A patient with neuritis of the facial nerve can be recognized immediately: squinted eyes, mouth, crooked smile, changes in facial expressions are immediately noticeable. However, the worst thing is that the time for treatment of facial neuritis is quite limited. If damaged nerves are not restored within several months, the chances of recovery are sharply reduced.
After about a year or two, you can only slightly reduce the pathological manifestations, but not completely get rid of them. After 5–10 years, all therapeutic measures will be aimed at at least partially restoring the functioning of the nerve endings. What do you need to know about the symptoms and treatment of inflammation of the facial nerve so as not to miss the deadline?
Concept of facial nerve neuritis
The main cause of a crooked smile is neuritis (inflammation) of the facial nerve. This is paresis, characterized by partial damage to the facial nerve with loss of certain functions. In severe cases, when the pathways of the nerves in the face are completely affected, we can talk about paralysis. Thus, this pathology is partial or complete damage to motor pathways from neurons located in the cerebral cortex to the end of the branches of the facial nerves with disruption of their functioning:
- facial expressions (smiling, raising eyebrows, wrinkling the nose or forehead, baring teeth, etc.);
- speeches;
- smell functions;
- closing eyes or blinking.
Gum level.
A smile looks attractive and more aesthetically pleasing , in which the line connecting the necks of the teeth (shown in dotted lines) repeats the line of the upper lip, and the level of gum exposed when smiling is symmetrical on the right and left. At the same time, with a maximally open smile, only the gum “triangles” between the teeth and a small strip of gum above them (no more than 2-3 mm wide) should be noticeable.
Thus, the gums around the upper teeth, upper and lower lips form a kind of frame for your smile. If the “picture” is not visible behind the frame, then such a smile will not look attractive.
Excessive visualization of the gums (the so-called “gummy smile”) is most often eliminated with the help of surgery, orthodontic treatment, as well as cosmetic interventions (for example, Botox injections into the upper lip, upper lip augmentation, etc.).
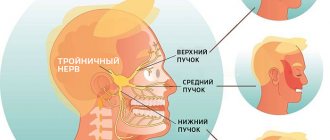
Facial nerve
The facial nerve is considered the main nerve of the human face. It comes to the surface in the area of the temporal bone and is divided into several branches:
- temporal;
- zygomatic;
- buccal;
- cervical and mandibular.
It performs mixed functions: provides secretion, movement, sensation (smell, taste). The facial nerve has a certain symmetry: thanks to it, both eyes close and open at the same time, both corners of the mouth are at the same height, when smiling they stretch symmetrically, when trying to raise the eyebrows they rise at the same height, and symmetrical folds form on the forehead.
Paresis or paralysis
When any part of the facial nerve is damaged, paresis or paralysis of a specific branch occurs - motor activity in this area is disrupted, and the patient cannot smile. His mouth begins to twist and his teeth on one side are not exposed when he smiles; one eye may not open. There may also be some disturbances in the functioning of the taste buds on the affected side. And salivation on this side, on the contrary, intensifies. This is how a crooked smile appears.
When the facial nerve is damaged, it usually becomes inflamed - when you palpate the affected cheek with your index finger and thumb, you will clearly feel the compaction of the branches of the nerves (you should palpate very carefully, as this causes pain to the person).
Vertical symmetry and midline.
A line passing through the center of the face should pass exactly between the central incisors of the upper jaw. The discrepancy between these lines causes a feeling of disharmony even with a quick glance at your smile from the outside. In this case, it is not at all necessary that it also passes between the central lower incisors. Firstly, a complete match is rarely found, and secondly, this in no way affects the aesthetic perception of your smile when viewed from the outside.
Distortion on the face
The most characteristic external manifestation of this condition is a drooping and motionless corner of the mouth, a skewed eye, and a cheek. Moderate or profuse drooling and lacrimation on the affected side may also be observed. Moreover, the patient does not feel these nerves - he seems to forget how to wrinkle his nose, smile or raise an eyebrow. The muscle fibers on one side are immobile due to impaired nerve patency. Deterioration or complete loss of taste may also occur.
