The incidence of acute respiratory diseases (ARI) and their high prevalence in children are a serious problem for healthcare in Russia [1]. The pathological process during acute respiratory infection can involve both the upper and lower respiratory tracts. Etiological factors represent a polyetiological group of infections, among which in children the proportion of viruses is 65-90% [2-4]. The most common bacterial pathogens detected in acute respiratory infections in children are Str. pneumoniae, H. influenzae, Str. pyogenes, Staph, aureus, M. catarrhalis
[5]. The role of bacterial flora in the development of complications and recurrent respiratory diseases in frequently ill children is especially high [6].
In children, a complicated course of acute respiratory diseases is much more often recorded in the form of inflammatory diseases of the nasal cavity, pharynx, larynx, trachea, which have a recurrent course. Currently, the treatment of these diseases is effective when using, first of all, antiseptic agents in combination with symptomatic drugs [7, 8] and physical factors [9-11].
One of the pressing problems of modern physiotherapy is the development of technologies that allow the administration of drugs using hardware physiotherapy methods [12].
An effective method for treating diseases of the upper respiratory tract is aerosol therapy in the form of inhalation of medicinal substances that have higher chemical and physical activity than conventional liquid drugs due to an increase in the total surface of the dispersed phase.
In recent years, a new generation antiseptic, Miramistin, has been widely used, which has pronounced activity against a number of microbes - viruses, bacteria, fungi.
The purpose of the study was to scientifically substantiate the possibility of using Miramistin solution in children with acute respiratory diseases using physiotherapy technologies and increasing the effectiveness of complex treatment.
Material and methods
Clinical observations and comparative studies were carried out in 60 children with acute respiratory diseases who received inhalation of miramistin solution through a nebulizer (40 children) and in the form of a spray (20 children - control group) 2 times a day for 10 days. Inhalations were carried out through a mask using a nebulizer using 3-4 ml of a standard 0.01% aqueous solution of Miramistin. Irrigation of the pharynx was carried out with a 0.01% solution of miramistin in the form of a spray.
The effectiveness of Miramistin was assessed on the basis of dynamic observation data in accordance with the results of various research methods (general blood count, rhinoscopy, pharyngoscopy, assessment of the dynamics of subjective complaints using a sensory analogue scale (SAS) on a 10-point system, examination of external respiratory function, monitoring peak expiratory flow, studying the level of physical development and physical fitness of children).
The studies were conducted in accordance with the requirements of the Declaration of Helsinki. Statistical processing of the study results was carried out using standard computer programs Statistika 7.0 and SPSS 15.0.
Adviсe
- Since in most cases a runny nose is caused by viruses, Miramistin will be ineffective . To confirm that a child has ARVI, it is important to consult a doctor and not give any medications until the baby is examined by a specialist.
- Miramistin in ointment form should not be used to treat a runny nose. Due to the fatty base, such an ointment will disrupt the functioning of the epithelium and will interfere with the removal of mucus, which will only worsen the course of a runny nose.
- If treatment with miramistin does not help eliminate the runny nose within 4-7 days, be sure to contact your pediatrician to find another drug.
Results and discussion
Before the start of the study, 45 (78.3%) children complained of poor health and malaise. In 24 (40.0%) children, rhinitis was complicated by symptoms of catarrhal sinusitis: difficulty nasal breathing, heaviness and pain in the head, in the projections of the sinuses. During rhinoscopy, 17 (28%) children had mucopurulent discharge from the nose in the middle and lower nasal passages, 43 (72.0%) had mucous discharge, 29 (48.0%) patients had hyperemia and swelling of the nasal mucosa . During pharyngoscopy, redness of the pharyngeal mucosa and mucus flowing down the back wall of the pharynx were observed in 48.1% of cases. In children, along with a runny nose, there were signs of acute pharyngitis and laryngotracheitis (24.0%), which was accompanied by a sore throat and dry cough; in 55% of cases the cough was paroxysmal in nature. In 40% of cases, complaints were made of chest pain when coughing. In 26.7% of children with symptoms of tracheitis, the cough was accompanied by the separation of viscous mucous sputum.
