Tonsil hyperplasia is a disease that is considered a childhood disease, in which pus collects in the folds of the mucous membrane of the tonsils, causing pathologies of the heart and/or kidneys.
- Causes of tonsil hyperplasia
- Symptoms
- Tonsil hyperplasia in children
- Diagnostics
- Treatment
- Prevention
- Forecast
Tonsils are a collection of lymphatic tissue that is designed to protect the body and has several locations. During certain processes in the body, the tonsils cease to perform the function of immunity and help the infection to spread. When lymphatic tissue increases in quantity, the tonsils become larger. Because of this, the child can no longer breathe normally. Hypoxia develops, and with a lack of oxygen in the body, as is known, the brain suffers greatly. In such cases, the child’s development is disrupted and he often falls ill.
Tonsils can grow due to swelling caused by inflammation. Provocateurs may be allergic agents or infection. The third reason is true hyperplasia. From 3 to 6 years, enlargement of the tonsils is a normal physiological process. Tonsil hyperplasia can be caused by pathogens such as mycoplasma and chlamydia. Correct prescription of medications is important for treatment. Anti-inflammatory drugs are relevant to relieve inflammation and minimize swelling. Antibacterial drugs are needed to destroy the pathogen that caused the disease.
If drug treatment is ineffective, the doctor prescribes a surgical operation called adenotomy. After this, you need to take immunostimulants for prevention. For the first degree of hyperplasia, surgery is not required.
Causes of tonsil hyperplasia
For the occurrence of the disease, a damaging factor, for example, a burn, is important. In such situations, not only the tonsils are affected, but also the tissues adjacent to them. Not only too hot water, but also alkaline and acidic substances can damage the tonsils. For treatment of such patients, hospitalization is mandatory.
Among the reasons are the impact of a third-party object. Most likely these are small fish bones that violate the integrity of the lymphatic tissue. When swallowing, a person in such cases feels as if something is stabbing in his throat. The next reason is tumors and abnormal development of the tonsils. An organ can also be damaged if:
- contact with infected mucus (adenoiditis)
- mouth breathing, resulting in prolonged inhalation of cold air
- diseases to which the child was exposed at a young age
- relapses and frequent diseases of the ears, throat and/or nose.
The following children are at risk for tonsil hyperplasia:
- malnourished
- with poor living conditions, without proper care from parents or guardians
- imbalance of hormones in the body
- lymphatic-hypoplastic constitutional anomaly plays a role
- exposure to radiation for a long time
- lack of vitamins
Activation of the production of lymphoid cells plays a role in pathogenesis.
external reference
- Photos at usc.edu (Registration required)
- Anatomical atlases - Microscopic anatomy, plate 09.163
- Histology Image: 09802loa - Boston University Histology Training System
- MedEd at Loyola (labeled "lymphoid tissue")]
- Lingual tonsil
Anatomy of the mouth | |
| Lip |
|
| Cheek |
|
| Sky |
|
| Gums |
|
| Glands |
|
| Teeth |
|
| Language |
|
| Back of the mouth |
|
Organs lymphatic system | |
| Primary organs | |
| Thymus |
|
| Tonsils |
|
| Lymph node |
|
| MALT |
|
- Anatomical portal
Symptoms
For effective treatment, parents must notice the pathology in time and come to the doctor with this problem. Timely diagnosis is a guarantee that there will be no complications. Doctors often record hypertrophic processes in several types of tonsils, including the pharyngeal tonsil. The doctor must palpate the tonsils; the consistency is soft or tightly elastic to the touch. The shade can be either light yellow or rich red.
The child may complain of difficulty inhaling and exhaling, as well as discomfort when swallowing. Breathing becomes noisy, the doctor records dysphagia (swallowing disorder) and dysphonia (voice disorder). Parents may characterize the little patient’s voice as nasal, his speech as unintelligible, and some of the words may not be pronounced entirely correctly by the patient.
As already noted, tonsil hyperplasia leads to hypoxia - the body does not receive enough oxygen. As a result, coughing and snoring may occur during sleep. If the pathological process involves the child’s ears, then the doctor notes otitis media.