Interincisal angles.
Interincisal angles are the spaces between the cutting edges of the anterior group of teeth.
With the harmonious construction of teeth, these angles should gradually increase from the center to the periphery: from a small closed angle between the central incisors, to a more direct and even open angle between the 2nd and 3rd teeth.
Tooth wear leads to a decrease or complete absence of interincisal angles, which makes the patient look older when he smiles.
At the same time, “female” teeth are characterized by rounded corners of the incisors, while “male” teeth are characterized by straighter ones.
Causes of pathology
Scientists have still not been able to establish a definitive cause of this disease. A number of factors have been associated with facial nerve inflammation:
- Hypothermia, which leads to a decrease in the body's immune defense. In the case of neuritis, local hypothermia is especially dangerous. For example, a person was in a draft for a long time. In this case, spasm of blood vessels and muscles occurs, which causes disruption of nerve nutrition and the development of a crooked smile.
- A herpes virus that lives in the body of most people and does not manifest itself in any way. However, in case of decreased immunity, it actively multiplies in its favorite place - in the structures of nerve fibers. The virus causes nerve swelling and inflammation. It is believed that this pathology can also be provoked by polio viruses, mumps, enterovirus and adenoviruses.
- Taking large amounts of alcohol. Ethyl alcohol is a strong poison for the nervous system. It can affect not only the brain, but also cause inflammation of the facial nerves.
- High blood pressure. Hypertension can lead to increased intracranial pressure. In this case, the nuclei of the facial nerve are damaged. In addition, high blood pressure often causes stroke. And if the hemorrhage occurs near the facial nerve, then it also suffers.
- Pregnancy. The first trimester is especially dangerous. During this period, hormonal changes occur in the female body, which affect the nervous system.
- Brain tumor. This is a rare cause of neuritis, however, it should not be excluded. The tumor grows, pinches the nerve and disrupts the passage of nerve impulses.
- Traumatic brain or ear injuries. The blow causes damage or rupture of the nerve fiber. Fluid begins to accumulate in this area, swelling and inflammation occurs, which subsequently spreads to the entire nerve.
- Unsuccessful dental procedures, carious infection.
- Severe stress.
- Previous sinusitis and otitis. Pathologies of the ENT organs, bacterial or viral in nature, can spread to neighboring tissues or cause inflammation of the nerve in the area of the temporal bone.
- Diabetes. With this disease, metabolic disorders develop, which provokes the development of foci of inflammation.
- Atherosclerosis. The capillary vessels that supply the nerve with blood become clogged with plaque. As a result, the nerve begins to starve and its cells die.
- Multiple sclerosis. This disease is associated with the destruction of the myelin sheath of nerves and the formation of plaques. Such processes cause inflammation of the facial and optic nerves.
Seven main violations when creating a smile design
Students and practitioners are increasingly turning to digital smile design techniques to directly demonstrate potential aesthetic changes to patients and healthcare team members (including dental technicians). The principles of smile design include studies of facial aesthetics, labiodental dynamics, gum and dentition architecture, as well as the phonetic component. To better explain to patients and demonstrate to their colleagues the dynamics of aesthetic changes in the smile, many doctors do a fantastic job of illustrating the principles of smile design in relation to the ideal state of harmony required, based on the individual anatomical features and physiological characteristics of each individual patient.
This approach is useful not only from a demonstration point of view, but also in terms of identifying possible violations that compromise the aesthetic appearance. Therefore, recommendations regarding the proper assessment and resolution of specific errors encountered during the smile design stage provide some guidance in the practice of aesthetic dentistry.
This article discusses seven main violations in the formation of design, as well as methods for assessing them and solving them to restore the ideal harmonious form.
