevent rapid closure of the surgical opening.
If the cyst is large or gigantic, cystotomy is often an intermediate step before cystectomy - radical removal of the cyst along with the membrane (and the tooth, or even more than one). If the size is relatively small, resection of the root apex can be performed with further antiseptic treatment and drainage. In complicated and severe cases, in fact, maxillofacial surgery is performed with access through the bone wall; since a long-existing cyst can lead to serious deformation of facial proportions and the formation of extensive defects, the question of plastic correction, replacement transplantation, dentures, etc. is raised.
However, all these methods, no matter how much they are improved and no matter how much they are honed by world dental and maxillofacial surgery, are significantly worse than the simplest and most effective method that everyone knows about: not finishing. But knowing and implementing are still not the same thing, so it wouldn’t hurt to repeat for the millionth time: regular visits to the dentist, even if nothing hurts, can prevent the most serious problems and complications.