Complications can be constant colds, because a child with hyperplasia cannot breathe normally and keeps his mouth open. Otitis media (the above-mentioned complication) causes persistent hearing loss.
Hyperplasia of the palatine tonsils
There is no inflammation, but lymph tissue growth is observed mainly in young children. Hyperplasia of the palatine tonsils in such cases acts as a compensation mechanism when the body is attacked by infections. When the tonsils become so large that they become an obstacle to the inhalation of air and its passage through the respiratory tract, surgery is performed to remove some of the tissue.
Pathogenesis involves an immunoreactive process. Breathing through the mouth is also important if the child has a problem such as adenoids. They contribute to the production of large amounts of infected mucus, which negatively affects the tonsils. Pathologies of the adrenal glands or thyroid gland play a role in pathogenesis. Apnea is likely to occur at night.
Hyperplasia of the lingual tonsil
This tonsil is located at the root of the tongue. From the age of fourteen, it develops back and therefore splits in two. When this process is disrupted, lymphatic tissue grows. With hyperplasia of the lingual tonsil, a teenager complains of a foreign body in the throat. This process can accompany the patient until he turns 40 years old. The cause is most often congenital. The patient's swallowing worsens, the timbre of his voice changes, and relatives may notice periods of time when the patient does not breathe at night, which is called apnea.
When a child is diagnosed with hyperplasia of the palatine tonsil, during physical exercise, breathing becomes bubbling and noisy. A symptom such as cough is likely to cause laryngospasm. Taking pills will not work; the cough will continue for years. In some cases, the cough can be prolonged and severe, leading to bleeding.
Hyperplasia of the nasopharyngeal tonsil
Researchers put forward the point of view that the nasopharyngeal tonsils play a role in immunity until the baby is 3 years old. Due to frequent childhood illnesses, pathological growth of lymph tissue may begin. The disease is typical for children living in cold or excessively damp rooms. Inflammation appears in the respiratory organs.
Tonsils can be of three degrees of growth. The first degree is characterized by the adenoids covering the top of the plate that forms the nasal septum. If this plate is closed by 65%, the doctor records degree II; closure by 90% or more indicates stage II of the pathology in question.
Symptoms: nasal congestion, significant “snot”, which is why nasal passage is very poor. Due to these factors, blood circulation in the nasal cavity is impaired, which aggravates inflammation in the nasopharynx. If the adenoids are of the second or third degree, then the voice is impaired and is characterized as deaf. The auditory tubes may be closed, in such cases, which is logical, hearing decreases to a greater or lesser extent. The child’s mouth may be slightly open, sometimes the lower jaw may sag, the nasolabial folds may smooth out, which changes facial features.
Hyperplasia of the pharyngeal tonsil
This amygdala develops before the age of 14, with a particularly rapid rate of development in infants. Hyperplasia of the pharyngeal tonsil is one of the manifestations of lymphatic diathesis. Hereditary factors, regular hypothermia of the body, lack of nutrients or calories in the diet, and attack by viral pathogens may also play a role.
In some cases, chronic inflammatory processes in the tonsils cause excessive growth of their tissue. It is difficult for the patient to breathe through his nose, so he opens his mouth to inhale and exhale air. The upper lip is higher than the normal level, swelling of the face and some elongation are observed. Therefore, the doctor may mistakenly suspect mental retardation.
The brain does not have enough air. In the morning the child looks as if he did not get enough sleep. During the day he can be unreasonably capricious. Dryness of the oral mucosa is typical, the voice is hoarse when the child tries to breathe through the mouth. Long-term rhinitis with sinusitis is also recorded; tubotympanitis and otitis are likely. The temperature may be slightly increased, appetite worsens, memory and attention also become worse.
Types of pathologies
Tonsils are the first barrier that traps pathogenic microorganisms. Therefore, inflammatory and infectious lesions of the tonsils are quite common, especially among children from 5 to 10 years old.
Angina
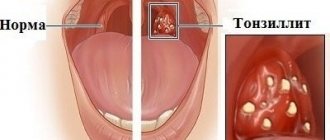
The term tonsillitis (acute tonsillitis) refers to acute inflammation of the palatine or pharyngeal tonsils. The main signs of the disease are dry, sore and sore throat, hyperemia and enlargement of the tonsils, increased temperature, and symptoms of intoxication.