1. Crooked smile
A crooked smile is an extremely noticeable violation not only for a dentist, but also for an ordinary person, like a crooked shelf on a flat wall. After restoration, few people additionally check the condition of the interincisal line, but it is this line that affects the visual inclination of the smile line relative to the vertical axis (photo 1 and photo 2). Straightening your smile requires developing a preliminary treatment plan that takes into account basic aesthetic principles. Among the aspects that definitely need to be examined: horizontal and vertical parameters of the face, including the line connecting the corners of the mouth, as well as the interpupillary horizontal line. A vertical line drawn through the middle of the face should be assessed in relation to the bridge of the nose, the tip of the nose and the middle of the chin. It is also important to ensure that the interincisal contact line is perpendicular to the absolute horizontal. To prevent a crooked smile, it is important to understand that the analysis of facial aesthetics should begin with studying the patient’s photograph, and in no case should it be reduced to the analysis of models (which is an extremely popular violation, taking into account the fact that even models in the majority are analyzed only on the subject of interest area of the jaw). When studying the planes of the face, it is necessary to take into account the patient’s characteristic horizontal position of the head, since it is largely the starting point for the further formation of the smile design. As a rule, this criterion in most cases coincides with the absolute horizontal plane, relative to which some facial features may have disturbances (as a consequence of the asymmetry effect). It is also important to analyze the facial area as a whole, and not concentrate on the position of only the area of interest relative to the horizontal plane. Restoring the horizontal plane is also an important aspect of collaboration with the dental technician using a facebow and wax-up (Photo 3 and Photo 4).
Photo 1. A comprehensive facial analysis before intervention is the key to treatment success. Changes in the interincisal angle, which may not be noticeable, can be detected through graphical analysis of photographs, which also facilitates collaboration with the laboratory when correcting a crooked smile (restorations made by IPS e.max and IPS Empress (Ivoclar Vivadent)
Photo 2. A comprehensive facial analysis before intervention is the key to treatment success. Changes in the interincisal angle, which may not be noticeable, can be detected through graphical analysis of photographs, which also facilitates collaboration with the laboratory when correcting a crooked smile (restorations made by IPS e.max and IPS Empress (Ivoclar Vivadent)
Photo 3. The use of a facebow and mock-up helps the dentist coordinate the dental technician regarding the required position of the incisal edges and interincisal line, which makes the final treatment results more predictable.
Photo 4. The use of a facebow and mock-up helps the dentist coordinate the dental technician regarding the required position of the incisal edges and interincisal line, which makes the final treatment results more predictable.
2. Reverse smile
Formation of a smile requires maintaining symmetry between the cutting edge of the anterior teeth of the upper jaw and the border of the lower lip following it (the principle of labiodental dynamics). Labiodental dynamics are formed from the cutting edge, where a convex line is created that extends into the area of the chewing teeth. The chewing teeth, as a rule, follow the level of the occlusal plane parallel to the Camper horizontal (from the nose to the tragus of the ear). The level of convexity depends on the patient’s gender, age, shape of the lower lip and individual characteristics. Straight smile lines are more common in men and older people, while more convex curves are more common in younger people and women. A reverse smile in the shape of a concave curve provokes an unaesthetic appearance of the cutting line, while creating the facial image of an “unhappy” person (photo 5). In order to ensure a “happy” smile, it is necessary to analyze in detail the length of the teeth and their relationship with the lips in a dynamic state. This approach will help you understand what is best to do: shorten the canines or lengthen the incisors to correct a concave smile. Although in the literature there are also recommendations that it is necessary to check the position of the fangs relative to the edge of the lips, since the type of incisors depends on too many factors: the shape and length of the lips, the length of the tooth and even the characteristics of lip movements. The results of recording the final position of the incisal edge are transferred to the laboratory before the stage of making the wax reproduction, because in this case it is possible to correct the length of the teeth and the convex shape of the smile, both using mock-up and using digital software (photo 6-8). The positions of the smile shape can be partially recorded using a face bow and models correctly plastered in the articulator, but to determine labiodental dynamics it is necessary to analyze photographs and videos of the patient.