The presence of acute inflammatory process activity in 41.7% of children with acute respiratory diseases was evidenced by leukocytosis up to 11.08±1.4·109/l in 62.5% of them and an increase in ESR on average to 16.2±1.45 mm/h in 79.2%.
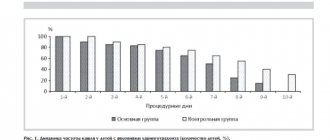
When using inhaled miramistin solution in children with symptoms of nasopharyngitis, the cough became milder, less frequent after the 2nd day of treatment, in 75% of patients it completely disappeared by the end of the course; sputum discharge improved, nasal congestion decreased, and the amount of discharge from the nasal passages decreased.
In 40% of children with symptoms of laryngotracheitis, cough complaints decreased significantly after the 4th day of inhalation. Against the background of a decrease in the number of coughing episodes in children in the main group, a change in the nature of sputum was recorded - the viscosity decreased, and the discharge acquired a mucous character. The cough became moist, more productive, its intensity decreased, which was accompanied by a significant decrease in sore throat and pain in the chest during coughing attacks. In 25% of children, the cough stopped completely after the 5th day of treatment, in half (45%) of the children - after the 7th day, in the remaining patients - after the 10th day of inhalation.
In the control group, the positive dynamics of clinical symptoms were less pronounced and occurred 3-4 days later ( Fig. 1
).
Under the influence of inhalation of Miramistin solution, favorable dynamics of the auscultatory picture were observed in the form of a decrease or disappearance of wheezing in the lungs after the 6th day of treatment in 65% of children with laryngotracheitis, in the remaining children - after the 8th day of inhalation. In the control group, the disappearance of wheezing was observed at a later date: in only 20% of children, wheezing disappeared by the end of the treatment course.
To assess the dynamics of subjective complaints, SAS was used. SAS data showed that by the end of the course of treatment, children of all groups had improved well-being and motor activity.
In children with symptoms of nasopharyngitis, nasal congestion, according to the SAS, decreased from 8.49±0.137 to 2.00±0 points, discharge from the nasal passages - from 9.25±0.155 to 2.00±0.10 points ( Fig. 2
).
In the control group, the dynamics of the severity of nasal congestion and nasal discharge decreased from 7.99±0.207 to 4.00±0.100 points and from 8.89±0.266 to 4.92±0.140 points, respectively ( Fig. 3
).
According to SAS data, after the first inhalation of miramistin solution in children with symptoms of laryngotracheitis, the intensity of cough decreased (from 9.30±0.179 to 7.70±0.193 points), weakness significantly decreased and performance increased. A significant decrease in subjective symptoms in children with symptoms of laryngotracheitis in the main group was noted after the 4th day of inhalation. In 2 children who received treatment for 10 days, by the end of treatment the severity of subjective symptoms decreased to 1 point ( Fig. 4
).
In the control group, the severity of subjective symptoms decreased gradually and by the end of the observation remained at an average level of 5.7 points.
Based on the studies conducted, a positive effect of inhalation of miramistin solution on peripheral blood parameters in children with acute respiratory infections who had initially reduced hemogram values was established, characterized by normalization of the leukocyte count and ESR in all children, which indicates an anti-inflammatory effect.
Analysis of the flow-volume curve data showed that at the beginning of the study, 70% of patients with complicated tracheitis had an average decrease in respiratory function below the age norm (POS - 69.24±0.23% D, FEV1 - 75.45± 0.67%D).
Under the influence of inhalation of miramistin solution, a tendency towards an increase in reduced indicators was noted (POS up to 73.02±0.34%D and FEV1 up to 82.36±0.41%D), but no significant dynamics were identified.
In children of the control group who received miramistin in the form of a spray, indicators of external respiration function remained at the same level.