There are several forms of angina, most often diagnosed:
- Catarrhal. The symptoms are mild and, with appropriate treatment, disappear within 3-5 days.
- Follicular. Follicles are affected. A characteristic symptom is pain when swallowing, radiating to the ear. The temperature can rise to 38 degrees or higher; upon examination, enlarged tonsils with whitish-yellow dots are visible.
- Lacunarnaya. The manifestations are similar to follicular, however, the symptoms of intoxication can be more pronounced. A yellowish-white coating covers most of the inflamed tonsils.
Treatment of sore throat involves the use of antibiotics, frequent gargling, and lowering the temperature if necessary. In the first days of acute inflammation, bed rest is necessary; compliance with it reduces the risk of complications.
Chronic tonsillitis
Most often it is a consequence of an untreated form of acute tonsillitis. It occurs with periods of relapses and remissions. A chronic focus of infection often becomes the cause of the development of dangerous diseases such as rheumatism, lupus erythematosus, and nephritis.
The treatment is complex. Antibiotics and drugs that enhance immunity are selected for the patient. If there is no effect from conservative therapy, partial or complete removal of the tonsils is recommended.
Hypertrophy
Tissue proliferation in most cases is characteristic of the nasopharyngeal tonsil. The disease is otherwise called adenoiditis and young children who often suffer from ARVI are susceptible to it. Primary signs are a frequently recurring runny nose, noisy breathing and snoring during sleep, a cough that gets worse at night, and mucous discharge from the nose.
Advanced forms of adenoiditis lead to chronic hypoxia, which causes lethargy and inattention. Lack of timely treatment can cause improper formation of the bones of the facial skull. Depending on the severity of hypertrophy, treatment can be medicinal or surgical.
Abscesses
They are characterized by the formation of cavities filled with pus near the tonsils. Most often, abscesses occur against the background of a sore throat. Symptoms are severe pain on the affected side, fever, high temperature, intoxication of the body. Abscesses are opened surgically.
Neoplasms
Cysts can form on the tonsils. A malignant lesion cannot be excluded, which at an early stage is manifested by tissue enlargement and periodic pain.
There are many reasons for the development of tonsil diseases. The main ones are infection with staphylococci, streptococci, and E. coli. Inflammation can be caused by hypothermia, mechanical injury, or chemical burn. The likelihood of pathologies increases with hypovitaminosis and low immunity. Pathogenic microorganisms can enter the tissues of the lymphatic ring not only directly, but also through the blood during chronic and acute diseases of other organs.
Tonsil hyperplasia in children
The child's body is often exposed to infections, such as whooping cough or scarlet fever. Hypertrophic processes are launched as compensatory ones. The diagnosis in question is made mainly to children under the age of ten years. Hyperplasia does not manifest itself as an inflammatory process. The tonsils are pale yellow in color, they are not red.
With the 1st degree of proliferation there are no symptoms. If growth is intense, then parents note a nasal voice of the child, breathing complications and other symptoms that were listed above. A large number of follicles, which are more fragile than normal, close the gaps without plugs.
Risk factors
- Viral infection (HPV16, HIV/AIDS, Epstein-Barr).
- Previous radiation or chemotherapy.
- Chromosomal aberrations.
- Tobacco smoking, consumption of low-quality alcoholic beverages.
Macroscopically, several forms of growth of formations are distinguished:
- Endophytic: flat or bulging (sometimes with ulcers).
- Exophytic: with or without ulcers.
The endophytic form of growth predominates and occurs in almost 80% of all cases where lymphoma of the tonsil or pharyngeal ring is detected.
In terms of prevalence, there are several stages of the process:
- 1 - the process is limited to the pharyngeal ring, the tumor diameter is up to 2 cm.
- 2 - differs from the first only in size, diameter - 2-4 cm.
- 3 - neoplasm spreads to the lymph nodes in the neck.
- 4 - the process spreads to adjacent organs and tissues (metastases to the larynx, Eustachian tubes, nasopharynx, skull bones, more distant organs).
