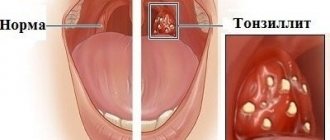
Tonsillitis is an infectious disease in which inflammation of the tonsils (glands) occurs. This disease affects both adults and children aged 2 years and older. Tonsillitis in a child most often occurs between the ages of five and ten years, and inflammation can recur several times a year.
The acute form of the disease is nothing more than the well-known sore throat. A person who has suffered from a sore throat at least once, during which he experienced severe pain in the throat, will not confuse it with any other diagnosis. Sore throat is an insidious disease that can cause serious complications in related organs and even lead to disability. What effective measures should be taken in the treatment of inflammation of the tonsils to avoid complications? We will talk about this in detail in our article.
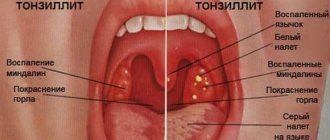
Symptoms:
- red, swollen tonsils with white or yellowish coating or streaks;
- a sore throat;
- difficult and/or painful to swallow;
- fever (temperature above 38.0);
- cervical lymph nodes are enlarged;
- hoarse or hoarse voice;
- headache;
- stiff neck muscles;
- abdominal pain (especially in young children).
In infants:
- drooling due to pain in swallowing;
- anxiety;
- refusal to eat
- With chronic tonsillitis, your breath may smell bad.
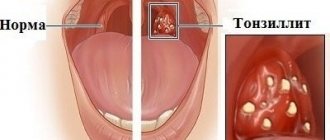
Tonsils on guard
The tonsils (or tonsils) are located on both sides of the throat. All bacteria and viruses that enter the body through the mouth are encountered first. Externally, the tonsils have a porous structure; this structure helps them “examine” all the substances that enter the body and decide what to do with them. In the thickness of the palatine tonsils there are special depressions - lacunae, and the convoluted channels in the thickness of the tonsils are called crypts; they are difficult to see in a photo or with the naked eye. There are also target cells that act as “traps” for microorganisms. When it comes into contact with them, the tonsil decides whether to fight them or not, whether they will cause harm to a person or whether they will be harmless.
When a person is healthy and his tonsils are strong, when any infection enters the body, they begin to actively produce white blood cells to fight the infectious pathogen. But when inflammation affects the tonsils themselves, they lose their protective function and themselves become a source of infection. Pathogenic viruses and bacteria settle firmly in the gaps. What function can inflamed tonsils perform? None! As a result, the tonsils fall out of the body's general defense system and there is a high chance of developing chronic tonsillitis in children.
Complications of tonsillitis
- Labored breathing.
- Sleep apnea (holding your breath during sleep).
- Spread of infection to the tissue near the tonsils (peritonsillitis), peritonsillar abscess - accumulation of pus behind the tonsil.
- Acute cervical lymphadenitis is inflammation of the cervical lymph nodes.
Streptococcal tonsillitis can cause complications such as:
- acute rheumatic fever, affecting the joints, heart and other organs;
- glomerulonephritis (inflammation of the kidneys, which can lead to serious consequences, including kidney failure).
Treatment with antibiotics significantly reduces the likelihood of complications after streptococcal sore throat.
Prevention and treatment of tonsillitis in children
What are the difficulties in treating chronic tonsillitis? What procedures are included in the complex of preventive treatment?
In the structure of diseases of the ENT organs in children, a significant part is made up of infectious and inflammatory diseases of the palatine tonsils, which account for 20% of cases in the general population and up to 43% in the group of frequently ill children.
In the etiology of acute tonsillitis (angina), the main role is played by the following microorganisms: Hemophilus influenzae, Moraxella catharralis and beta-hemolytic streptococcus, the relevance of which in the development of the pathological process is still high.
Other microorganisms, such as viruses, streptococci of other groups, Neisseria, etc., are of significantly less importance.
Infection occurs by airborne droplets, the source is a sick person or, more importantly for children attending preschool institutions and schools, an asymptomatic carrier.
The clinical picture of acute tonsillitis, as a rule, is quite typical and does not cause diagnostic difficulties: there is an acute onset with a rise in body temperature from low-grade fever to severe hyperthermia, general weakness, headache, sore throat, aggravated by swallowing, enlargement and tenderness of the tonsillar lymph nodes.
During pharyngoscopy, the picture is also typical: hyperemic and edematous tonsils, soft palate, posterior wall of the pharynx, as well as lateral columns (in Western countries the diagnosis of tonsillopharyngitis is accepted; in the lacunae of the tonsils there are inflamed purulent follicles or widespread white-yellow overlays on the tonsils (but not extending beyond the tonsils, that is, not spreading to the arches and soft palate).The plaques are loose, easily removed from the surface of the tonsils. After removing the film, the tonsil does not bleed.