During the study, daily monitoring of peak expiratory flow (PEF) was carried out in children with symptoms of tracheitis, which made it possible to monitor the state of external respiration and evaluate the effectiveness of the therapy. The initial PEF values in 25% of these children were below the age norm. In the course of the study, under the influence of inhalation of miramistin solution, a tendency was noted to increase the average PEF values after the 5th inhalation in almost half (45%) of children (from 66.79±0.76 to 74.22±0.62%D) , by the end of the course there was a significant increase in indicators to 78.35±0.89%D ( p
<0.05).
In children who received miramistin in the form of a spray, similar dynamics of PEF indicators were not recorded, which indicated a more pronounced positive effect of inhalations ( Fig. 5
).
Analysis of the initial level of physical fitness of school-age children with acute respiratory infections revealed a decrease in the degree of development of speed-strength capabilities in 70% of children, and a decrease in the level of development of strength capabilities in 80%.
Data from a repeated study of the functional state of the muscular system in all children after recovery indicated positive dynamics in speed-strength indicators of physical fitness (standing long jump, dynamometry).
A comprehensive assessment of the effectiveness showed a significantly higher therapeutic effectiveness of inhalation of Miramistin solution (87.5%) than when using Miramistin in the form of a spray (75.0%, p
<0.05), due to an increase in the pharmacotherapeutic activity of the drug due to an increase in the total volume of the drug suspension and the contact surface of the aerosol obtained using a nebulizer.
Miramistin - principle of action
Miramistin is a local antiseptic drug, the use of which allows you to disinfect mucous membranes and skin tissue. The drug has a wide spectrum of action, which allows it to be used in various areas of medicine, including for the treatment of runny nose in children of different ages.
The mechanism of action of the drug Miramistin is aimed at suppressing and destroying pathogens, which, after entering the body, provoke the development of inflammatory reactions. The active component of the drug, miramistin, after application to the nasal mucosa, interacts with lipids, penetrates the cell membranes of bacteria, destroys them from the inside, without causing harm to healthy tissues. Using Miramistin for a runny nose, you can not only stop the spread of infection in time, but also minimize complications and speed up the recovery period. The drug is highly effective in the treatment of runny nose, which is caused by staphylococci, streptococci, gram-positive, gram-negative and anaerobic bacteria. The medicine does not affect viruses or allergens, so it may be ineffective in treating a viral infection or allergic rhinitis.
The instructions for the drug indicate that Miramistin has the ability to act only on the superficial layers of the epithelium, is not absorbed into the blood plasma, and is non-toxic, therefore it can be used for children and pregnant women. Reviews from people who have used Miramistin for a runny nose are quite good, but as practice shows, the drug shows its high effectiveness in the first days of the disease.
We recommend reading: Miramistin for the nose during pregnancy.
Miramistin is available in the form of a solution, aerosol and ointment for external use. In the treatment of bacterial rhinitis, a solution or aerosol is most often used, which are convenient to use. Miramistin for a runny nose in children will not only suppress the aggressiveness of pathogenic bacteria, but also strengthen local protection, create a barrier for the penetration of microbes into the deeper layers of the epithelium of the nasal mucosa and the upper respiratory tract.
The instructions for the drug state that Miramistin is not prescribed to infants , but as practice shows, pediatricians often prescribe this drug for the youngest.
The solution, like Miramistin aerosol, can be used for the prevention or complex treatment of diseases of bacterial origin. For a runny nose, it is used in drop form, for washing the mucous membrane or for inhalation. The drug effectively fights various microbes and bacteria, stimulates local immunity, and accelerates the recovery period.
Inhalations with Miramistin for runny nose for children
Inhalation procedures with Miramistin are also very common in the treatment of bacterial rhinitis, but to carry out the procedure you will need an ultrasonic nebulizer. Miramistin - nebulizer inhalation for children with a runny nose should be used in its pure form. For one procedure you will need 1 - 2 ml of solution. The duration of inhalation is 5 – 10 minutes. The frequency of inhalation procedures is 2-3 times a day. It is important to remember that at temperatures above 37.2 degrees, inhalations are contraindicated.