Diagnostics
An experienced doctor pays attention to the facial expression of a small patient. It is important to interview parents, and, if possible, the child himself, to identify the main complaints. The history may indicate such points as low immune defense of the body, respiratory diseases (several per year), and a stuffy nose for a long time. Laboratory tests are important to determine the diagnosis. It is necessary to identify the pathogen and check its response to commonly used medications. The patient is prescribed bacterial culture from the throat.
The patient's blood must be taken for analysis, including acid-base balance, and urine must be taken for analysis to detect inflammation. Instrumental diagnostic methods are also relevant when diagnosing tonsil hyperplasia. Ultrasound diagnostics of the pharynx, pharyngoscopy, fibroendoscopy and rigid endoscopy are performed.
Tonsil hyperplasia can be caused (must be taken into account when diagnosing):
- cancer in the tonsils
- tuberculosis
- granulomas of the pharynx of an infectious nature
- leukemia
- lymphogranulomatosis
Treatment
Treatment requires a comprehensive approach, including the use of medications, physical therapy and, if necessary, surgery. In grade I (classification described above), special medications and rinses are prescribed. For the latter procedure, cauterizing and astringent agents are suitable, including a tannin solution; Antiseptics are also prescribed.
Hypertrophied areas are lubricated with a 2.5% solution of silver nitrate. The following medications are suitable for treatment:
- tonsilgon
- tonsilotren
- umkalor
- lymphomyosot
Topical physiotherapy techniques include:
- ultrasound
- ozone
- Microwave
- UHF
In some cases, endopharyngeal therapy with laser is needed. Mud ultraphonophoresis, electrophoresis, inhalation with decoctions of medicinal herbs, and vacuum hydrotherapy are often prescribed. In cases of II and III degrees of hyperplasia, surgical operations are resorted to. Most often, part of the overgrown tonsil is removed. This method is relevant for patients under seven years of age, if there is no polio, diphtheria, infectious diseases, or blood diseases.
Cryosurgery is a method of treating tonsil hyperplasia, in which the organ is affected by low temperatures, which allows you to get rid of pathological growths. In this case, the patient does not feel pain, and there is no blood either. This operation is indicated for patients with heart failure, atherosclerosis and heart defects.
The next method of treating the pathology in question is diathermocoagulation, in other words, cauterization. When agreeing to treatment with this method, consult your doctor about the high likelihood of various complications.
Prevention
It is important to live in favorable conditions, keeping the room clean, maintaining a normal level of air humidity and a temperature comfortable for the human body. Nutrition must be correct for the immune system to be active. In autumn and winter, you need to dress according to the weather, not breathe through your mouth, so that the tonsils are not exposed to icy air.
To maintain immunity, hardening, spa treatment, and additional courses of minerals and vitamins may be important. Respiratory and any other diseases must be treated on time so that they do not become chronic.
Structure
Microanatomy
The lingual tonsils are covered on the outside with stratified squamous non-keratinized epithelium, which invaginates inward, forming crypts. Under the epithelium there is a layer of lymphoid nodules containing lymphocytes. The mucous glands located at the root of the tongue drain through several ducts into the crypt of the lingual tonsils.[2][3] The secretions of these mucous glands keep the crypt clean and free of debris.
Blood supply
The lingual tonsils are located on the back surface of the tongue, through which they receive:[1]
- Lingual artery, branch of the external carotid artery
- Tonsillar branch of the facial artery
- Ascending and descending palatine arteries
- Ascending pharyngeal branch of the external carotid artery
Nervous nutrition
The lingual tonsils are innervated by the tonsils from the tonsil plexus, formed by the glossopharyngeal and vagus nerves.[1]
Forecast
Doctors almost always give a favorable prognosis. Thanks to tonsillotomy, a person can breathe through his nose, and his immunity returns to normal. The brain functions without hypoxia, which normalizes the patient’s sleep and general well-being. Nasal voice also disappears after proper treatment. At an early age, moderate hyperplasia of the tonsils can be detected, but after the child reaches ten years of age, it goes away. If after 10 years hyperplasia still exists, you need to consult a doctor.
If symptoms appear, consult a doctor for early diagnosis and treatment.