Diagnosis of catarrhal tonsillitis may present some difficulties when there is no plaque on the tonsils. But this is a somewhat special case: there is currently a discussion about the legitimacy of such a diagnosis, that is, the existence of catarrhal tonsillitis as such is being questioned. In these cases, it is proposed to make a diagnosis of acute respiratory disease.
A clinical blood test determines changes typical of the inflammatory process.
Ideally, before starting therapy, a microbiological examination of a smear from the tonsils is carried out to determine sensitivity to antibiotics.
Therapy for acute tonsillitis remains traditional: it is antibacterial therapy, and aminopenicillins with clavulanic acid (amoxiclav, augmentin) remain the drugs of choice. Synthetic penicillins retain their value only in the treatment of acute tonsillitis caused by beta-hemolytic streptococcus. Today, from the group of penicillins for oral administration, amoxicillin is the most important, surpassing other drugs in this group in its pharmacokinetic properties. Along with penicillins, cephalosporin antibiotics are used, with preference given to drugs of the first (cefadroxil) and second (cefuroxime, axetil, cefaclor) generations.
In case of intolerance to penicillins and cephalosporins, macrolides are used.
Along with systemic antibiotics, topical antiseptics are also used that have an anti-inflammatory and analgesic effect (hexasprey, hexoral, stopangin, tantum verde, etc.).
Irrational treatment of acute tonsillitis, in particular refusal of systemic antibiotic therapy or its unjustifiably shortened course, is one of the reasons for the chronicity of the process.
Treatment of chronic tonsillitis, both in the acute stage and in the remission stage, is associated with a number of difficulties. In particular, it is necessary to take into account that in a chronic process, as a rule, not an isolated flora is detected, but a mixed infection, which is much less amenable to antibacterial therapy. The most obvious way to treat chronic tonsillitis is surgery - bilateral tonsillectomy. In adult patients, this route is justified in any case. But as to whether tonsils should be removed in children, and if so, at what age, expert opinions differ. This is due to the fact that the lymphopharyngeal ring performs protective functions and is an immunocompetent organ. Therefore, a significant number of pediatricians believe that if chronic tonsillitis occurs in a compensated form, it is necessary to carry out conservative treatment.
The standard complex of preventive conservative treatment of chronic tonsillitis includes a set of procedures aimed at combating pathogenic microflora that is constantly located in the lacunae of the tonsils, improving the drainage of the tonsils, and correcting the body’s immunological defense. This complex includes washing the lacunae of the tonsils, lubricating the tonsils with antiseptic solutions, physiotherapeutic procedures (ultrasound in the submandibular area or laser therapy), and the use of immunomodulators. The course of treatment is carried out twice a year.
Our study was conducted to identify the most optimal scheme for the preventive treatment of chronic tonsillitis.
From April 2000 to June 2002, 68 children aged 7 to 12 years with a diagnosis of chronic tonsillitis, compensated form, were under our supervision. (Children under 7 years of age were excluded from the study, since contact with them was difficult and, therefore, there were limitations in carrying out the full course of complex therapy.) In 24 (35%) children, the disease occurred with exacerbations in the form of sore throats 1 time per year or 2 every three years, 6 of them had a history of peritonsillar abscesses. All parents categorically refused surgical intervention. The remaining 44 (65%) people had a compensated non-anginal form of chronic tonsillitis. (There was no documented diagnosis of tonsillitis in the medical history.)
All children complained of increased fatigue and periodic headaches. Parents paid attention to weakness, sweating, frequent colds, and a prolonged “unmotivated” increase in body temperature to subfebrile levels.
During examination, all children showed enlargement and hardening of the submandibular lymph nodes. Soreness was noted by 11 (16%) children included in the examination 7-10 days after suffering from tonsillitis.
All children had slight hyperemia of the mucous membrane of the tonsils and the posterior pharyngeal wall. The anterior arches were significantly hyperemic and injected with vessels. The tonsils are fused to the arches, with widened lacunae; there is pathological purulent discharge in the lacunae. 49 (72%) people had grade II tonsils and 19 (23%) people had grade III tonsils. 10 children had a purulent odor from their mouth.
All children under our supervision underwent a course of conservative treatment of chronic tonsillitis 2 times a year. Every other day, they washed the lacunae of the tonsils (from 8 to 10 procedures, depending on the effectiveness). In all cases, these procedures were combined with ultrasound examination of the submandibular area.
Washings were carried out with solutions of Hexoral (10 patients), Miramistin (20 patients), Octinosept (28 patients). These drugs were chosen due to the fact that they have a wide spectrum of antimicrobial and antifungal effects, are non-toxic, are not absorbed through intact mucous membranes, have a taste acceptable to children, and are available in the form of solutions.