Photo 5. With a reverse or concave smile, the line of the incisal edge of the teeth is not congruent with the border of the lower lip. Correcting the incisal line to a more convex shape ensures that the smile is symmetrical relative to the lower lip and creates a more aesthetic profile.
Photo 6. Before starting treatment, it is important to establish the final position of the incisal edge, taking into account the shape of the gingival margin and the ratio of the length and height of the crowns. Excessive elongation of teeth can cause the effect of narrow central incisors. The use of digital methods (for example, proportional shapes with specific width-to-height ratios) during the pre-planning stages will determine the required length of incisal edges, taking into account changes in the gingival margin. The final length of the incisors can also be double-checked on a mock-up before changing the gingival contour. The use of wax reproductions significantly reduces the time required to make provisional structures. The concave shape of the smile was restored to a more convex contour with IPS Empress restorations.
Photo 7. Before starting treatment, it is important to establish the final position of the incisal edge, taking into account the shape of the gingival margin and the ratio of the length and height of the crowns. Excessive elongation of teeth can cause the effect of narrow central incisors. The use of digital methods (for example, proportional shapes with specific width-to-height ratios) during the pre-planning stages will determine the required length of incisal edges, taking into account changes in the gingival margin. The final length of the incisors can also be double-checked on a mock-up before changing the gingival contour. The use of wax reproductions significantly reduces the time required to make provisional structures. The concave shape of the smile was restored to a more convex contour with IPS Empress restorations.
Photo 8. Before starting treatment, it is important to establish the final position of the incisal edge, taking into account the shape of the gingival margin and the ratio of the length and height of the crowns. Excessive elongation of teeth can cause the effect of narrow central incisors. The use of digital methods (for example, proportional shapes with specific width-to-height ratios) during the pre-planning stages will determine the required length of incisal edges, taking into account changes in the gingival margin. The final length of the incisors can also be double-checked on a mock-up before changing the gingival contour. The use of wax reproductions significantly reduces the time required to make provisional structures. The concave shape of the smile was restored to a more convex contour with IPS Empress restorations.
3. Social Six
Aesthetic violations of the front teeth (their color and shape) are much more difficult to correct than similar violations in the posterior area, since it is the front teeth that recreate the main appearance of the smile. Although the study of dentolabial width points to the fact that in most cases, 10 to 12 maxillary teeth are exposed when smiling, so smile correction needs to be carried out wider than the range of the social six (photo 9-11). To do this, before starting treatment, you need to study in detail photographs of the patient’s smile from the frontal and lateral views. Another principle of dentolabial dynamics (also known as buccal corridor or buccal width) is that the size of the space between the back teeth and cheek can vary from patient to patient, so this aspect is also equally important when contouring a smile. If the buccal corridor is quite narrow, then treating only the social six teeth further provokes a narrow appearance of the smile. In addition, such an approach to rehabilitation provokes the effect of highlighting the frontal teeth and their contrast in comparison with the chewing group. Conversely, restoration of the posterior teeth with some lightening can simulate a wider volume of cheek space, and thereby recreate a completely new and fuller smile contour. The right solution is to find a balance between these parameters. Again, before treatment, you need to analyze the nature of the smile, evaluate the color and contour of the existing back teeth. In addition, the relationship between the occlusal plane in the posterior region and the plane of the incisal edge must be taken into account. It is always necessary to take into account those treatment options in which it is possible not only to restore the smile with the help of individual restorations in the frontal group of teeth, but to adjust its contour in relation to the chewing teeth, while giving it a full appearance and aesthetic harmony.