After the treatment, a visual effect was noted after the 5th procedure: the tonsils shrank in size, acquired a pale pink color, the lacunae remained free, and the bad breath disappeared.
In addition to the direct impact on the tonsils with antiseptic solutions and the use of physiotherapy, we included in the complex of preventive procedures homeopathic remedies that have an anti-inflammatory effect, aimed at strengthening the lymphoid tissue. In particular, tonsilotren was used, a complex drug whose action is aimed at eliminating the symptoms of inflammation, reducing hypertrophy of the palatine and nasopharyngeal tonsils, as well as regional lymph nodes by improving the drainage of lymphoid tissue and the immunomodulatory effect.
The drug was prescribed as a tablet 3 times a day (at the same time a course of lavage of the tonsil lacunae and physiotherapy began) and was taken for a long time, for 6 weeks. The drug was well tolerated. In 4 (6%) children, tonsilotren had to be discontinued on the 4th day of treatment at the request of their parents due to a slight exacerbation of tonsillitis symptoms.
Control was carried out 3 months after the start of complex therapy. After the first course of preventive treatment, out of 64 children taking tonsilotren, 53 (83%) people did not have any complaints related to diseases of the ENT organs for 3 months. The pharyngoscopy picture remained satisfactory. 9 (14%) people suffered mild ARVI, 2 (3%) patients had ARVI with high fever and sore throat.
After 6 months (from the start of the first course), 64 people underwent preventive treatment again in full, excluding 4 children who did not take the homeopathic drug. During a follow-up examination carried out 6 months later (before the next course of preventive treatment), a satisfactory pharyngoscopy picture was noted, no pathological changes were observed in clinical blood and urine tests, and the ECG was within the age norm. During the reporting period, 59 (92%) people had virtually no complaints. 2 (3%) children suffered from ARVI, 1 child had bronchitis, 2 (3%) people suffered from follicular tonsillitis. In 1 child, tonsillitis was complicated by a peritonsillar abscess. The parents refused the operation.
During the observation period, the children received 5 courses of preventive treatment for chronic tonsillitis. During this time, the number of children suffering from acute respiratory viral infections and other respiratory infections sharply decreased. In 62 (97%) people, sore throats did not recur. The pharyngoscopy picture remained satisfactory.
In 2 children, bilateral tonsillectomy was performed due to the ineffectiveness of conservative treatment.
Thus, complex preventive treatment of chronic tonsillitis with the inclusion of antiseptic solutions and homeopathic drugs (tonsilotren) in the therapeutic regimen is highly effective and allows children to preserve the tonsils as a necessary immunocompetent organ and avoid traumatic surgery.
Literature
- Belov B.S. A-streptococcal tonsillitis: clinical significance, issues of antibacterial therapy // Attending Physician. 2002. No. 1-2. pp. 24-28.
- Karaulov A.V., Sokurenko S.I., Barmotin G.V. Principles of immunoprophylaxis and immunotherapy of recurrent respiratory diseases // MMA im. I. M. Sechenov, clinic of the Ministry of Foreign Affairs of the Russian Federation. M., 1999.
- Lazarev V.N. Adaptation reactions and their correction in chronic inflammatory diseases of the upper respiratory tract: Abstract of thesis. dis. ... doc. honey. Sci. M., 1995.
- Lopatin A. S. Treatment of acute and chronic pharyngitis // RMZh. 2001. T. 9. No. 16-17.
- Dagnelie CF Sore Throat in General Practice. A Diagnostic and Therapeutic Study. Thesis. Rotterdam, 1994.
- Rice D. H. Microbiology. In: Donald PJ, Gluckman JL, Rice DH Editors. The Sinuses. New York: Raven Press. 1995. pp. 57-64.
At the beginning of an exacerbation of chronic tonsillitis or in the postoperative period (after tonsillectomy), it makes sense to use topical antiseptics to accelerate the relief of inflammatory and pain symptoms in the oral cavity. In particular, the drug faringosept, which has a pronounced antiseptic effect and is available in the form of lozenges, has proven itself well. This ensures convenience and painlessness of its use, which is especially important in the postoperative period.
Diagnosis of tonsillitis
- For tonsillitis, the doctor will examine the child's throat, as well as his ears and nose, where there may also be inflammation.
- The doctor will examine the child's skin, since streptococcal sore throat sometimes causes a specific rash. This is what is called “scarlet fever” - it is not some kind of separate disease, but a sign of damage to the body by streptococcus.
- The doctor will feel the cervical lymph nodes - as a rule, with tonsillitis they swell.