Photo 9-11. Patients with excessive buccal space can improve the overall appearance of their smile due to problems with the anterior teeth only. On the contrary, a deficiency of the buccal corridor can compromise the treatment result through the effect of an artificial smile. Widening the smile from the anterior IPS e.max restorations to the directly restored premolars allows you to create the ideal oral width parameter.
4. Ignoring the proportions of the central incisor
The central incisors naturally dominate the smile, so incisor symmetry is of utmost importance to achieve optimal aesthetic contour. In addition, the proportion of each individual incisor also plays an equally important role. The Golden Ratio has traditionally been the reference principle for creating the perfect smile, but today artistic design is leaning towards less regimented approaches and individualized designs. The width-to-height ratio of unworn incisors is usually 80%. This proportion must be adhered to in order to avoid too long, narrow, or, on the contrary, too wide and excessively voluminous appearance of the front teeth. When correcting aesthetic length or width, or when deliberately altering incisors due to crowding, the most common effect is that the tooth is too long or too narrow compared to its actual width. With the loss of the central dominant, the sizes of the central and lateral incisors may appear similar, which creates an unaesthetic and artificial appearance of the smile. If the space for restoration of the central dominant is limited, you can slightly narrow the shape of the lateral incisors, or even rotate them slightly around their axis (photo 12 and photo 13). An effective principle is to support 65% of the width of the central incisors in the area of the lateral teeth, and, accordingly, 75% of the transverse width of the laterals in the area of the canines. The use of graphical proportion limiters in Keynote or PowerPoint and their positioning on top of the teeth image, or measuring the actual width and height of the crown in patients and calculating the ratios greatly facilitates the effect of visualizing a smile and promotes cooperation with the laboratory at the treatment planning stages.
Photo 12-13. Patients with excessive buccal space can improve the overall appearance of their smile due to problems with the anterior teeth only. On the contrary, a deficiency of the buccal corridor can compromise the treatment result through the effect of an artificial smile. Widening the smile from the anterior IPS e.max restorations to the directly restored premolars allows you to create the ideal oral width parameter.
5. Overly contoured teeth
There are three main tooth shapes: narrow, square and oval. All teeth also have reflective and refractive zones, separated by right angles. By manipulating these angles, it is possible to imitate a short and voluminous shape, a long and narrow appearance, or a more rectangular or curved tooth outline. The mesio- and distal-facial right angles are located on the facial surface closer to the contact area. Moving them outward from the contact pads creates a wider tooth appearance, while moving them toward the center imitates a narrower tooth shape. Without distinguishing between the reflective and refractive zones, teeth may appear overly contoured (Figure 14 and Figure 15). Since ceramists work in conditions created by the preparation stage, in which transition angles are reduced, they need to restore specific areas of the tooth using the ceramic itself as a veneering material. When preparing for veneers, you must carefully ensure that the tissue is adequately reduced relative to the contour of the final restorations at the mock-up stage. The depth of preparation should be appropriate mesio- and distofacially in all three planes to provide sufficient space to create esthetic reflective and refractive zones in these areas without thickening the shape of the entire tooth.
Photo 14-15. Teeth lacking visualization of final right angles appear overly contoured as the contour height parameter migrates in the facial direction. This problem is related to the design of the preparation. Preparation with mock-up allows you to achieve the ideal design. The use of wax reproduction helps to predict the result and make the necessary corrections before the fixation stage. The existing ceramic restorations on teeth 4-13 were replaced with IPS e.max restorations; teeth 20-29 were also restored.
6. Ignoring negative space
The space around a tooth determines its visual boundaries and the overall composition of the smile. When designing a smile, it is important to provide sufficient space for embrasures in the incisal area and interincisal angles in the incisal area. The width of the tooth and visual depth are determined by the area of the interdental contact areas, which for central incisors expand to the cutting edge and reduce the cutting angle. Tooth contact points migrate apically from the central incisors to the canines, thereby increasing the interincisal angles. As teeth wear down, the incisal angles decrease or disappear completely, creating a flat smile line and an aging effect. When restoring a smile, clinicians must recreate the natural progression of the interincisal angle, which in turn determines the morphology, appropriate tooth length, and convexity of the incisal curve. Incisal angles are also taken into account when preparing for construction to ensure that ceramists have enough room to restore negative space. These areas can be corrected after cementation using the proper tools (photos 16-19).