- The doctor will feel the spleen to distinguish a sore throat from mononucleosis, which also causes swollen lymph nodes.
- The streptococcal test is a simple and accurate way to distinguish streptococcal tonsillitis from viral tonsillitis. The doctor takes a scraping from the child’s throat and within 24-48 hours the result is ready.
- In some cases, a general blood test may be needed, the results of which can also indicate the viral or bacterial nature of the disease. It is usually taken if the streptococcal test is negative, but the course of the disease leaves the doctor in doubt.
About the clinic
Euromed Clinic is a multidisciplinary family clinic in the center of St. Petersburg.
- Calling a doctor to your home
- 24/7 therapist appointment
- Tests, ultrasound, x-ray
- Whole body diagnostics
- Hospital and surgery
- Vaccination
Find out more about the clinic
Causes of tonsillitis
As a rule, the cause of the disease is bacteria and viruses (usually streptococcus). Typically, infection occurs through airborne droplets, especially when children are in large groups (kindergarten, school, various clubs and sports sections). If the causative agent of the disease is bacteria, you can become infected through dishes, a handshake, or through the patient’s personal items (towel, spoon). A child only needs to play with the toys of another sick child to become infected. Alas, acute tonsillitis is a highly contagious disease; and it is very easy to become infected with it.
Another cause of the disease is microorganisms that constantly live on the mucous membranes. This is the norm. A healthy body controls their amount and does not allow them to be exceeded. But as soon as the immune system weakens, the number of pathogenic microorganisms begins to increase: and in essence it turns out that the body infects itself. That is, the development of inflammation can occur with prolonged exposure to unfavorable factors on the child’s body that cause a decrease in immunity: dry indoor air, cigarette smoke, polluted air in big cities, etc.
Treatment of tonsillitis
The child should be provided with:
- peace and the opportunity to sleep as much as he wants;
- Drink plenty of fluids to relieve sore throats and prevent dehydration;
- air humidification;
- a sore throat can be relieved by both warm drinks and cold ice cream, especially popsicles;
- for a sore throat, it helps to gargle with a solution of table salt and soda - a teaspoon of salt and a small pinch of soda per 250 ml of warm water;
- Children over 4 years old can be offered lozenges for sore throats. Do not give candy to small children - they may choke;
- do not smoke when your child is sick, avoid strong odors that irritate the throat;
- A sore throat and fever can be relieved by medications containing paracetamol and ibuprofen. Don't give children aspirin; in rare cases, it can cause deadly Reye's syndrome.
Confirmed bacterial tonsillitis (usually streptococcal tonsillitis) is treated with antibiotics. It is dangerous to interrupt or stop the course because it increases the likelihood of infection spreading to the joints, heart, kidneys and other organs. Continue taking antibiotics even if your symptoms are completely gone.
Complications
It may seem that acute tonsillitis is a completely harmless disease. “Sore throat, fever - what’s wrong with that? A common manifestation of infection,” you say. But let us remember the nature of the disease. Its causative agent, streptococcus, can cause serious consequences.
Complications after tonsillitis can be divided into local (they are localized and noticeable in a certain area) and general (when changes affect the whole body).
Local ones include:
- paratonsillar and parapharyngeal abscess;
- mediastinitis (when a purulent infection descends into the heart sac);
- bleeding from the tonsils, provided that there were ulcers on their surface;
- otitis and eustacheitis (ENT organs are directly connected to each other, so an infection from the throat can easily migrate to the middle ear cavity, the auditory tube and cause an inflammatory process there);
- swelling of the larynx (with this condition, asphyxia develops. This condition is very dangerous, even fatal. A characteristic sign is a bluish tint of the skin against the background of severe suffocation);
- phlegmon and abscesses (purulent inflammation).
Common complications include diseases of the heart, kidneys, joints (rheumatism), tonsil intoxication and sepsis. In order to avoid dangerous consequences for the child’s body, it is very important to promptly begin the fight against tonsillitis under the supervision of a qualified otolaryngologist.
Friends! Timely and correct treatment will ensure you a speedy recovery!
Make an appointment right now!
Call us by phone or use the feedback form
Sign up
When should you see a doctor?
Even slightly enlarged tonsils in a child are a signal to contact a pediatric otolaryngologist. However, mild hypertrophy of the glands often does not manifest itself in any way, so it cannot be noticed visually. A visit to the doctor is required if the child, in addition to enlarged tonsils, has:
- classic signs of a cold: pain when swallowing, redness of the throat, cough, nasal congestion, fever, uncharacteristic weakness, headache;
- white plaque on the tonsils;
- swollen lymph nodes;
- pustules, ulcers in the larynx;
- swelling of the neck.