Photo 16-19. Loss of space between the incisors creates the appearance of an older smile. View before intervention: 38-year-old patient with signs of pathological abrasion due to bruxism. At the planning stage, a mock-up was made and proportions were determined to restore the ideal shape of the teeth. After installing IPS e.max restorations, the interdental spaces were restored, which made the appearance even more masculine; the parameters of durability, function and aesthetics were also optimized.
7. Gum asymmetry
The position of the gums is another important factor in determining smile design. The aesthetics of the gums influences the parameters of symmetry (identity of parameters relative to the vertical axis) and harmony (the criterion of repetition of relationship parameters), and is one of the key criteria at the treatment planning stage. However, restoring tooth length to recreate symmetry can disrupt the harmony of the smile, especially if the height and position of the gum margin were not taken into account when planning treatment. The position of the gum margin is especially important in people with medium to high smile lines. The smile line is also one of the parameters of labiodental dynamics, which determines the position of the lips during a smile (for example, 69% of people expose from 75% to 100% of the height of the central incisors along with the area of the interdental papilla when smiling). The gingival margins of the canines and central incisors should be symmetrical and positioned more apically than those of the lateral incisors. The gingival margin should gradually migrate towards the incisal area in the direction from the central to the lateral teeth. The rule is that the gum edge of the canines and central incisors should be in line, and the gums around the lateral teeth should be slightly closer to the incisal area, that is, the gingival edge line of the lateral incisors should be below a similar line connecting the gum edge of the central incisors and fangs (photo 20). Since the position of the gingival margin is determined by photographs and models correctly positioned relative to the horizontal line, there is a need for high-quality preoperative images. The optimal diagnostic analysis will help you choose the right treatment approach: whether to contour the gum area or get by with crown lengthening. Loss of soft tissue levels is most often observed in cases of poor surgical planning, so the use of surgical guides helps to more accurately control such changes. Assessing a smile together with the patient helps the doctor motivate the latter to perform specific procedures aimed at leveling factors that compromise the external aesthetic appearance. In addition, cooperation with the patient helps the doctor understand and satisfy specific individual wishes and achieve exactly the results that the patient, in principle, expects.
Figure 20: Gingival esthetics also play a key role in smile design, and understanding the ideal soft tissue parameters makes it easier to plan appropriate treatment, highlighting important points that need to be discussed with the patient prior to intervention. For ideal symmetry, it is important that the lateral incisors are more gingival to the line connecting the gingival margin of the central incisors and canines.
conclusions
Proper examination and treatment of patients with smile disorders helps to recreate the desired aesthetic appearance of the patient and achieve the maximum possible positive rehabilitation results. Continuous education in the basic principles of smile design will help you identify and understand the basic criteria that must be adhered to during treatment, and a discussion of the seven most common design mistakes will help you anticipate and avoid subsequent complications and disappointments in the final outcome of your rehabilitation.
Posted by Jason Olitsky, DMD, AAACD
Diagnostics
Establishing a diagnosis is quite simple - the patient has it “written all over his face.” The main external sign is an asymmetrical smile. However, for adequate therapy it is important to determine the location and extent of the lesion. Based on external signs, one can only guess which branches are affected, but this is not enough for a complete clinical picture.
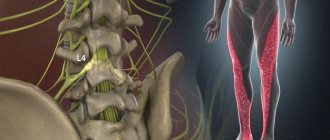
For diagnosis, electroneuromyography is used, which allows one to evaluate the conductivity of nerve endings, track the signal path and find the affected area.
An MRI may also be ordered. The photographs show the affected nerves and surrounding tissues.
Interdental gingival papillae.
The gingival papilla is the part of the gum that fills the interdental space (marked with lines in the photo).
The location and appearance of the papillae is determined by the underlying bone, which has exactly the same contour. In the most optimal option, the tops of the gingival papillae are located as in the photo (marked with dots) - between the central incisors the gingival papilla is longest, and gradually its length decreases towards the periphery. Moreover, they should all have a healthy appearance - a triangular shape with a sharp apex, pink color, no swelling.
With various periodontal diseases, as well as with improperly performed restorations, the gingival papilla may become inflamed, acquiring a darker (or even bluish) color, losing its pointed shape, or may even disappear completely. At the same time, unaesthetic black spaces form between the teeth.
This is what the main, but still far from complete, list of parameters that need to be assessed and taken into account when planning and creating an ideal smile looks like. aesthetic dentistry does . Now you can evaluate for yourself how close your smile is to ideal. And I hope that this note will help you better understand what exactly you would like to change and improve. After all, this will greatly facilitate mutual understanding between you and your dentist.
PS See the photographs of clinical cases of my patients presented in this note in detail in the photo gallery section of the site, where details about aesthetic dentistry and modern dental technologies for restoring an ideal smile.
Treatment
People often ask: “What pills should I take if I have a crooked smile?” Let's figure it out.
Facial neuritis should be treated no later than 3 to 7 days from the onset of the first symptoms. This is because the disease progresses rapidly as nerve cells begin to die.
It is important to find out in advance how to correct a crooked smile.
For neuritis of the facial nerve, medications containing B vitamins are prescribed. This is a neurotropic combination that improves metabolic processes, trophism of nerve pathways, and impulse transmission. Lipoic acid (thioctacid) and the medicine Keltican are also prescribed.
To restore movement functions, the patient is prescribed a massage of the face and collar area, physical therapy, which is aimed at restoring blood supply to the affected nerves.
Position of cutting edges.
The cutting edges of the central group of teeth are also located at different levels. For the central incisors and canines - approximately at the same level, for the lateral incisors - slightly higher (as marked by lines in the photo).
Again, due to the abrasion of teeth with age, the cutting edges of the teeth become at the same level, the line connecting them takes on a straight rather than convex appearance, and sometimes (with increased pathological abrasion) even concave. Therefore, to make a smile more “youthful,” you need to return the relationship of the cutting edges to a harmonious one.
It can also be noted that the dominance of the central incisors over the lateral incisors and canines also gives the smile a more youthful appearance.
The dominance of the canines, their sharp, prominent cutting cusps, make the smile more aggressive. This effect is based on the fact that in nature, long, sharp, well-developed fangs are characteristic of predators, whose entire philosophy of existence is based on aggression towards their prey.
Exercises
What exercises can be performed for inflammation of the facial nerve? How to correct a crooked smile with exercises?
It is necessary to force the nerve fibers to begin functioning again. To practice, you need to use a mirror, in front of which you do gymnastics: raising and lowering your eyebrows, blowing air through pursed lips, pronouncing sounds, syllables and words, trying not to twist your lips to one side.
We looked at the symptoms and treatment of inflammation of the facial nerve. For therapy to be effective, it is necessary to approach the process comprehensively. A variety of physiotherapeutic procedures that are aimed at eliminating the inflammatory process in nerve fibers and restoring their conductivity have a good effect.
Proportions of the tooth.
The central incisors of the upper jaw always attract special attention, because... best visible when talking and smiling. Therefore, it is very important that their proportions are correct. The most harmonious looking teeth are those with a ratio of tooth width to length of approximately 0.7-0.8: 1
However, at different ages this ratio may change. Due to the physiological wear of teeth in older age, this ratio tends to be 1:1. Therefore, if you want to “rejuvenate” your smile, you usually need to increase the length of the tooth.